
Abstract
Study Design
A meta-analysis
Introduction
To perform a meta-analysis to explore the risk factors of perioperative hidden blood loss (HBL) in the treatment of intertrochanteric fracture for Chinese patients.
Significance
An extensive search of the literature was performed in the English databases of PubMed, Embase, and Cochrane Library and the Chinese databases of CNKI and WAN FANG (up to July 2021). We collected factors including demographic data and surgical factors. Data analysis was conducted with RevMan 5.3 and STATA 12.0.
Results
Finally, we collected 7 studies including 1377 patients in the final analysis. In our study, female patients (P <.00001), hypertension (P =.008), time from injury to operation (<2 days, P =.02), operation time (≥60 mins, P =.001), fracture type (A2.2 to A3.3, P <.00001), and without anticoagulation (P <.00001) were found to be associated with perioperative HBL in Chinese patients receiving the treatment of the intertrochanteric fracture. However, anesthesia, ASA classification, and body mass index were not associated with perioperative HBL.
Conclusions
In our study, female patients, hypertension, time from injury to operation (<2 days), operation time (≥60 mins), fracture type (A2.2 to A3.3), and without anticoagulation were related to increased risks of perioperative HBL in Chinese patients receiving the treatment for the intertrochanteric fracture. We hope this article can guide for surgeons to reduce perioperative HBL as far as possible in the treatment of intertrochanteric fracture.
Introduction
With the rapidly increasing number of the aging population, hip fractures, of which 40%–45% occur in the trochanteric region including femoral neck fracture and intertrochanteric fracture, increase each year. 1 It is estimated that about 1.7 million people suffer from hip fractures each year in the world. 2 The morbidity and mortality of hip fractures are also displaying a rising trend, which brings a huge burden to individuals, families, or even society. Anemia, as an important complication of hip fractures, has been given more and more attention. 3 Actually, total blood loss during treating hip fractures is much larger than that observed during surgery. 4 Up to now, increasing articles have been focused on the risks of hidden blood loss (HBL), which were easily ignored. With the advent of the concept of the HBL, several researchers discovered that there was a large amount of potential blood loss following hip fractures, which was frequently disregarded. Previous research has revealed that the average drop in Hb level between admission and discharge was 16 g/L, with an excess of up to 6-fold that recorded during the surgical operation.5-8 However, there remains a considerable controversy. As we know, few articles explored the risk factors of HBL after surgery in the treatment of intertrochanteric fracture by performing a meta-analysis, which is the aim of this study.
Methods
Search Strategy
We searched for English and Chinese language studies with the keywords ‘‘hidden blood loss,’’ ‘‘intertrochanteric fracture,’’ and “risk factors” in the English databases of PubMed, Embase, and Cochrane Library and the Chinese databases of CNKI and WAN FANG. There was no limitation on the date of publication, which covered all previously published studies up to July 2021.
Eligibility Criteria
Included articles must meet the following criteria: (1) the study population must be adult Chinese patients; (2) the incidence and risk factors of perioperative HBL must be measured; (3) patients must only have an intertrochanteric fracture, and (4) hemoglobin (Hb) and hematocrit (Hct) must be measured on the day of admission and postoperative 2–3 days. Studies were excluded if they (1) were abstracts, letters, reviews, or case reports; (2) had repeated data; (3) did not report outcomes of interest; (4) patients treated for tumors, infection, or inflammation; or (5) patients who had had hip surgery in the past.
Data Extraction and Outcome Measures
The data include the general characteristics of each study and the outcomes measured. General characteristics include first author, year of publication, country, the number of patients, and type of article. The outcome includes the rate of every risk factor. When the same population was reported in several publications, we retained only the most informative article or complete work to avoid duplication of information. The data were extracted independently by two authors. Any disagreements concerning paper eligibility were resolved by discussion and consensus. Test for the risk of publication bias. We performed a visual inspection of the funnel plot for publication bias. The funnel plot should be asymmetric when there is publication bias and symmetric in the case of no publication bias. We performed Egger and Begg tests to measure the funnel plot asymmetry using a significance level of P <.10. The trim and fill computation was used to estimate the effect of publication bias. Sensitive analysis overall Because of the low heterogeneity of every factor, we do not calculate sensitive analysis.
Statistical Analysis
Only continuous outcomes were mentioned in our study, so odd ratios (ORs) and 95% confidence intervals (CIs) were calculated for outcomes. A P value <.05 was judged as statistically significant. Random-effects or fixed-effects models were used depending on the heterogeneity of the studies included. Heterogeneity was analyzed with both the chi-squared test and I square test, where a P value of <.10 for the chi-squared and I2 >50% implied heterogeneity. 9 All statistical analyses were performed using Review Manager version 5.3 (The Cochrane Collaboration, Oxford, UK) and STATA 12.0 (Stata Corporation, College Station, TX, USA).
Results
Study Identification and Selection
Initially, we collected a total of 110 records through the database search. 71 records were excluded due to repetition and 25 records were removed for review based on the titles and abstracts. The remaining 14 records were retrieved for inclusion criteria and 7 of them were excluded. Finally, seven articles that met our inclusion criteria were included in the present meta-analysis. The selection process that was included in this meta-analysis is shown in Figure 1. Flow diagram of study selection
Baseline Characteristics and Quality Assessment
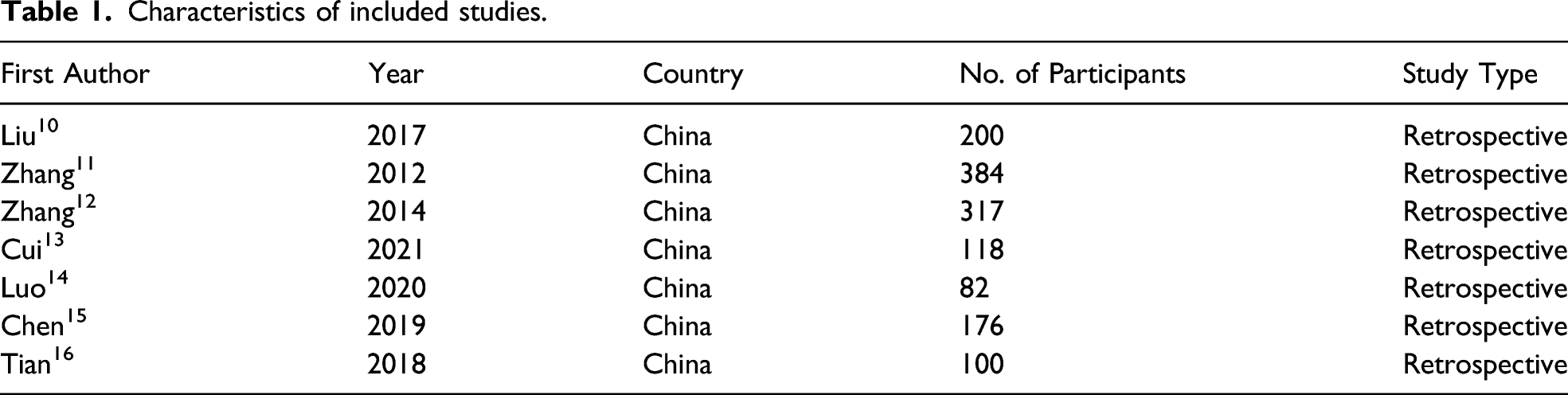
Characteristics of included studies.
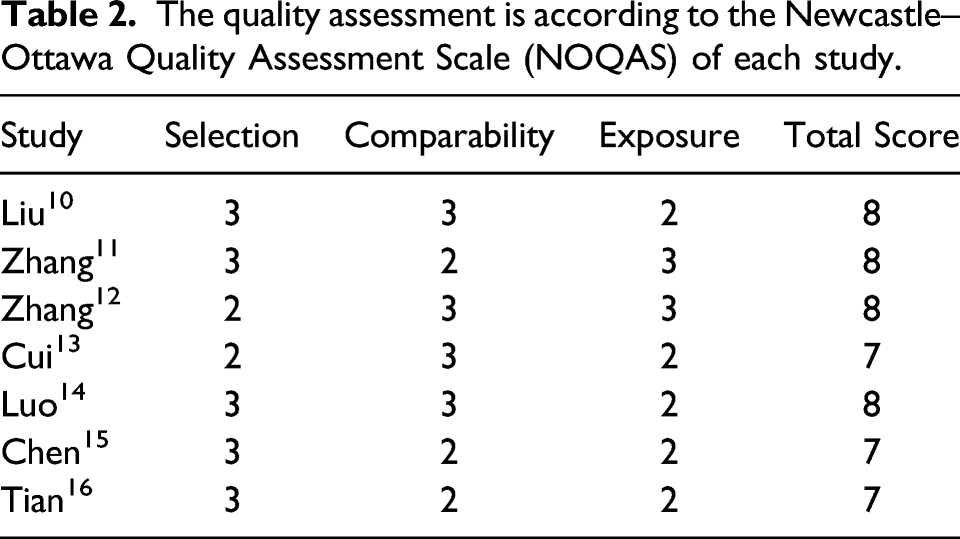
The quality assessment is according to the Newcastle–Ottawa Quality Assessment Scale (NOQAS) of each study.
Assessment of Risk Factors of HBL
Gender
Four studies10-13 reported the relationship between gender and HBL. The test for heterogeneity was not significant and the studies had low heterogeneity (P for heterogeneity = .36; I2 = 6%, Figure 2). The meta-analysis showed that female patients were significantly associated with HBL (fixed-effects model; P <.00001, OR= −17.00, 95% CI [−18.26, −15.74], Figure 2). The standardized mean difference (SMD) estimates relationship between sex and hidden blood loss. CI=confidence interval, df=degrees of freedom, M-H=Mantel–Haenszel.
Hypertension
Three studies12-14 reported the relationship between hypertension and HBL. The test for heterogeneity was significant and the studies had low heterogeneity (P for heterogeneity = .46; I2 = 0%, Figure 3). The meta-analysis showed that hypertension was associated with significantly associated with HBL (fixed-effects model; P=.008, OR=47.65, 95% CI [12.53, 82.77], Figure 3). The standardized mean difference (SMD) estimates the relationship between hypertension and hidden blood loss. CI=confidence interval, df=degrees of freedom, M-H=Mantel–Haenszel.
Diabetes
Three studies12-14 reported the relationship between diabetes and HBL. The test for heterogeneity was significant and the studies had low heterogeneity (P for heterogeneity =.33; I2 =9%, Figure 4). The meta-analysis showed that diabetes was not associated with HBL (fixed-effects model; P =.05, OR =45.49, 95% CI [−.66, 91.63], Figure 4). The standardized mean difference (SMD) estimates the relationship between diabetes and hidden blood loss. CI=confidence interval, df=degrees of freedom, M-H=Mantel–Haenszel.
Time From Injury to Operation
Two studies10,12 reported the relationship between time from injury to operation (<2 days vs ≥2 days) and HBL. The test for heterogeneity was significant and the studies had low heterogeneity (P for heterogeneity =.97; I2 =0%, Figure 5). The meta-analysis showed that time from injury to operation<2 days was significantly associated with HBL (fixed-effects model; P =.02, OR =49.96, 95% CI [6.80, 93.13], Figure 5). The standardized mean difference (SMD) estimates the relationship between time from injury to operation and hidden blood loss. CI=confidence interval, df=degrees of freedom, M-H=Mantel–Haenszel.
Operation time
Two studies12,14 reported the relationship between operation time (<60 mins vs ≥60 mins) and HBL. The test for heterogeneity was not significant and the studies had relatively high heterogeneity (P for heterogeneity =.14; I2 =54%, Figure 6). The meta-analysis showed that operation time ≥60 mins was significantly associated with HBL (fixed-effects model; P =.001, OR =−65.91, 95% CI [−96.43, −25.84], Figure 6). The standardized mean difference (SMD) estimates the relationship between operation time and hidden blood loss. CI=confidence interval, df=degrees of freedom, M-H=Mantel–Haenszel.
Fracture type
Three studies12-14 reported the relationship between fracture type (A1.1 to A2.1 vs A2.2 to A3.3) and HBL. The test for heterogeneity was significant and the studies had low heterogeneity (P for heterogeneity =.19; I2 =39%, Figure 7). The meta-analysis showed that fracture type (A2.2 to A3.3) was significantly associated with HBL (fixed-effects model; P <.00001, OR=−145.17, 95% CI [−176.63, −113.71], Figure 7). The standardized mean difference (SMD) estimates the relationship between fracture type and hidden blood loss. CI=confidence interval, df=degrees of freedom, M-H=Mantel–Haenszel.
Anesthesia
Two studies12,14 reported the relationship between anesthesia (general vs spinal or nerve block) and HBL. The test for heterogeneity was significant and the studies had low heterogeneity (P for heterogeneity =.88; I2=0%, Figure 8). The meta-analysis showed that anesthesia was not significantly associated with HBL (fixed-effects model; P =.08, OR =37.45, 95% CI [−4.20, 79.10], Figure 8). The standardized mean difference (SMD) estimates the relationship between anesthesia and hidden blood loss. CI=confidence interval, df=degrees of freedom, M-H=Mantel–Haenszel.
ASA classification
Three studies10,12,14 reported the relationship between ASA classification (I, II vs III or IV) and HBL. The test for heterogeneity was significant and the studies had low heterogeneity (P for heterogeneity =.92; I2 =0%, Figure 9). The meta-analysis showed that ASA classification was not associated with significantly associated with HBL (fixed-effects model; P =.55, OR =−15.95, 95% CI [−68.64, 36.74], Figure 9). The standardized mean difference (SMD) estimates the relationship between ASA classification and hidden blood loss. CI=confidence interval, df=degrees of freedom, M-H=Mantel–Haenszel.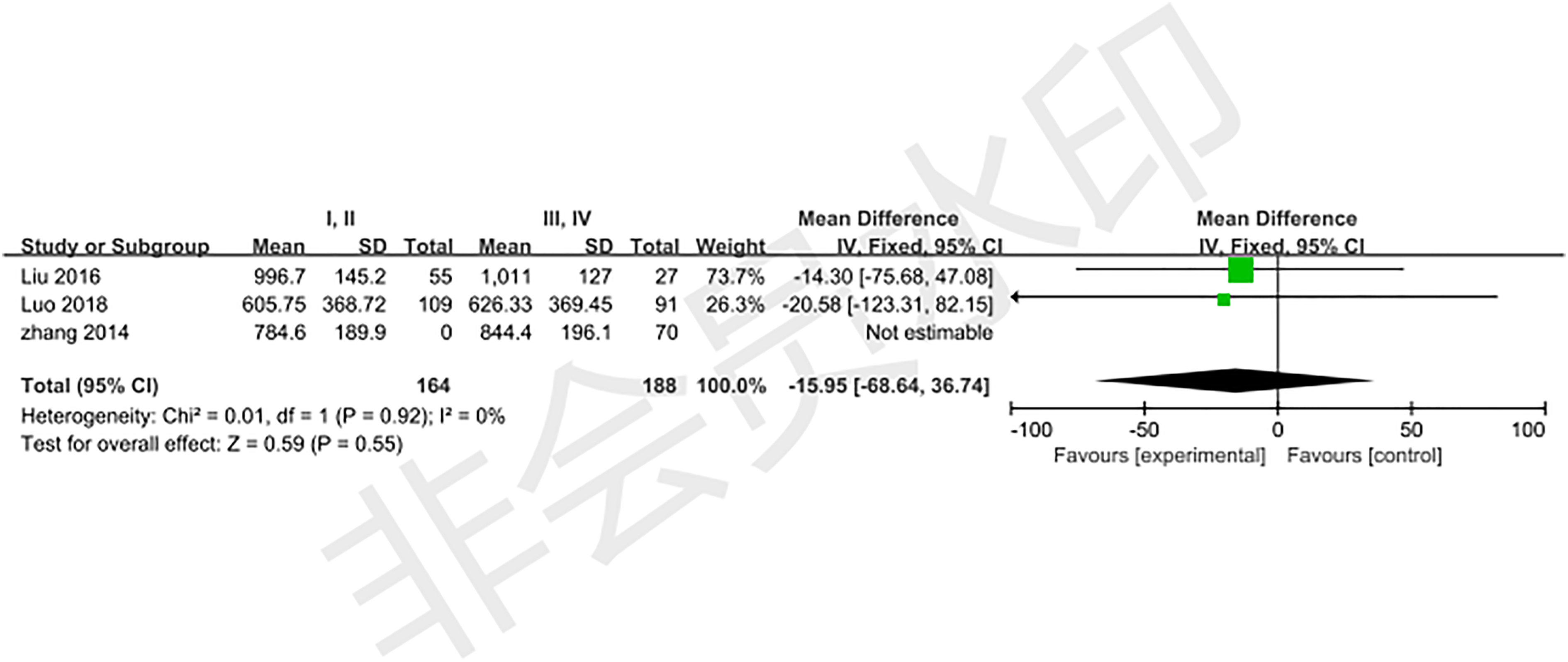
Anticoagulation
Three studies14-16 reported the relationship between anticoagulation and HBL. The test for heterogeneity was significant and the studies had low heterogeneity (P for heterogeneity =.26; I2 =25%, Figure 10). The meta-analysis showed that without using anticoagulation was significantly associated with HBL (fixed-effects model; P <.00001, OR =−81.30, 95% CI [−101.11, −61.50], Figure 10). The standardized mean difference (SMD) estimates the relationship between anticoagulation and hidden blood loss. CI=confidence interval, df=degrees of freedom, M-H=Mantel–Haenszel.
Body mass index (BMI)
Two studies10,13 reported the relationship between BMI and HBL. The test for heterogeneity was significant and the studies had low heterogeneity (P for heterogeneity =.66; I2 =0%, Figure 11). The meta-analysis showed that BMI was not significantly associated with HBL (fixed-effects model; P =.21, OR =36.86, 95% CI [−20.24, 93.95], Figure 11). The standardized mean difference (SMD) estimates the relationship between body mass index and hidden blood loss. CI=confidence interval, df=degrees of freedom, M-H=Mantel–Haenszel.
Publication bias
After a detection of publication bias by STATA 12.0, there was no publication bias found for all included studies (all P >.05).
Discussion
Intertrochanteric fractures are common injuries in clinics, especially for the older population. Nowadays, surgery is a recommendable choice to treat intertrochanteric fractures which is able to achieve good operative results.17,18 However, mortality, as a serious complication, definitely affects the total outcomes of treatment for intertrochanteric fractures. Previous research found that more than 10% of European patients with hip fractures died within 30 days, and more than 25% died within 1-year.16,19 Anemia is one of the important factors related to mortality rate, which increases the incidence of pulmonary and cerebral diseases and breaks the balance of oxygen supply and demand in the tissues.
Currently, perioperative HBL while treating hip fracture has been controversial and is still a topic of debate. Foss 5 observed 546 hip fracture patients and found that the total blood loss was 6 times the blood loss in surgery. In addition, Foss hypothesized that HBL may be associated with postoperative hemorrhaging, anticoagulation, and bleeding from other sources. Li 20 retrospectively evaluated the perioperative blood loss in older patients with intertrochanteric fractures and found that the cumulative total blood loss from admission to postoperative day was 863.8 ± 429.9 mL, of which the mean HBL was 772.3 ± 424.7 (89.4%), and the mean preoperative HBL was 375.5 ± 242.0 mL. Wang 21 found that age, diabetes, operation time, and time from trauma to operation may be the risks of HBL, whereas Liu 10 indicated that an at-admission albumin level < 30 g/L was associated with HBL.
Although an increasing number of articles have been focused on HBL, the risk factors for it remain debated. The aim of our study was to explore the risks of perioperative HBL in the treatment of intertrochanteric fractures in Chinese patients. To eliminate racial differences and minimize heterogeneity, only Chinese patients were included. As far as we know, this was the first meta-analysis to report the risks of perioperative HBL for Chinese patients. Our findings showed that anesthesia, ASA classification, patients with a history of diabetes, and body mass index were not associated with HBL. However, female patients, patients with a history of hypertension, time from injury to operation (<2 days), operation time (≥60 mins), fracture type (A2.2 to A3.3), and without anticoagulation were associated with an increased risk of perioperative HBL in the treatment of intertrochanteric fracture.
Luo 14 found that HBL was significantly higher in male patients than in female patients with intertrochanteric fracture. While Miao 22 found that female patients had a higher risk of increased HBL than male patients receiving total hip arthroplasty. In the current study, our results were consistent with those of Miao. Our results also revealed that hypertension was considered an important risk for HBL. Two possible explanations were accounting for this. First, it was well known that patients with hypertension were more likely to bleed than those with normal blood pressure, which could lead to more HBL. Second, changes in hemodynamics and blood composition caused by hypertension may lead to more HBL. Similar results can also be found in our study that patients with a history of diabetes, as a risk factor for HBL, may be associated with body matter and blood metabolism.
Harper 23 reported that there were 44% of delays from 25 to 48 hours, and 42% of delays were greater than 48 hours from hospitalization to surgery due to hematologic abnormalities. As for the timing of surgery, it has been debated by reviewing related articles. Luo 14 found a positive relation between preoperative blood loss and the timing of surgery, but a negative correlation between perioperative HBL and timing of surgery. However, our previous study 24 demonstrated that patients with intertrochanteric fractures operated within 2 days may cause more perioperative HBL in comparison with those operated for more than 2 days, which was consistent with this study. It was well known that the body after injury was in a state of blood loss, and the hematopoietic mechanism was also stimulated since then. Moreover, Wilson 25 found a hypercoagulable state in patients that occurred from 3 to 5 days after operation. The operation, similar to the initial fracture, is also essentially equivalent to trauma for patients. Thus, we could infer that patients who were operated without a hypercoagulable state (within 2 days) were more likely to have blood loss in comparison with those who were operated in a hypercoagulable state (more than 2 days). Regarding operation time, our result was consistent with previous results that more operation time may cause more blood loss.
Kumar 26 and Luo 14 observed a significant correlation between the amount of HBL and the fracture types. Furthermore, Cui 13 found that patients with AO/OTA types 31-A2.2 to 31-A3.3 fractures had more HBL than those with AO/OTA types 31-A2.2 to 31-A3.3 fractures, which was the same as our results. It was obvious that unstable fractures were more serious than stable fractures, which could definitely cause more HB. Therefore, we should pay more attention to reviewing patients’ routine blood tests and obtaining timely blood transfusions during treatment for complicated fracture types.
Several randomized controlled trials16,27 published in recent years have confirmed that patients without using anticoagulation experienced less blood loss in the treatment of the intertrochanteric fracture. Undoubtedly, our results were the same as in previous studies. However, few literature reported on the risk of venous thrombosis in patients with intertrochanteric fracture using anticoagulants, to which we should pay attention.
Regarding anesthesia and ASA classification, our results were the same as previous findings.10,11,15 However, slight differences were present for body mass index (BMI). Liu 10 proved that BMI<25 kg/m2 was a risk factor in the univariate analyses, but not in the multivariate analyses, whereas Cui 13 demonstrated that BMI was not a predictive factor, no matter in the univariate analyses or multivariate analyses. Our results showed no relationship between BMI (<28 kg/m2 vs BMI ≥28 kg/m2) and perioperative HBL. The reason leading to the difference might be associated with the different standards for the definition of BMI.
There were several limitations in this study. First, there was no RCT article focused on HBL; we need RCT articles for performing the further study. Second, the statistical power could be improved in the future by including more studies. Due to the small number of included studies, some parameters like age, transfusion, surgery type, and fixation could not be analyzed. Finally, we found that all the included articles originate from China, but each one presents high-quality data.
In conclusion, female patients, patients with a history of hypertension, time from injury to operation (<2 days), operation time (≥60 mins), fracture type (A2.2 to A3.3), and without anticoagulation were found to be risk factors for perioperative HBL in the treatment of intertrochanteric fractures in Chinese patients. In this meta-analysis, we can clearly see which characteristics of patients were more likely to have more perioperative HBL. We hope this article can provide a reference for surgeons in the treatment of intertrochanteric fractures. Meanwhile, it is helpful for future studies on HBL. Further large-scale, well-designed studies are urgently needed.
Footnotes
Authors’ contributions
TW and JFG were responsible for studying the concept and writing the article. ZYH was responsible for revising the article. ZYH was responsible for reviewing and writing the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was financially supported by the National Key R&D Program of China (No. 2019YFC0120600), and the 2019 Hebei Provincial Department of Finance Geriatric Disease Prevention and Control Funds.
Ethics approval and consent to participate
This study was approved by the institutional review board (IRB) of the Third Hospital of Hebei Medical University (No. T2018-026-1). An informed consent from the patients was not considered necessary by the Ethics Committee as it is a meta-analysis study. The present study has been conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Availability of Data and Materials
All data generated or analyzed during this study are included in this article. Further inquiries can be directed to the corresponding author.