
Abstract
Introduction
The outbreak caused by SARS-CoV-2 virus, first detected in Wuhan, China,1–3 unleashed a worldwide pandemic, as stated by the World Health Organization (WHO) on March 11, 2020. 4 Nowadays, SARS-CoV-2 impacted every single country, with ∼100 million confirmed cases and almost ∼2.5 million deaths. 4 Spain was one of the first countries hit by this pandemic and Madrid the most devastated region accounting for up to ∼3 million cases and ∼70k deaths. 5
Orthopedic and trauma activity was dramatically modified in order to treat COVID-19 patients. 6 Surgeons had guidelines and recommendations changing continuously, as the whole country was adapting daily to this unprecedented situation, and sophisticated protective equipment was necessary for surgical practice.7–10 Elective surgery was suspended, and hip fractures were the most frequent orthopedic surgical procedure performed during SARS-CoV-2. 6 Elderly patients suffering from proximal femoral fractures were among the most vulnerable and also the most affected by the virus. 11 Higher mortality rate in hip fracture and SARS-CoV-2 disease was recently evidenced. 12 It remains unclear how clinical and functional outcomes in this group of patients were affected during this pandemic. The overcrowding and changes made to cope with this disease, as well as the stressful situation might have an impact in long-term outcomes.
The aim of this study is to describe our experience treating proximal femoral fractures in the epicenter of SARS-CoV-2 pandemic. We evaluated radiographic, clinical, and functional outcomes, comparing them to a standard situation during the same period in 2019. Our hypothesis is a decrease in hip fractures number during the quarantine period, increased mortality due to COVID-19 infection, but similar surgical results.
Materials and methods
Study design
An observational retrospective study analyzing the incidence and outcomes of hip fractures treated in two different scenarios was performed: pre and intra-epidemic SARS-CoV-2 at our hospital in Madrid, Spain. It is a public tertiary-level hospital, equivalent to a level I trauma center according to the American College of Surgeons classification. This specific period took place during the lockdown that associated confinement measures by the Spanish government, from March 15 to April 30, 2020. We treated both COVID and non-COVID patients during the lockdown. The same outcomes were evaluated and measured in patients during 2019. Patients suffering from an acute low energy hip fracture who attended our Emergency Department in the defined period were included. Patients younger than 50 years old diagnosed with pathological or periprosthetic fractures were excluded. Outcomes at short-term follow-up assessed 30 days after hospital discharge and at medium-term follow-up at 1 year were evaluated. Institutional review board approval was obtained and patients signed informed consent. In our center, since 2018, all hip fracture patients, signed an informed consent to be included in our hip fracture registry.
Data analyzed
Information was collected anonymously from our hospital database. 2019 patients were found using the hospital hip fracture registry.
Demographic data and baseline patients’ characteristics
Age, sex, habitual residence (family home or nursing home), medical records, comorbidities measured using the Charlson comorbidities index (CCI) including age, and ASA classification were collected. Regarding preoperative blood test, hemoglobin, albumin, and cholesterol were collected in order to detect differences in patients baseline status at the time of admission. Functional status was measured with functional ambulation classification (FAC) as it is used in the Spanish national hip fracture registry and it is validated for hip fractures patients. 13 Medium follow-up was 512 days from discharge in 2019 and 295 in 2020.
COVID-19 infection status
Hip fractures evaluated during the pandemic were divided into three groups according to their COVID-19 infection status regarding the SARS-CoV-2 novel coronavirus: positive, negative, and unknown if no test was performed. COVID-19 infection status was studied using the polymerase chain reaction (PCR) test (FluoroCycler XT, HAIN Lifescience, Nehren, Germany) at admission at the emergency room before hospitalization.
Fracture distribution
Fracture type was classified as intracapsular (femoral neck fractures) or extracapsular (intertrochanteric or subtrochantheric fractures). Extracapsular fractures were also divided into stable and unstable fracture patterns, according to AO criteria. 14 Data extraction and clinical and radiographic evaluation of eligible patients were performed by two individuals (FGS, SGC) with independent verification by a third reviewer (GLA). Disagreements were resolved by consensus or a fourth reviewer (EC) arbitration.
Surgical performance
Since surgery might have been hindered during the pandemic due to epidemiological conditions and due to the necessity of using protection equipment for all COVID-19 infected patients, surgery delay was defined as those procedures performed more than 48 hours after the fracture. All COVID-19 patients were operated even infected, but hemodynamically stable, then they were kept in isolation until PCR-COVID test was negative.
Surgical timing, the shift in which surgery was performed (from 8 Example of reduction measurement in a anteroposterior radiograph, analyzing both Tip-Apex distance and position of the cephalic screw in the femoral neck (inferior, middle or inferior). Example of varus–valgus stem position evaluation in a anteroposterior radiograph.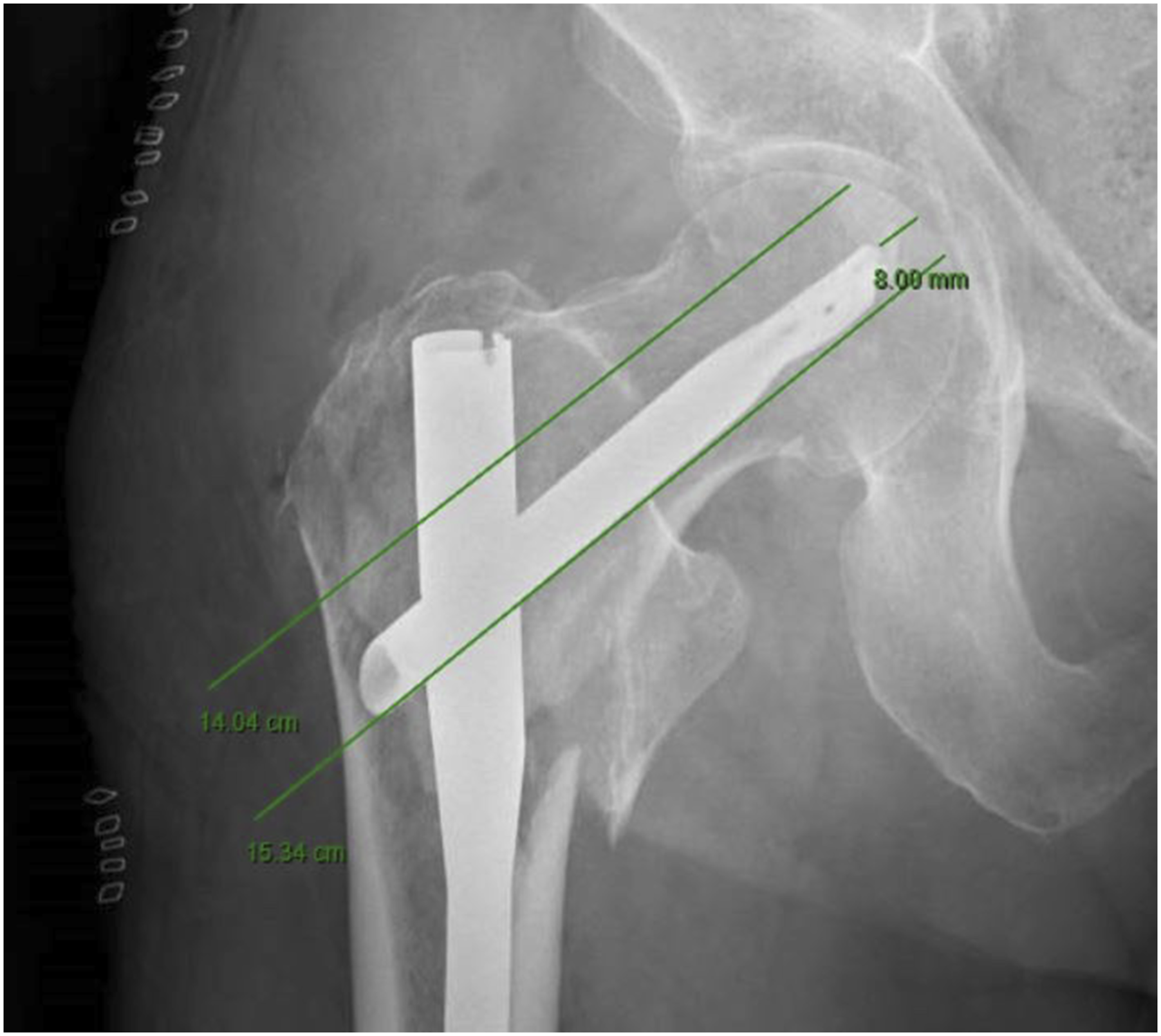

Postoperative outcomes
Time elapsed from trauma to emergency department attendance, hospital stay, discharge destination (home or nursing home), visits to the emergency room or any hospitalization event that occurred during the first postoperative 30 days, and mortality were recorded at 30 days and 1 year. Functional ambulation recovery information using the FAC (functional ambulation classification) scale was also collected within our follow-up period in order to evaluate the impact of the lockdown in these patients considering that no physiotherapy could be provided in the immediate postoperative period (Figure 3).
13
In addition, medical complications in patients treated in both periods were recorded and functional outcomes of COVID-19 patients were compared to those who were not infected in 2020. Functional ambulation classification (FAC) scale.
Statistical analysis
Relevant data were inserted into an electronic database (Microsoft® Excel for Windows® (Microsoft Corp, Redmond, WA) for further analysis. Mean and standard deviation were used to describe quantitative variables, median was used for ordinal variables, and frequency and percentage for qualitative variables. Statistical differences were assessed using Student t-test, chi-square test, Wilcoxon, and Mann–Withney tests. Data analysis was carried out using IBM SPSS version 24.0 (IBM SPSS, Armonk, NY, USA), and significance of pooled estimates was set at P < .05. A total of 146 fractures were analyzed: 89 fractures in 2019 (∼60%) and 57 (∼40%) in SARS-CoV-2 pandemic
Results
Demographic and preoperative variables.

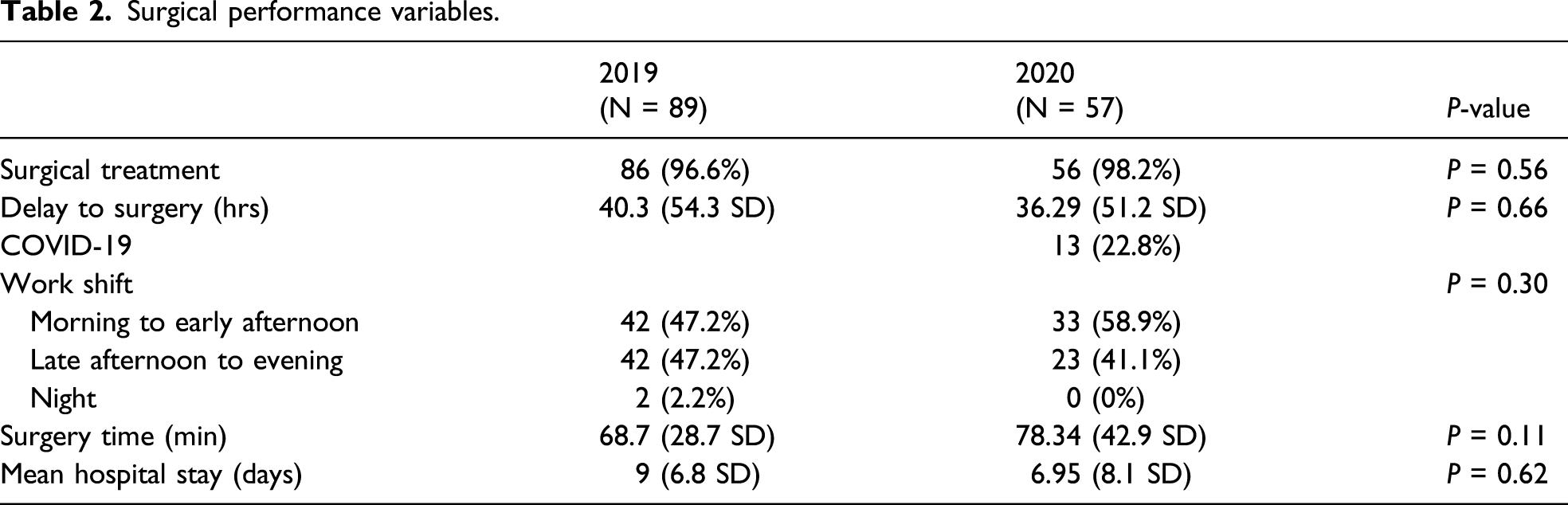
Surgical performance variables.
Extracapsular fracture patterns.

Surgical performance in extracapsular fractures. 14

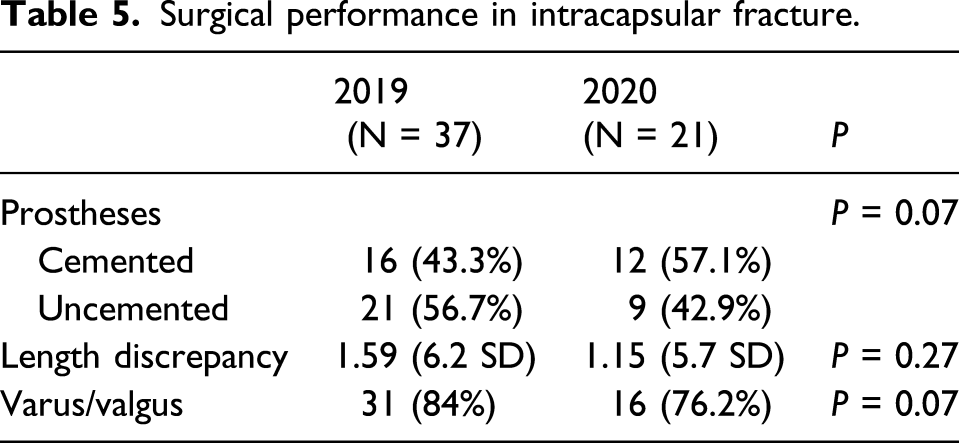
Surgical performance in intracapsular fracture.
Postoperative outcomes
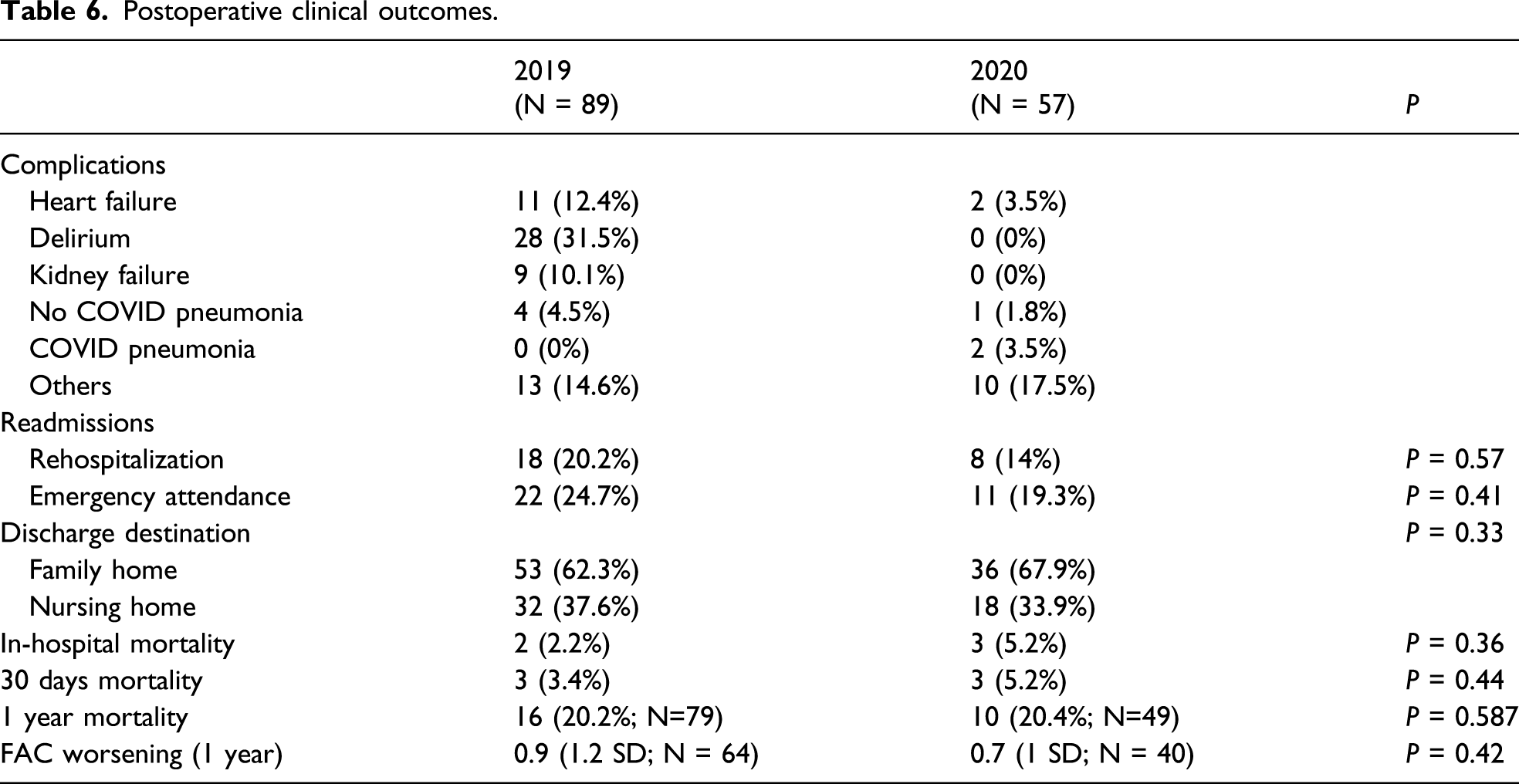
Postoperative clinical outcomes.
Outcomes in COVID-19 tested patients.

Discussion
We found a hip fracture incidence decrease during the SARS-CoV-2 pandemic, contrary to recently published works.12,14 Difficult conditions in which patients were treated were associated neither with worse surgical performance nor significant higher mortality or differences in functional recovery.
A different hip fracture incidence could be reasonably explained by the confinement measures during those months. Due to home lockdown, people’s physical activity decreased sharply, particularly for the elderly and at nursing homes, reducing falls and injuries. Fear of infection could be a delay factor for certain pathologies but not for hip fractures that are extremely painful and completely disabling. There is a possibility that patients attended other hospitals in our city; however, this is highly unlikely as transfers are scheduled based on where patients live, so patients do not decide which hospital to go to.
Despite this change, fracture pattern distribution did not suffer changes during the pandemic. Similarly, no significant differences were found between patients’ habitual residence either, nor their preoperative variables such as blood tests (hemoglobin and cholesterol), Charlson comorbidity index and pre-fracture functional scores. There were statistically differences in albumin levels that could explain patients during quarantine presented higher malnutrition status. We received fewer patients but with no important differences.
Regarding fracture management, we did not find differences in the overall time delay from admission to surgery, except for those patients in whom PCR tests were positive for COVID-19, who required to be scheduled in specific operating and recovery rooms following strict epidemiological recommendations. On the other hand, the number of patients operated during the morning shift increased because there were more operating rooms available since elective surgery had been suspended. This could lead to a better surgery performance with better preoperative preparation and rested surgeons. The team of surgeons was similar in both scenarios, since residents operated most hip fractures.
Although not significant statistically, we also observed a clear decreasing trend in hospital stay in 2020, as recently reported.6,17 Confinement has increased family support for these patients and they played a key-role by taking care of them after discharge, coupled with the fear of SARS-CoV-2 in-hospital infection might explain this finding.
SARS-CoV-2 threatened health systems generating a serious concern for governments and individuals around the world.5,6,10,13 The lockdown has been a stressful situation, but particularly for health-care workers. In this study, we analyzed for the first time the potential impact of the pandemic on the surgical performance when operating hip fractures. This stress has been especially acute operating on COVID-19 patients, a novel situation for everyone that implied working in a special operating room, following strict protocols, and bearing uncomfortable personal protective equipment. In spite of this condition that might have hindered surgical performance, radiographic results were comparable with those in 2019. Furthermore, a significantly superior number of cases with a central position of the screw in the femoral head and a higher rate of satisfactory calcar reduction in extracapsular hip fractures were detected. Interestingly, this superior performance was achieved without requiring a superior operative time. We cannot give a clear satisfactory explanation for this finding, but the high level of responsibility and motivation of the surgical team to address this frequent procedure under stressful conditions seemed to have overcome difficulties, and better results in certain variables analyzed were obtained.
Mortality rates increased in our cohort at the short time, without being statistically significant, and were similar at 1-year follow-up, which is in line with other published studies. 17 Contrary, most studies found major increased mortality in COVID patients at short time.18–21 We may fail to achieve statistical signification due to low sample size mainly. Re-entry rate and emergency attendance at 30 days decreased, but no statistical significance was observed.
Another interesting finding is the lack of differences in the degree of functional recovery according to the FAC scale. Although no physical therapy treatment was provided in the hospital during the lockdown, functional outcomes based on FAC scale were not significantly worse.
Regarding patients with a positive PCR test for SARS-CoV-2 in 2020, and compared to the rest of the patients that suffered a hip fracture during this period, they showed more complications and rehospitalization events and an increase in average stay, as previously reported. 12 Differences were not statistically significant in this study probably due to the small sample size, and therefore, no conclusions should be drawn.
This investigation provides data on the management of proximal femoral fractures in a Department of Orthopedics and Traumatology at a hospital at the epicenter of SARS-CoV-2 pandemic in Europe. To our knowledge, this is the first investigation that takes into account not only medical variables but also surgical performance in a global pandemic scenario, with 1-year follow-up. This study has several drawbacks. Our main limitation was the low sample size as stated previously, which could underestimate our results. Although a 1-year follow-up is not enough to evaluate certain surgery complications as peri-implant fracture, it is the longest follow-up available for COVID infection at this moment.
Information on the status with regard to the infection by SARS-CoV-2 could be registered in the majority, but not all patients were treated in 2020; we only found 13 COVID-19 positive patients. In addition, as a retrospective study, we have several inherent limitations like missing information and patient follow-up loss
In summary, the decrease of hip fracture during the confinement has been a fact in our area, yet the management of proximal femoral fractures has been successful, with comparable result at 1-year follow-up with pre-pandemic clinical practice, despite the global emergency, and every patient received appropriate surgical treatment, even when all efforts were focused in SARS-CoV-2 patients and pandemic control.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.