
Abstract
Objective
To discover the key evaluation tool of the cephalic fixation position for predicting implant failures in geriatric intertrochanteric fracture (ITF) patients treated with internal fixations after achieving an acceptable reduction.
Methods
We measured the geriatric ITF patients undergoing single-screw cephalomedullary nailing (CMN) fixation surgery after obtaining the acceptable reduction (including anatomical reduction and positive medial cortex support reduction) in our treatment group between September 2016 and March 2020 by using four kinds of cephalic fixation position evaluation tools including Cleveland zone system, Parker’s ratio index, tip–apex distance (TAD), calcar-referenced TAD (CalTAD), and analyzed which were the key evaluation tools for measurement of cephalic fixation position for prediction of implant failures in geriatric ITF patients with internal fixations.
Results
Seventy-four ITF patients treated with single-screw CMN fixation after obtaining the acceptable reduction were enrolled in this study. Of the 74 patients, nine cases were observed with implant failures. There were six cases of cut-out and three of pending cut-out. We found that TAD (odds ratio (OR)=1.149; 95% confidence interval (CI), 1.00–1.32; P=.046) and CalTAD (OR=1.140; 95% CI, 1.00–1.30; P=.037) were risk factors for implant failures by univariate analysis, while only CalTAD (OR=1.200; 95% CI, 1.032–1.395; P=.018) was the independent risk factor for implant failures by multivariate analysis. The Kappa coefficient (κ) of CalTAD was .976 (95% CI, .966–.984) by ICC analysis. The ROC analysis showed that the best cut-off value of CalTAD was 23.76 mm with a sensitivity of 77.8% and specificity of 72.3% (area under the curve, AUC =.775; P = .001).
Conclusions
CalTAD is the key evaluation tool for measurement of cephalic fixation position for predicting implant failures in geriatric ITF patients treated with single-screw CMN after obtaining the acceptable reduction.
Keywords
Introduction
With the aging population increasing globally, intertrochanteric fracture (ITF), which leads to numerous morbidity, mortality, and financial burden to family and society, are on rising every year with an expected incidence of 4.5 million in 2050. 1
Usually, ITF is treated with internal fixation because internal fixation can reduce mortality, relieve pain and improve the quality of daily life. 2 Although internal fixation devices and operative techniques have been developed rapidly, implant failure in ITF patients is still widely reported with the failure rate varying from 3.2% to 20.5%.2-10 Thus, how to prevent implant failures is critical to geriatric ITF patients.
No doubt, the causes of implant failures in ITF patients are multi-factorial. Usually, bone quality, fracture severity, reduction quality, fixation type, and fixation position are the risk factors of implant failure in ITF patients. Unfortunately, what we can change are only the quality of reduction, the type of fixation, and the position of fixation. Therefore, we should do our best to achieve good reduction, select suitable fixation, and put the fixation in right place.
Of course, reduction quality is the first importance in ITF internal fixation. If the reduction is poor, the implant tends to fail. It is well known that reduction, particularly the medial cortex reduction, is the most important factor for preventing implant failures in ITF patients.5,7,11-14 However, there are only three kinds of reductions of ITF (Figure 1): anatomical reduction (Figure 1(a)), positive medial cortex support reduction (Figure 1(b)), and negative medial cortex support reduction (NMCS reduction, Figure 1(c)). Since anatomical reduction and positive medial cortex support reduction can result in better biomechanical effects and clinical outcomes,7,11 we can consider these two kinds of reductions as acceptable reductions. Therefore, we commonly attempt to obtain an acceptable reduction at least. Indeed, we tend to restore the exact cortical contact by reaching the anatomical reduction during surgeries rather than merely achieve positive medial cortex support reduction. Three kinds of medial wall reduction. Anatomical reduction: the cortex of proximal fragment and distal shaft fragment contacted smoothly (a). Positive medial cortex support (PMCS): The proximal cortex displaced medially to the upper edge of distal cortex (b). Negative medial cortex support (NMCS): The proximal cortex displaced laterally to the upper edge of distal cortex (c). Both Anatomical reduction and PMCS are called as acceptable reduction (a, b).
However, implant failures still happen even in the cases with the acceptable reduction. The failures are mostly contributed by both fixation selection and fixation position. Nowadays, the cephalomedullary nail (CMN) with a lag-screw or a helical blade is the most used for ITF treatment; therefore, the cephalic fixation position is the most important role to prevent implant failures if we treat our ITF patients with CMN after obtaining an acceptable reduction.
Unfortunately, we are usually confused because there are so many studies on evaluation tools of cephalic fixation position including Cleveland zone system, 15 Parker’s ratio index, 8 tip–apex distance (TAD), 9 calcar-referenced TAD (CalTAD), 10 and all of the tools are so important in their studies. However, little discussion about which tool is the key tool of cephalic fixation position for predicting implant failures in ITF patients with internal fixation after obtaining an acceptable reduction in published literature. Although Kashigar indicated that CalTAD was the only significant risk factor for the cut-out in CMN fixation, there were 33 (43%) patients with poor reduction in their study. 10
So we hypotheses that there should be a key tool among these evaluation tools which can predict implant failures of ITF patients with internal fixation after achieving acceptable reduction. If we discover the key evaluation tool, we may avoid implant failures in geriatric ITF patients with internal fixation.
Therefore, the purpose of this study is to identify the key evaluation tool of cephalic fixation position for prediction of implant failures in geriatric ITF patients undergoing single-screw CMN internal fixation after obtaining an acceptable reduction. We find that CalTAD is the key evaluation tool of cephalic fixation position for prediction of implant failures in geriatric ITF patients treated with single-screw CMN internal fixation after obtaining an acceptable reduction.
Methods
This study was approved by the Ethics Committee of Guangzhou First People’s Hospital. Clinical and radiological data were collected from the Hospital Information System (HIS) in our hospital. The inclusion criteria of this present study were the patients: (1) diagnosed as ITF, (2) with internal fixation, (3) underwent surgeries in our treatment group between September 2016 and March 2020. And the exclusion criteria were the patients: (1) aged less than 65 years, (2) with pathological fracture, (3) without preoperative X-ray radiographs, (4) with none of single-screw CMN internal fixation, (5) with NMCS reduction intraoperatively, and (6) without any implant failures while radiographic follow-up less than 90 days. (Figure 2) Flow of patients through the study.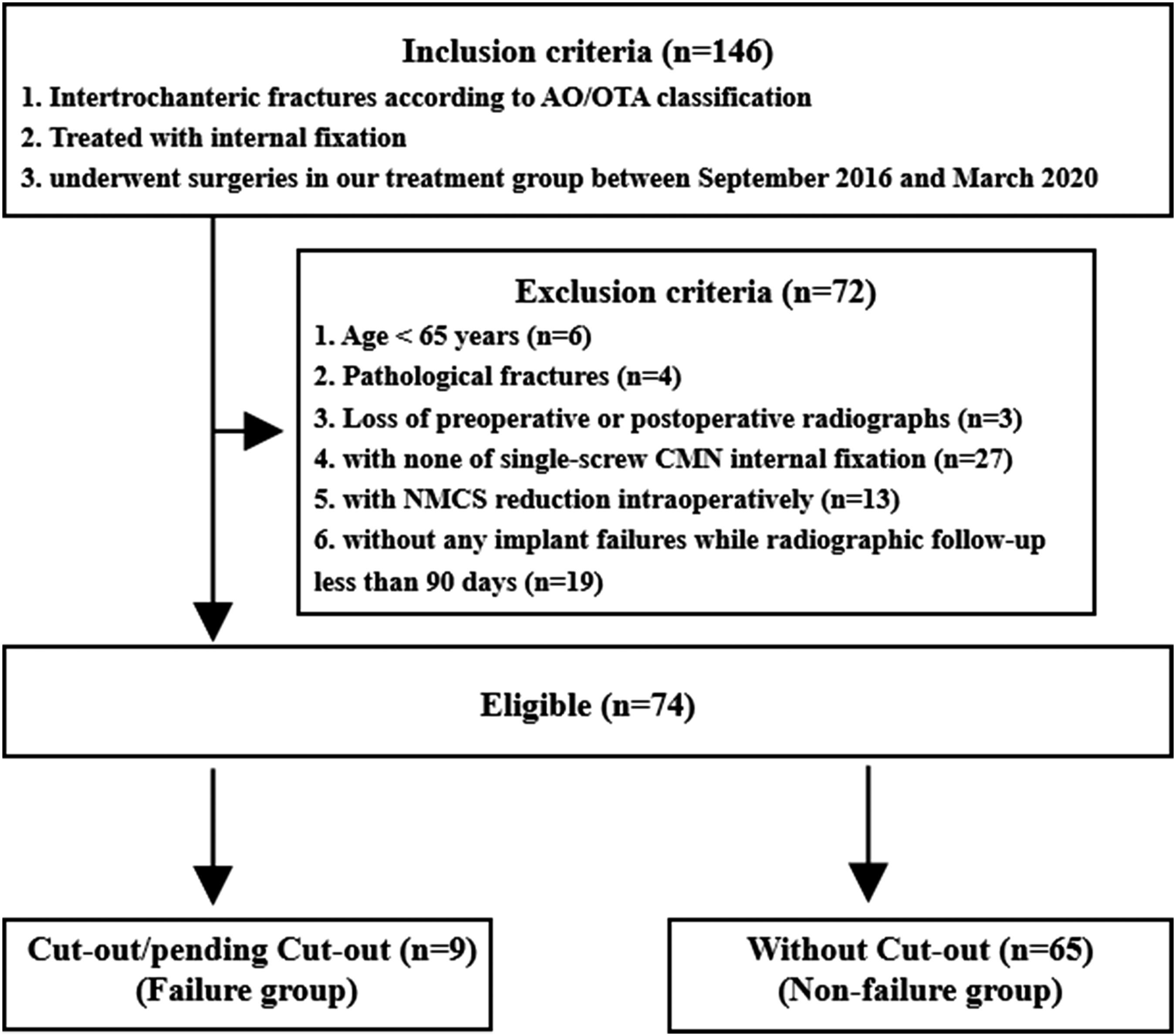
Clinical data including age, gender, fracture site, fracture type, Singh index, American Society of Anesthesiologists (ASA) classification, New York Heart Association (NYHA) classification, anesthesia, fixation type, and cephalic nail position were analyzed.
Radiological parameters were obtained from preoperative, intraoperative, or the first postoperative X-ray and radiographic follow-ups. The fractures were graded based on the AO/OTA classification (2018 version). 16 Singh Index was used to evaluate osteoporotic degree on the preoperative anteroposterior (AP) view. 17
The cephalic nail position was evaluated by four kind evaluation tools including tip–apex distance (TAD), 9 calcar-referenced TAD (CalTAD), 10 Cleveland zone system), 15 and Parker’ 8 s ratio index on AP and lateral views.
Implant failures included cut-out and varus deformity (pending cut-out). Cut-out was extrusion of the cephalic nail from the superior femoral head. Pending cut-out was the presence of over 15° decrease of neck-shaft angle (NSA) without penetration or cut-out of the cephalic nail on the AP view in the last radiographic follow-up compared with the NSA on the AP view in the first radiograph right after surgeries. Non-implant failure was the presence of the radiological bone union without implant failures after surgery.
All calibrations were performed using Digimizer (version 5.4.4 MedCalc Software) by referencing cephalic nails diameter. And all parameters were measured by an orthopedist (Jian-wen Huang) three times in one-month intervals. The median reliability for the radiological measurement is .907 (range, .725–.958), which indicated excellent intraobserver reliability.
Statistical Analysis
With the occurrence of implant failures as the dependent variable, Student’s t-test or Mann–Whitney U test was used for the continuous variables and chi-square test for the categorical variables, respectively. A univariate logistics regression was used for crude odds ratio (OR) with a 95% confidence interval (CI).
Four kinds of cephalic fixation position evaluation tools including the Cleveland zone system, Parker’s ratio index, TAD, and CalTAD were entered in multivariate analysis with a backward likelihood ratio method for the best model. All variables at multivariate analysis were analyzed for the intraclass correlation coefficient (ICC) for continuous variables and with κ coefficients for categorical variables, respectively. 18 A one-way random-effects model with 95% CI was performed to obtain the average measures ICC. And κ coefficients were calculated with 95% CI. Receiver-Operating Characteristic (ROC) curve was used for the best cut-off value of the significant continuous variable at multivariate analysis.
All analyses were performed using SPSS (IBM SPSS Statistic for Windows, Version 25.0. Armonk, NY: IBM Corp). All tests were two-sided and the P-value below .05 was considered statistically significant.
Results
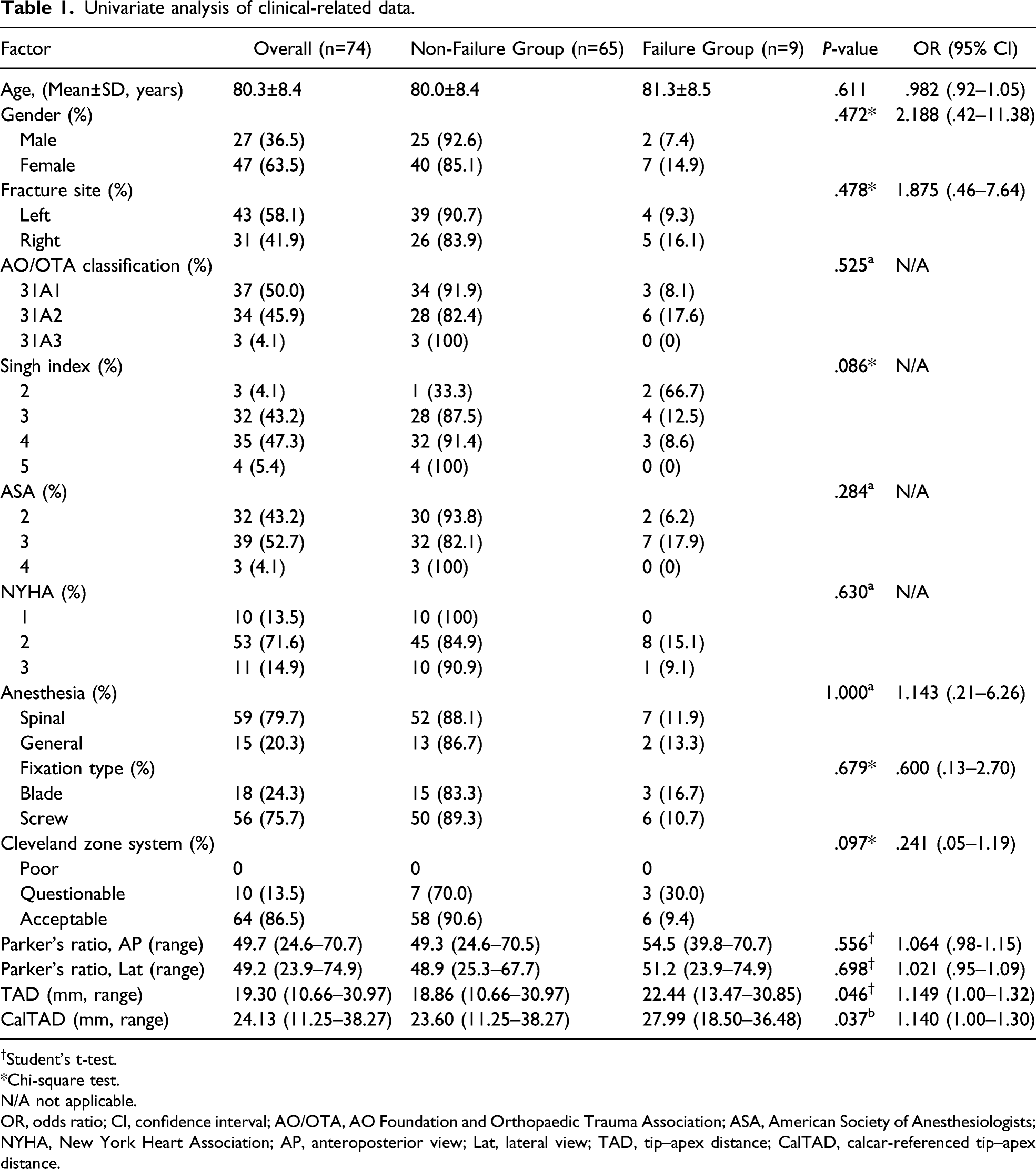
Univariate analysis of clinical-related data.
†Student’s t-test.
*Chi-square test.
N/A not applicable.
OR, odds ratio; CI, confidence interval; AO/OTA, AO Foundation and Orthopaedic Trauma Association; ASA, American Society of Anesthesiologists; NYHA, New York Heart Association; AP, anteroposterior view; Lat, lateral view; TAD, tip–apex distance; CalTAD, calcar-referenced tip–apex distance.
In the operative factors, no significances were found except TAD (P=.046) and CalTAD (P=.037) utilizing univariate analysis (Table 1). Cephalic fixation was located in six of the nine zones within the femoral head based on the Cleveland zone system. Overall, no case was observed with the poor placement while 10 with questionable (13.5%) and 64 with acceptable (86.5%). Most of the nail position was in Zone 5 (44/74), of which four cases suffered from implant failures. The failure rate was highest (50%) in Both Zone 3 and Zone 4 while lowest in Zone 8 (5.9%), but the difference in the cephalic nails position was not significant between the two groups (P=.097). Similarly, there were no significant differences to Parker’s ratio both on the AP view (P = .556) and lateral view (P = .698).
In the comparison of the Non-failure group, the Failure group significantly had bigger TAD (22.44 mm vs 18.86 mm, P=.046) and bigger CalTAD (27.99 mm vs 23.60 mm, P = .037) by means of univariate analysis.
Multivariate analysis of fixation position evaluations.

OR, adjusted odds ratio; CI, confidence interval; TAD, tip–apex distance; CalTAD, calcar-referenced tip–apex distance.

Receiver-Operating Characteristic (ROC) curve indicated that the best cut-off value of CalTAD was 23.76 mm. (the area under curve (AUC) = 0.775. Sensitivity = 77.8, specificity = 72.3, P = 0.001).
Reliability for significant variables.
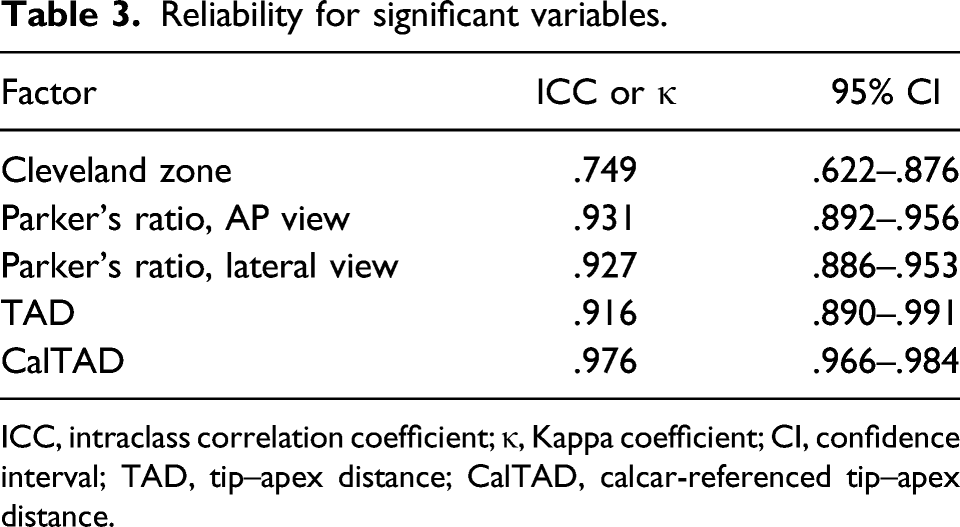
ICC, intraclass correlation coefficient; κ, Kappa coefficient; CI, confidence interval; TAD, tip–apex distance; CalTAD, calcar-referenced tip–apex distance.
Discussion
Disregarding reduction quality to discuss the relationship between the implant failures and the cephalic fixation position in ITF internal fixation is unreasonable, irresponsible, and meaningless. Reduction and how to evaluate it are the most important in ITF internal fixation. No doubt that anatomical reduction is the best for ITF. However, an anatomical reduction is exactly difficult in all geriatric ITF patients because of their aging. As we know, the acceptable reduction (anatomical reduction and positive medial cortex support reduction) can result in better mechanical effects and clinical outcomes.7,11 Therefore, the acceptable reduction is reasonable for geriatric ITF patients. After achieving acceptable reduction, the most important are fixation selection and fixation position. Nowadays, single-screw CMN is the most used fixator to treat ITF. Therefore, fixation position is the key factor for ITF treatment. And how to evaluate the fixation position of the cephalic fixation is the most important in ITF internal fixation during surgeries. We found that CalTAD was the key evaluation tool of cephalic fixation position for predicting implant failures in the geriatric ITF patients treated by single-screw CMN after obtaining an acceptable reduction in this retrospective study. And the optimal CalTAD was less than 23.76 mm for avoiding implant failures.
CalTAD is More Reasonable to Predict Implant Failures
As we have known, the emphasis of the Cleveland zone system, Parker’s ratio index, TAD, and CalTAD are different. Both the Cleveland zone system and Parker’s ratio index mostly emphasize on illustration of the cephalic fixation location. TAD emphasizes on the measurement of the cephalic fixation depth. While CalTAD, a modified TAD, is highly combined with the evaluation of cephalic fixation location and measurement of the cephalic fixation depth. Therefore, CalTAD is more reasonable to predict implant failures in ITF patients with internal fixation.
TAD, a reliable predictor for screw cut-out first reported by Baumgaertner, was widely used for illustrating the placement of cephalic nails at the time of operation. 9 Baumgaertner suggested that TAD should be lower than 25 mm for preventing cut-out in both extramedullary and intramedullary fixations. 9 In terms of CMN, John reported that TAD with 23.56 mm was the most sensitive for predicting cut-out. 19 Our study confirms a bigger TAD as the risk factor for implant failures (OR=1.149; 95%CI, 1.00-1.32; P = .046) by univariate analysis, but not as an independent predictor by multivariate analysis.
However, CalTAD, as a modified TAD, is highly combined with the evaluation of cephalic fixation location and measurement of the cephalic fixation depth. CalTAD was different from TAD because CalTAD favored an inferior–central region of the femoral head as the optimal cephalic nail position. CalTAD differed from TAD only in AP view while the same as TAD in lateral view. We calculated CalTAD based on the line which passed through the apex of the femoral calcar and paralleled to the longitudinal axis of the femoral neck in AP view. CalTAD, therefore, favored inferior–central placement of the cephalic fixation. 10 The significance of CalTAD in both the univariate analysis (P = .037) and the multivariate analysis (P=.018), combined with the almost perfect intraclass correlation coefficient shown in this study, supported that CalTAD was the only significant predictor of implant failures for geriatric ITF with CMN internal fixation.
Kashigar also reported that implant failures such as cut-out could not be there when CalTAD <20.98 mm. 10 Coinciding with Kashigar’s conclusion, 10 our study further confirmed that the best cut-off value in the ROC curve was 23.76 mm (P < .001). There is consensus in the literature that individual differences and geometrical characteristics correlated to the precise cut-off value.20,21 Moreover, the same as Kashigar and Kane,10,22 we postulate that a smaller CalTAD is likely to reduce the risk of implant failures.
Limitations or Weakness
There were still several limitations in this study. First, it was a retrospective study that cannot eliminate bias. Second, we only enrolled patients who underwent single-screw CMN implants; as a result, the conclusion might not apply to other kinds of internal fixation. Third, the sample size of this study was small, so further prospective investigations were needed to confirm these findings.
Conclusion
CalTAD is the key evaluation tool of cephalic fixation position for prediction of implant failures in geriatric ITF patients treated with single-screw CMN after obtaining an acceptable reduction.
Footnotes
Acknowledgments
We gratefully acknowledge Guangdong planned project of science and technology (No. 2015-110-8) for its partial support, and L Li for his C-arm X-ray assistance during surgery.
Author Contributions
All authors contributed to the study conception and design. The study was designed by Yun-fa Yang. Material preparation, data collection and analysis were performed by Jian-wen Huang and Xiao-sheng Gao. The first draft of the manuscript was written by Jian-wen Huang and was revised by Yun-fa Yang. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Partial support by Guangdong planned project of science and technology (No. 2015-110-8).
Ethics Approval
The study was approved by the Ethics Committee of Guangzhou First People’s Hospital (K-2020-106-01).
Code Availability
Software applications used in this study are listed as follows: IBM SPSS Statistic for Windows, Version 25.0. Armonk, NY: IBM Corp; Digimizer 5.4.4© 2005-2021 MedCalc Software Ltd; MedCalc® Statistical Software version 19.5.6 (MedCalc Software Ltd, Ostend, Belgium; https://www.medcalc.org; 2020).
Data Availability
The dataset supporting the conclusions of this study is available upon request by contacting the corresponding author, but the primary data were not shared because other studies related these primary data were underway confidentially.