
Abstract
Introduction
In the background of the aging population, an increase of geriatric patients with specific age-related co-morbidities has already been seen over the years for proximal femur fractures in orthopaedic surgery as well as other medical disciplines. However, the geriatric aspect has not been well recognized in periprosthetic joint infection (PJI) patients so far. Therefore, this paper seeks to provide an overview on the co-morbidities of PJI patients with respect to the definition of geriatric patients.
Material and methods
In this single-center retrospective study, patients treated between 2007 and 2020 for PJI were included (n = 255). Patients were defined as geriatric according to the consensus definition criteria of the Federal Working Group of Clinical Geriatric Facilities e.V., the German Society for Geriatrics e.V. and the German Society for Gerontology and Geriatrics e.V. based on age (≤70 years), geriatric multimorbidity and the Barthel index (≤30).
Results
Applying the criteria defined 184 of the 255 (72.2%) PJI patients as geriatric infection patients. Regarding geriatric comorbidity, incontinence was most prevalent (38.1%), followed by immobility (25.6%). Comparing the geriatric infection patients with those classified as non-geriatric (n = 71
Discussion
We propose to use the term orthogeriatric infection patients in those cases in order to focus treatment not only on the orthopaedic infections but also on the important geriatric aspects.
Conclusion
The inclusion of geriatric physicians into the multidisciplinary team approach for PJI patients might be beneficial.
Keywords
Introduction
The term “geriatric orthopaedics” was firstly coined in 1974 by Michael Davis, who ran an orthogeriatric service with Bob Irvine in the Hasting Clinics in the UK. 1 Due to the aging population, the field of geriatric orthopedics gained importance and has been grown in recent years. 2 However, the focus has been primarily set on fragility fractures and the specific needs of the elderly requiring a comprehensive approach to care.2,3 For instance, it has been shown that elderly patients with fragility fractures benefit from a multidisciplinary treatment including geriatric assessment.4-6 Further, treating patients undergoing elective surgery aged 65 years with a team including a consultant geriatrician, nurse specialist in older people, occupational therapist, physiotherapist and social worker was reported to reduce postsurgical complications and length of hospital stay. 7 Nevertheless, besides osteoporosis, also the prevalence of other musculoskeletal diseases increases with age such as osteoarthritis, which has been ranked as the 11th highest contributor to global disability in 2010. 8 For end stage osteoarthritis, joint replacement as a life-enhancing procedure is often the therapy choice. It was estimated that 80% of total hip arthroplasty (THA) and 96% of total knee arthroplasty (TKA) surgeries are due to osteoarthritis. 9 In Germany, primary total knee or hip arthroplasty is among the most common procedures, with an increase in the number of surgeries of up to 45% predicted for the year 2040. 10 Periprosthetic joint infection (PJI) is a dreaded complication in orthopaedics and trauma surgery with an incidence of 24/1 000 000 inhabitants in Germany. 11 Hence, an increasing percentage of older patients with bone and joint infection is expectable.
Whereas there is no major differences in the pathogenesis and etiology of PJI between the adult and the geriatric population is evidenced, 12 several studies suggest that elderly patients have a higher risk of adverse outcomes after revision total joint arthroplasty.13,14 Hereby, the functional status of the patients plays a major role 15 and comorbidities such as congestive heart failure, chronic pulmonary disease, preoperative anaemia, diabetes and depression increase the risk for a subsequent infection. 16 Also, lower success rates after 2-stage exchange arthroplasty have been reported in immunocompromised hosts 17 as well as an increased PJI-related mortality rate in older patients. 18
Therefore, we suggest expanding the current field of orthogeriatrics to include PJI as host optimisation plays a key role in the treatment of this specific patient population and the incorporation of comprehensive geriatric assessment could reduce complication rates, and improve the outcome and patients’ quality of life. For this purpose, it was aimed at providing an overview of the current situation, classifying PJI patients treated in our department as geriatric infection patients by age, Barthel index and comorbidities to evaluate the value of the term “orthogeriatric infection” in this context.
Material and Methods
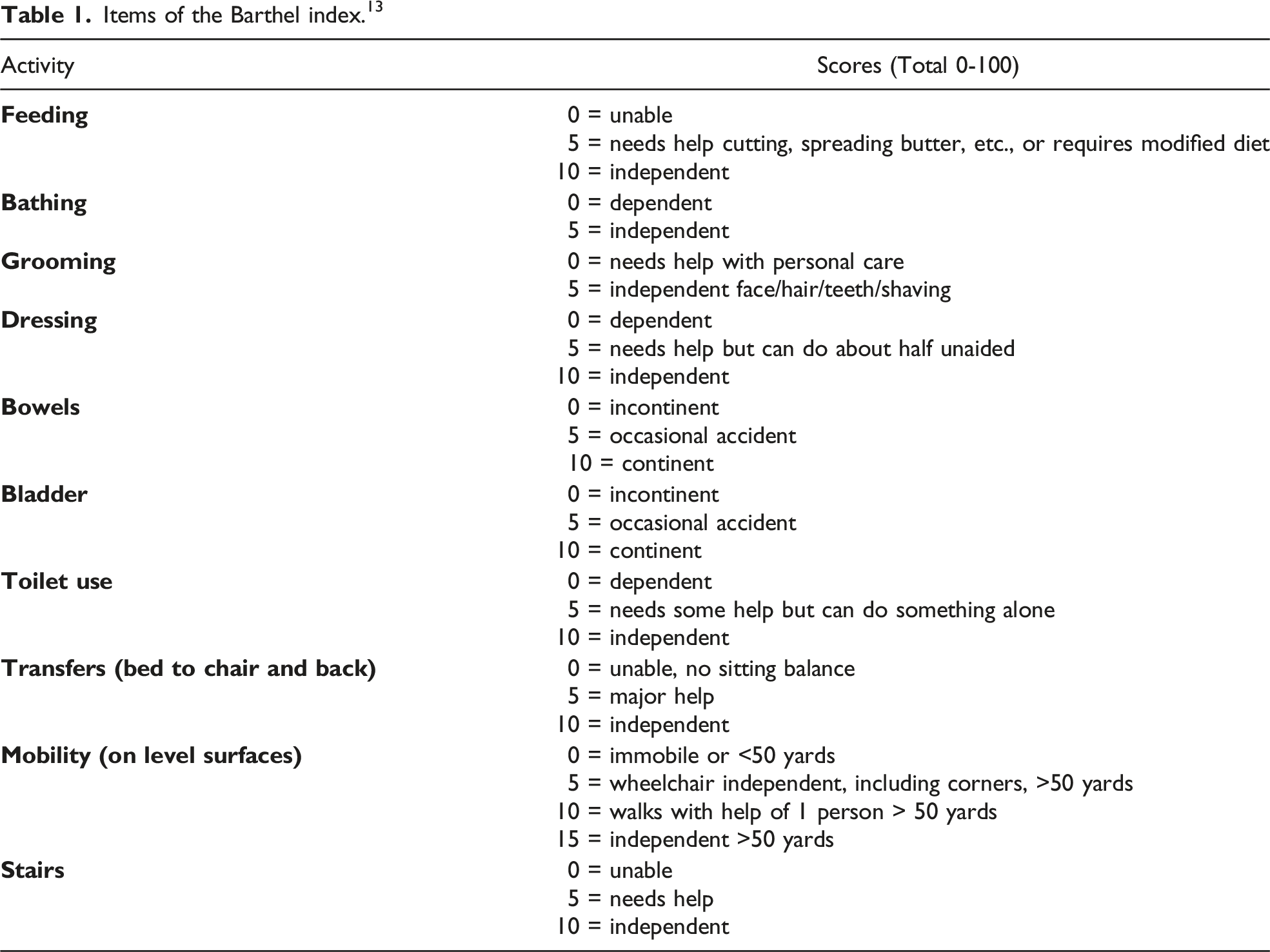
Items of the Barthel index. 13
Results
In total, 255 patients were identified (56.1% males) with PJI of the shoulder (7.0%), the hip (45.5%) and the knee (47.5%). The mean age was 70.7 ± 10.7 years [36-91], whereby 49 patients (19.2%) were older than 80 years and 154 patients (60.4%) were older than 70 years. The mean CCI was 2.5 ± 2.3 (range: 0-11). On average patients were hospitalized for 42.6 ± 34.8 days (range: 12-208 days). The Barthel index is a toll to assess daily living activities and mobility, such as urinal or fecal incontinence, help needed for feeding and walking etc. with a total score between 0 and 100 representing severely impaired and normal daily activities, respectively. The mean Barthel index was 40.2 ± 26.8, whereby n = 68 (26.7%) patients had a Barthel index in the range of 0-15 (Figure 1). A Barthel index ≤30 was recorded in 44.3% (n = 113) of the patients. Distribution of the Barthel-index.
Distribution of the Geriatric Multimorbidity.

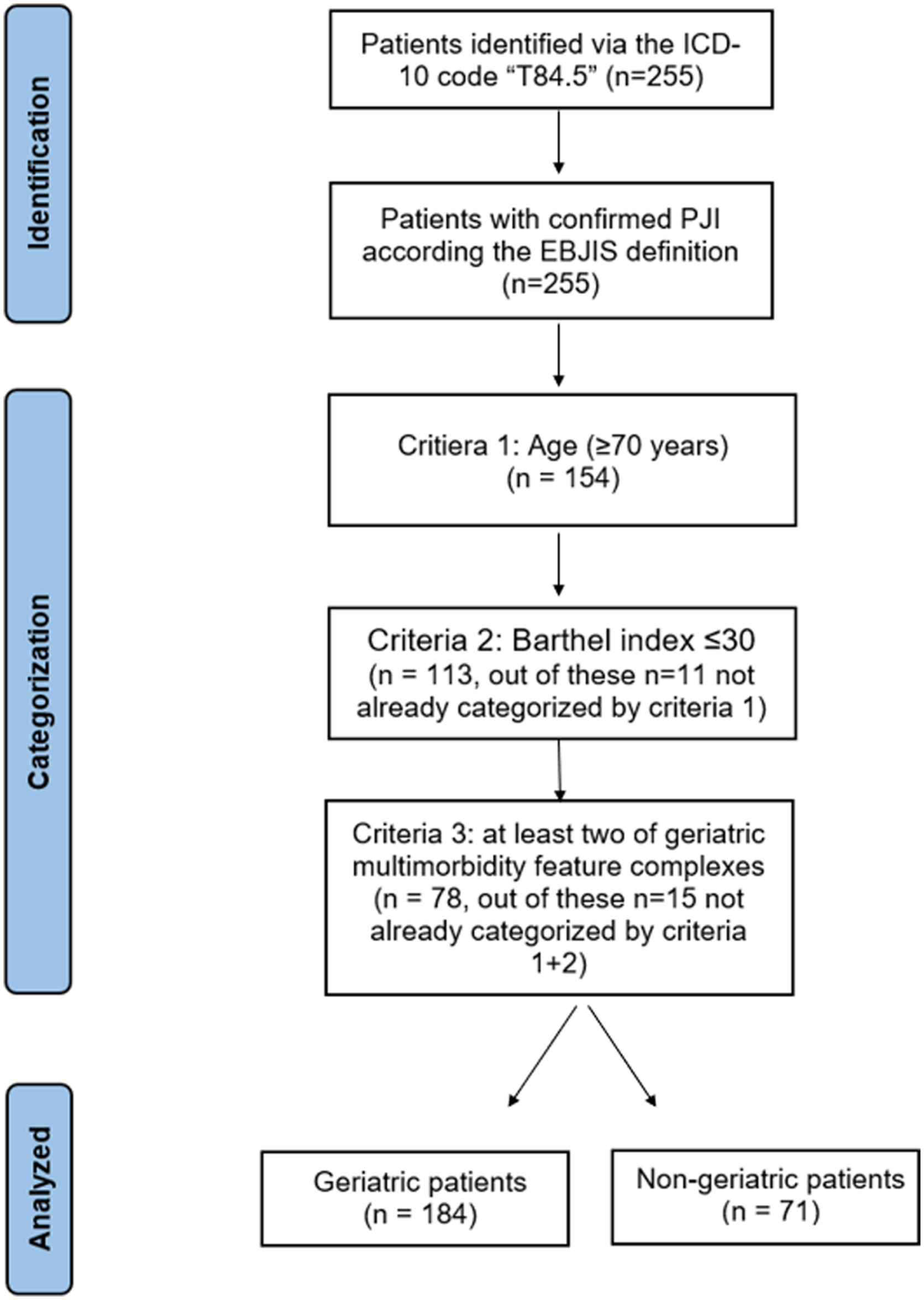
Schematic overview of the categorization process.
Patient Characteristics and Outcomes Divided in the Geriatric and Non-Geriatric Population. *P ≤ .05.
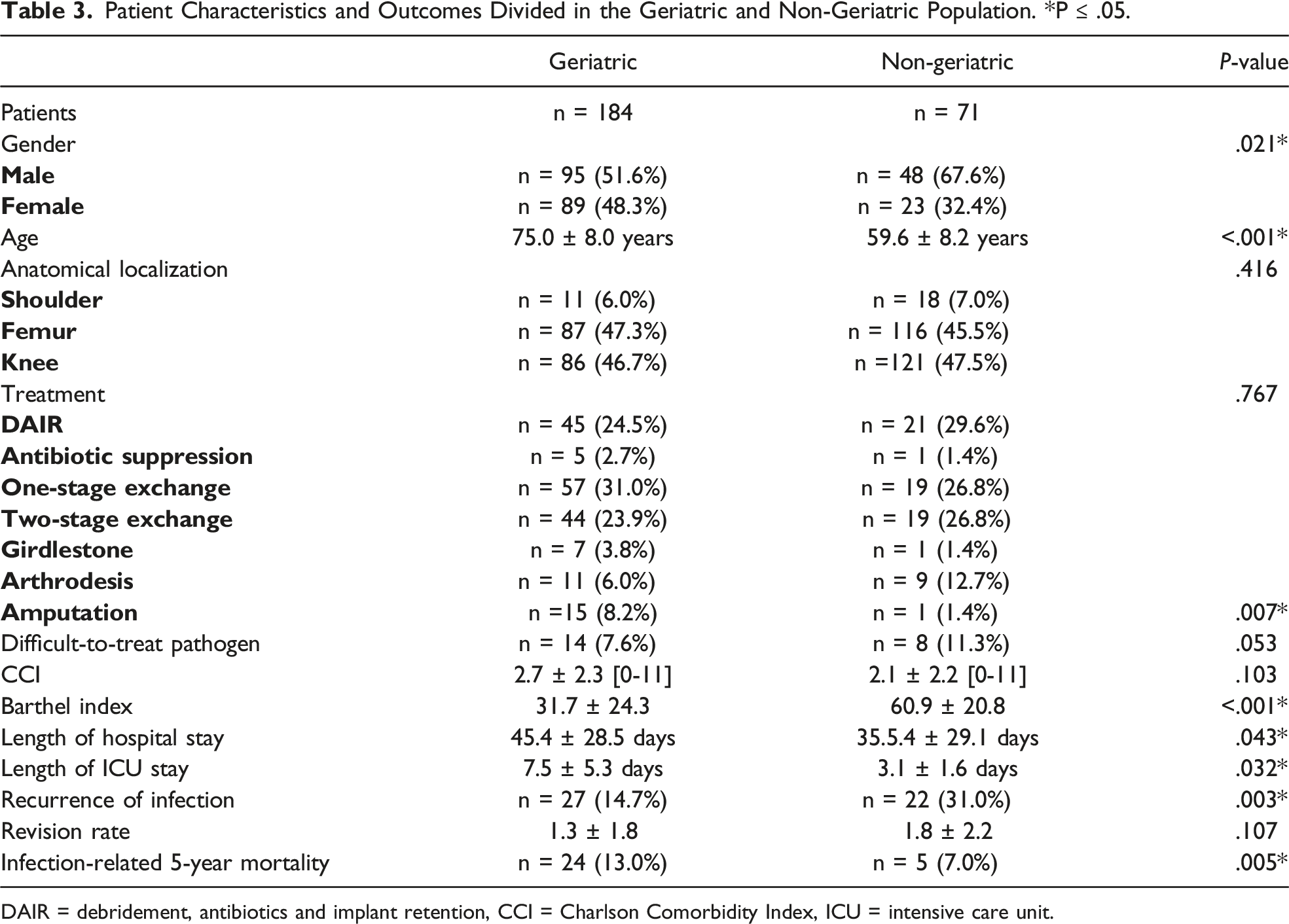
DAIR = debridement, antibiotics and implant retention, CCI = Charlson Comorbidity Index, ICU = intensive care unit.
Discussion
The purpose of this study was to introduce a definition of the term “orthogeriatric infection”. Here, 72.2% of all PJI patients were categorized as geriatric infection patients. Based on the consensus definition criteria of the Federal Working Group of Clinical Geriatric Facilities e.V., the German Society for Geriatrics e.V. and the German Society for Gerontology and Geriatrics e.V., 22 age of ≥70 years was chosen for the classification of patients. However, the heterogeneity of the definition of elderly age in orthopedic research has been highlighted. 23 In a meta-analysis including 80 studies and 271 470 patients it was shown that 95% of the studies defined elderly age solely based on chronology with a range from 50 to 80 years, whereby 65 years was most commonly used as a cutoff (47.5%). Therefore, including a fraility index is deemed beneficial for an improved approach in orthopaedic research focusing on the elderly. 23 Here, the Barthel index was applied, which has a sufficient structural validity, reliability, and interpretability and depicts a valuable tool to assess the ability to perform daily activities, especially in geriatric patients. 24 The Barthel index was shown to have a strong and independent association with mortality in geriatric patients. 25 Especially in patients with hip fractures, a lower Barthel index was associated with increased mortality serving as an independent risk factor,26,27 which is in line with our findings of a significant association between the Barthel index and the mortality rate in the present cohort. Also, lower Barthel indices were determined in patients with fracture-related infection of the hip compared with a matched control group without infection. 28 A recent study conducted in Spain collected the Barthel scores in 2 nursing homes before and after an infection with Covid-19. In their cohort (mean age 85.9 ± 6.42, 34 male/34 female) the post Covid Barthel total score was 52.30 ± 27.22 (44.56-60.04), which was higher than in the cohort analyzed here (40.2 ± 26.8), emphasizing the burden of PJI. 29 Further, the geriatric multimorbidity was considered. The results showed that patients were diagnosed with 2.7 ± .9 multimorbidity feature complexes on average and that incontinence (38.1%) and immobility (25.6%) were the most prevalent. Also here, heterogeneity in the literature can be noted. For instance, a recent meta-analysis reported a prevalence of delirium among orthopedic surgery patients between 4.5% and 41.2%. 30 Vetrano et al. investigated geriatric syndromes in 6903 participants presented with an average of 2.0 geriatric symptoms with pain (48%), urinary incontinence (47%) and falls (33%) being the most prevalent. 31 Another study conducted in France analysed geriatric symptoms in people aged 75 years and older reported that the most frequent geriatric syndromes were polypharmacy (50.6%, 95%CI = 46.7-54.5) and falls (43.1%, 95%CI = 38.4-46.1). Whereas here no significant association between the type of feature complex (e.g immobility and incontinence) was found, in general, comorbidity of the patients plays an essential role in the treatment and prognosis for PJI. Therefore, also considering the higher amputation rate reported in this study in the geriatric population, alternatives therapy strategies for elderly patients with PJI who would not benefit or survive surgical treatment have to be addressed. 32 For instance, Prendki et al. recorded that 60% of (n = 38) patients in the age range 80-95 years remained event-free during 2 years of prolonged suppressive antibiotic therapy., 33 Other authors have shown a high success rate (84% of n = 26 patients) for prolonged antibiotic suppression therapy. 34 Additionally, a significantly higher infection-related mortality rate was found in the geriatric population, which is in line with other findings showing that PJI-related death is more common in older patients (6.5% vs .8%, P < .05). 18
Thus, to achieve the best outcome for the patient, interdisciplinary approaches and early involvement of multidisciplinary teams are deemed important. For instance, it was demonstrated that patients treated for PJI of the hip had a shorter in-hospital stay, reduced numbers of surgeries and less antibiotics when discussed with a multidisciplinary team. 35 In addition, Bauer et al. analyzed files of patients treated for bone and joint infection before and after the implementation of a multidisciplinary staff meeting, reporting optimized adaptation of antibiotic therapy. 36 A similar approach with valuable clinical experiences is reported by Carlson and colleagues with a collaboration between infectious disease clinicians and orthopaedic arthroplasty surgeons to optimize PJI treatment. 37 Recently, also raising numbers of psychological comorbidities over the years have been shown for PJI patients, whereby the authors concluded that interdisciplinary collaboration is warranted and a psychologists should be included in the management. 11 In light of the presented findings, routine geriatric screening assessment should be considered. Further, the high number of geriatric infection patients (72.2%) emphasizes that geriatric physicians should be included as part of the PJI treatment team.
The study shows limitations. The first depicts its retrospective design, which did not allow to present longitudinal changes of the Barthel index. Further, correct coding of the comorbidities was assumed, although it is not fully assured.
In conclusion, to prepare for the changing demographics among bone and joint infection patients, geriatric infection-oriented trainings should be provided to improve patient’s quality of life, surgical outcomes, and reduce healthcare cost. Interdisciplinary collaborations among orthopaedic surgeons, geriatric physicians, physiotherapists and psychologists should be strengthened. Decision makers in healthcare systems should support future efforts to enhance not only the quantity but quality of life of patients with geriatric bone and joint infections.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
The study was approved by the institutional ethics committee of the XX (file number 20-1681-104). and conducted according to the World medical Association Declaration of Helsinki.
Data Availability
The data that support the findings of this study are available on request from the corresponding author, V.A.