
Abstract
Purpose/Background:
Olecranon fractures are common, particularly in the elderly osteoporotic population. Although various techniques of fixation are available, the gold standard—tension band wiring (TBW)—has high complication and reoperation rates. We sought to identify current evidence for the use of high-strength suture tension banding methods to determine whether they reduce complications and reoperation rates while maintaining fixation.
Methods:
A systematic review of several databases was performed according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The databases included Cochrane, PubMed, MEDLINE and Embase. We searched for evidence of at least Level I to IV (according to NHMRC) of the use of tension band suturing or anchors in the surgical treatment of displaced olecranon fractures. We also analyzed the cost of fixation in our institute.
Results:
Four hundred and forty articles were identified. Of these, 9 met the inclusion criteria. One hundred thirty-one subjects had an average age of 66 years. All the studies showed that high-strength suture tension banding/anchoring maintained fixation with displaced olecranon fractures, reducing the complication rates and showed minimal reoperation rates. There was also a significant cost advantage of the suture tape construct mainly due to avoiding subsequent removal of metal.
Conclusion:
Tension band suturing or anchoring displaced olecranon fractures may be an alternative cost effective method to TBW in maintaining fixation, reducing metalware complications and reducing re-operation rates.
Level of Evidence:
IV.
Introduction
Fractures of the olecranon account for approximately 20% of all proximal forearm fractures, with the most common mechanism of injury being a simple fall from standing height and the most common type being Mayo 2A. 1
Various fixation methods are available to treat olecranon fractures, such as tension band wiring (TBW), intramedullary screw fixation (IS) and the recently used tension band suturing. These fixation methods have resulted in the anatomical reduction, restoration of movement and healing of the fracture. However, problems exist with the different types of fixation, such as the loss of fixation, non-union and revision surgery.
TBW is the gold standard of fixation for simple displaced olecranon fractures, converting the distraction forces of the triceps to compression at the articular surface. Several complications are usually encountered with this method, such as wound breakdown, metalwork prominence leading to discomfort, the loss of motion and the need for revision surgery to remove the hardware. Reoperation rates are high with TBW, up to 46% with 65% of patients with prominent hardware causing irritation and pain. 2
Investigating alternative methods of fixation to reduce complications is paramount. Although various implants exist in the market, no ideal solutions are currently available for the fixation of these fractures. Tension band suturing with or without anchors is a new method used with great success in recent case series and biomechanical studies without complications of metal removal. 3 -5
In this study, we aimed to systematically review the literature of high-quality studies to justify the use of tension band suturing with or without anchors for elderly patients with displaced olecranon fractures.
Methods
This systematic review aimed to investigate the following population, intervention, control and outcome (PICO) question: in elderly patients with displaced simple olecranon fractures, does the use of tension band suture fixation provide a stable construct compared with TBW to reduce reoperations and complications?
To address this question, we performed a systematic review of the available medical literature using several medically relevant databases, including Cochrane, PubMed, MEDLINE and Embase.
Two authors independently performed the search on September 7, 2020. The database journal search dates ranged from 1948 to the current year. A range of search items was used to obtain all the articles related to the topic (Table 1). The search terms included various combinations, including tension band suture, tape, anchors and olecranon as keywords. Level I to IV evidence (according to the NHMRC) was used in the review. Potential inclusive papers were manually screened by the authors and discussed, and a decision was made regarding inclusion or exclusion. The full manuscripts of the remaining articles were reviewed, and reference lists were checked for potential studies not identified by our original search. The authors of these articles were further contacted without any further discovery of additional publications related to this review. The inclusion and exclusion criteria were established to ascertain the highest quality studies to answer our clinical question.
Inclusion
Level I to IV evidence studies, including comparative studies
English language studies only
Human or cadaveric subjects
Study publication date from January 1, 1948 to the current year
Studies investigating tension band suture or anchor fixation with traditional TBW or metal wiring techniques
Exclusion
Level V evidence studies, including case reports and technical notes
Non-English language studies
Studies investigating fixation techniques other than suture fixation
No plate fixation augmentation
Trials not published at the time of search
Subjects aged younger than 18 years
Search Results of Keywords in the Databases

Table 1 identifies all the databases and search criteria citation results. 440 were identified across the 4 databases. The title, abstract and keywords of all the articles were then screened for relevance. After applying the exclusion criteria and removing duplicate studies, 9 studies met the inclusion criteria, which were further analyzed.
Three articles were excluded upon full-text evaluation. The Kuru and Mutlu study 6 was excluded because they used a 3-dimensional finite element bone model to simulate real human bone and compare different fixation techniques. This model was excluded in this review because it did not simulate real anatomical tissue subjected to mathematical computer-based equations to provide results of the difference techniques. The other 2 articles were excluded because they were either very small case reports and or were technical notes classified as level V evidence. 7,8
Two authors then reviewed 9 articles independently, and the data were extracted. An attempt was made to identify common outcome measure (s) across all the studies analyzed. However, several different clinical outcome measures were used for assessment, such as the force to failure, cycles to failure, clinical scores, displacements and range of movement. A P-value less than 0.05 were deemed a priori to be statistically significant. The lack of subject-level specific data and heterogeneity in outcome reporting precluded meta-analysis.
Results
The extensive literature review is summarized in the PRISMA flow diagram (Figure 1).

The PRISMA flow diagram illustrating the selection procedure for article inclusion. A total of 440 studies were identified through free text searching of the Cochrane library, Pubmed, Medline and Embase databases.
The authors independently searched keywords in the databases to identify 440 articles. The screened titles, abstracts and keywords highlighted 12 relevant articles for full manuscript review. The reference lists and author contacts of those relevant articles revealed no further studies. Independent analysis of the full text of all the articles identified results in 9 relevant studies included in the final review. Four biomechanical cadaveric comparative studies and 5 human retrospective case series were identified for review.
All the articles identified were level III or IV based on NHMRC levels of evidence. At the time of review, no level 1 systematic reviews or randomized control trials were available. For discussion, all the subjects in the studies were either prospective cohort human studies or cadaveric olecranon fracture specimens. The total cohort size was 131 subjects (52 cadaveric and 79 live human patients) with an average age of 66 years. Two studies disclosed potential conflicts of interest in their research (Cha et al and Von Keudall et al). The other 7 studies reported no other conflicts of interest. The risk of bias of the articles is summarized in Table 2.
Risk of Bias of Studies.

All the studies showed that tension band suture, with or without suture anchors, maintained fixation and reduced complications, particularly reoperation. Four studies used FiberWire fixation methods 9,11,14,15 with results comparable to TBW regarding union without hardware complications. Three studies also used suture anchors, 5,12,15 also providing excellent fixation with biomechanical, radiological and clinical markers. The use of high-strength braided sutures, including No. 5 Ethibond, No. 2 Ultrabraid, No. 2 Orthocord and No. 2 Panacryl transosseously could also maintain fixation and reduce reoperation rates but showed some failure at high forces when early mobilization was simulated. 3,5,10,11,13
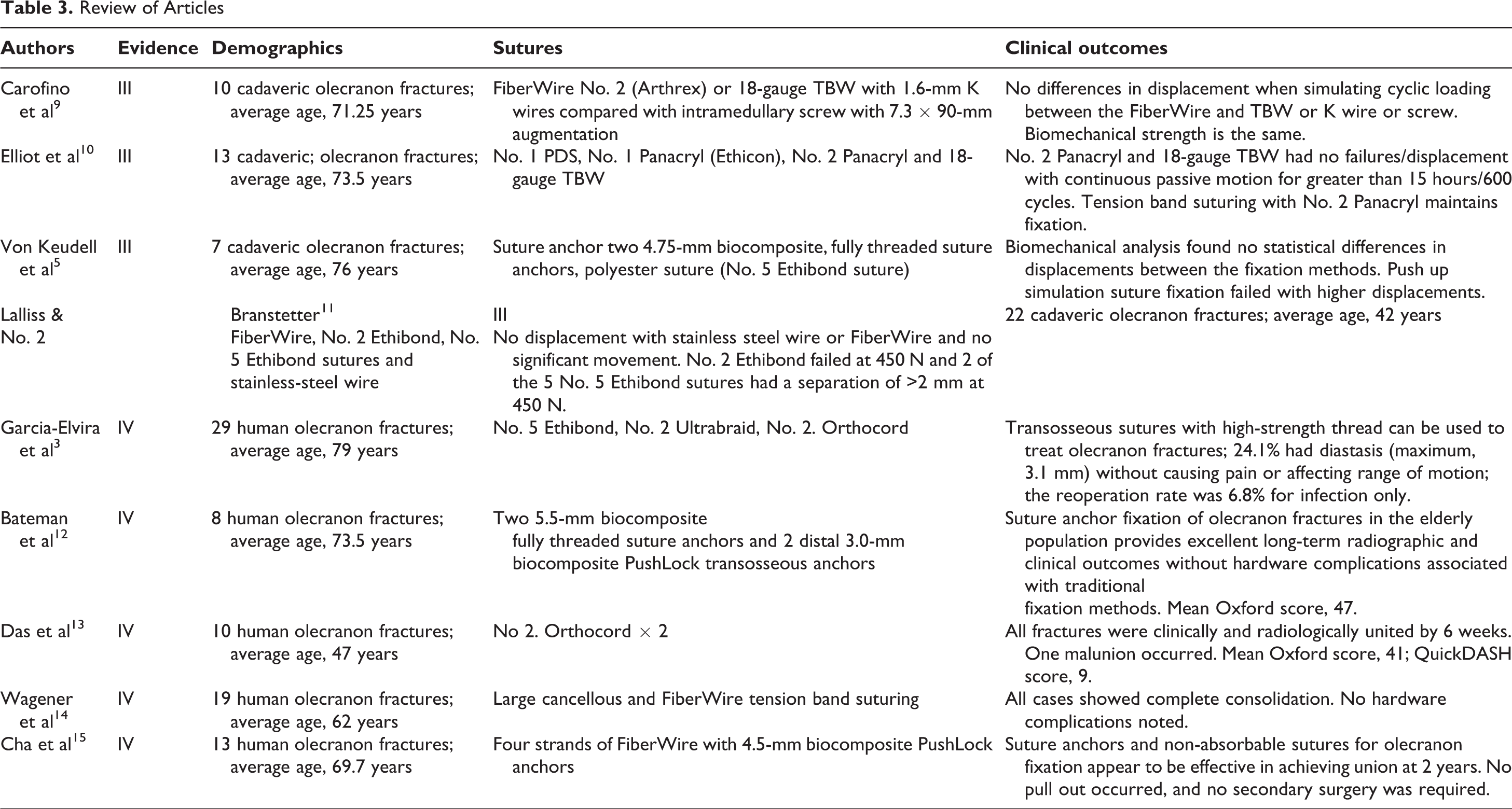
The details of these articles are summarized in Table 3.
Review of Articles
Discussion
Displaced olecranon fractures affect the functional outcomes in patients. Traditional surgical management for olecranon fractures includes TBW with K wires, intramedullary screw or plate fixations, with each technique yielding similar outcomes. 16
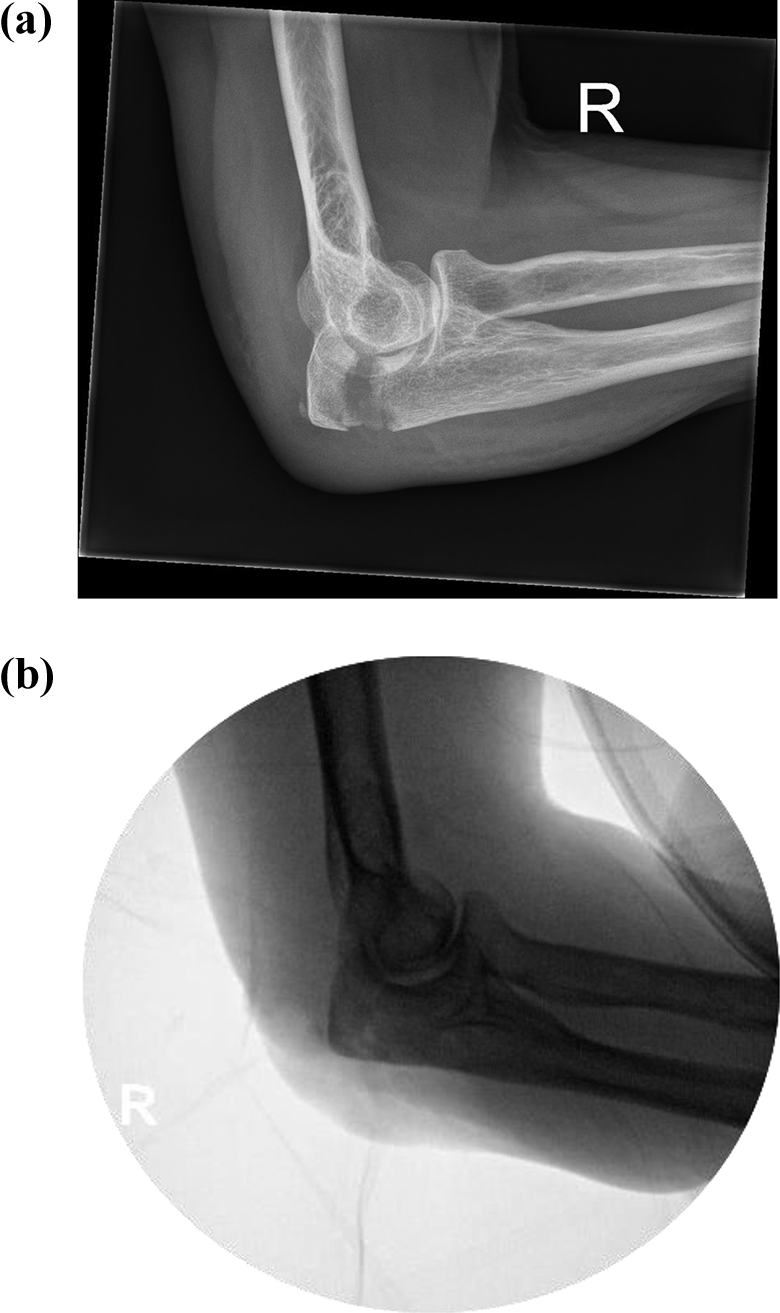
Classically, K wires and metal TBW are used for simple displaced olecranon fractures and olecranon osteotomies according to the AO trauma classification (Figure 2). Due to the high complication rates (12-14), such as pull out (up to 80%), defects of the skin and infection requiring reoperation, alternative techniques are available but have not been studied extensively. 17,18

a) Pre-operative x-ray of displaced olecranon fracture. b) Post-operative x-ray of a) treated with K-wires and TBW.
In a more recent study that investigated reducing the problems with TBW, particularly in the pediatric population, Nimura et al 8 introduced FiberWire to reduce olecranon fractures in children, eliminating metalware removal and complaints of pain and skin irritation in their small case report study. Gortzak et al 19 further expanded their technique using percutaneous K wires with absorbable suture tensioning in 6 pediatric patients with a mean follow up of 13 months and showed no immediate complications with good radiographic results.
FiberWire is a high strength polyblend suture comprising polyester and polyethylene; it has more than twice the strength of traditional sutures like PDS, Orthocord, Ultrabraid and a braided polyester suture like Ethibond. The ultimate strength of FiberWire was found to be up to 2.5-fold greater than that of traditional nonabsorbable sutures, such as those made of polyester or polydioxanone. 20 Several biomechanical studies have shown that FiberWire sutures are as good as stainless steel in fixation maintenance of the patella 21 and elbow fractures. 9
Carodino et al 9 used high-strength tension band suturing for olecranon fracture repair and compared the technique to standard TBW using a steel wire. They used 2 strands of No. 2 FiberWire. When testing under both active motion and simulated chair push up conditions, they found no significant difference in fixation between the FiberWire and metal gauge wire tension bands using either K wires or intramedullary screws.
Von Keudall et al 5 investigated simulated olecranon fractures in osteoporotic bone. They compared 3 fixation techniques, K wire fixation, suture anchor fixation and a polyester suture with a No. 5 Ethibond suture. They found no significant difference in displacements when comparing all the methods of fixation with an active range of motion. However, with simulated push up testing, the polyester suture failed after 17 cycles and showed significantly higher displacement but no difference between suture anchor fixation and K wire fixation. They concluded that suture anchors might be a viable solution to osteoporotic olecranon fractures in geriatric patients.
When comparing 3 common suture fixations (No. 2 and No. 5 Ethibond and No. 2 FiberWire) to steel wire tension banding for olecranon fractures, Lalliss and Branstetter 11 showed that, with high forces (450 N), Ethibond suture fixation failed with separation. However, FiberWire showed no significant failures measured across the site of the osteotomy comparable to stainless steel wire, particularly when simulating pushing up from a chair for 500 cycles. These high forces may be excessive when imposed on a healing fracture when unprotected with immobilization. Given these results, FiberWire could be used as an alternative to steel wire in tension band fixations of transverse fractures and osteotomies of the olecranon.
This systematic review looked at the available evidence of the use of sutures or anchors in the fixation of displaced olecranon fractures in elderly patients. Most of the materials used could maintain fixation initially, but all biomechanical studies simulated early mobilization protocols with high forces, causing failure with specific braided sutures like Ethibond. However, all the studies using FiberWire were positive with no failures of fixation, biomechanically comparable to the stainless-steel wire. The effectiveness of FiberWire may reduce the discomfort from hardware and reoperation rates seen with traditional TBW and K wires. Three studies also used suture anchors, 5,12,15 which also provided excellent fixation with biomechanical, radiological and clinical markers comparable to TBW. These alternatives to traditional metal fixation can prevent the irritation, skin complications and morbidity of reoperation, particularly with older adults.
This technique is used for fixation of simple transverse or avulsion olecranon fractures and chevron osteotomies. It can also be used to augment plate fixation of comminuted proximal ulna fractures. It has also been shown to be effective in pediatric olecranon fractures where placement of metalwork is even less desirable and early range of motion is needed. 22 The suture anchor technique described by Bateman et al 12 is also an alternative fixation especially in elderly patients with excellent long-term radiological and clinical outcomes without hardware complications of traditional metalwork fixation. There has been no comparative study on the different type of suture or anchor fixation techniques to assess superiority at present. These surgical techniques are summarized below in Figure 3. The authors of this review recommend a modified technique described by Phadnis and Watts in 2017 23 shown in Figure 4 (technique 5) with the use of SutureTape ® (Arthrex) which is a flat-braided suture with similar structure as FibreWire® (Arthrex) suture but more resistant to tissue pull out. When compared to wire suture, transosseous braided tape suture provides almost twice the bone pull-through strength 24 and provides the strength needed in displaced olecranon fractures.

Bar chart showing the mean displacement of an olecranon osteotomy during a) simulated active range of movement with 1000 cycles at 15N and b) during simulated pushing up from a chair with 500 cycles at 450N. The error bars represent the standard error of the mean. Reprint permission copyright from Lalliss & Branstetter. 11

Five methods of fixation for displaced olecranon fractures without the use of metal tension-band wiring. 1. Suture bridge fixation (Cha et al). (A) One transverse hole approximately 5 cm from the fracture site, and 2 oblique holes starting 2 cm proximal to the first hole and traversing to the fracture site, are drilled using a 2.5 mm drill bit. Four sutures are passed through the transverse hole and (B) through the bone to the fracture site using a suture passer. (C) 8 drill holes are made in the olecranon fragment using K-wire at a 90° degree angle, with the wires passed through these holes with a needle. (D) The wires are knotted and the olecranon fragment is reduced manually by an assistant, and confirmed using fluoroscopy. (E). Once reduced, the wire ends are attached to suture anchors 7-8 cm distal to the fracture site. 2. Bone tunnel fixation (Phadnis and Watts). (A) The fracture fragments are reduced, and a single transverse tunnel made through the ulna with a 2.5 mm drill bit at least 15 mm distal to the fracture line. Two sutures in total will be threaded through the hole. (B) The first suture is passed from lateral to medial, with a grasp of the lateral triceps tendon taken at its insertion point. The suture is then passed back through the tunnel with a section of medial tendon grasped, before the knot is tied on the medial side and protected under the anconeus muscle. (C) A second suture is passed and follows a similar course to the first, however the suture is moved dorsally and obliquely to capture the tendon on the opposite side to which it exits the tunnel. 3. Suture anchor fixation (Bateman et al). (A) Two suture anchors are inserted into the cancellous bone bed of the ulna, toward the dorsal aspect of the bone. (B) The 8 total suture anchor limbs are passed transosseously through the fracture fragment using a free needle. (C) The first limb of each anchor is passed through the triceps tendon using the Krackow method and knotted to the second limb. (D) The third and fourth limbs of each are attached to suture anchors on the ulnar as pictured, with accurate reduction confirmed with visual inspection and fluoroscopy. 4. Transosseous high strength fixation (Garcia-Elvira et al). (A) Two tunnels are drilled, one proximal (relatively more ventral) hole which communicates with the hollow cortex of the ulnar, and another distal (relatively more dorsal) tunnel. (B) Two threads are passed through the proximal hole, which exit through the cortex to the fracture site. One of each suture end is passed through 1 of 4 holes within the proximal olecranon fragment and then (C) knotted, and the fracture is reduced. (D) Two sutures are then passed through the distal tunnel and travel obliquely across the olecranon to form a figure-of-8, with a Krakow or Kessler type knot used to tie the suture to the triceps brachii tendon. 5. Bone tunnel fixation (authors preferred method with a flat-braided suture). (A) The fracture fragments are reduced and a single transverse tunnel made through the ulna with a 2.5 mm drill bit at least 15 mm distal to the fracture line. Two sutures in total will be threaded through the hole. (B&C) The first suture is passed from lateral to medial, with a grasp of the lateral triceps tendon taken at its insertion point. The suture is then passed back through the tunnel with a section of medial tendon grasped, before the knot is tied on the medial side and protected under the anconeus muscle. (D&E) A second suture is passed and follows a similar course to the first, however the suture is moved dorsally and obliquely to capture the tendon on the opposite side to which it exits the tunnel. For all suture techniques, we recommend passing the sutures close to the bone as possible to minimize loss of tension of the construct as the sutures could erode through soft tissue. We also recommend taking a small full thickness bite of the triceps tendon, rather than a large bite, which can result in deformation of the tendon when the sutures are tensioned. Figure produced with BioRender.
a) Pre-operative displaced olecranon fracture. b) Intra-operative imaging post tension band suturing technique.
This systematic review is the first to look at the use of sutures or anchors as tension bands in displaced olecranon fractures that can have a large impact on TBW morbidity, including irritation, skin breakdown, pain and pull out. Nonabsorbable braided sutures can replace stainless steel wire and K wires, as shown by the available evidence. All the studies showed positive results with respect to fracture reduction, patient functional outcomes and reduced complications, including return to the operation theater.
Another advantage of using suture based fixation for olecranon fractures is the cost. Suture tape fixation has a significant cost advantage over TBW as most will end up being removed. Data obtained from our institute’s financial services, showed the average cost of suture tape fixation admission was $8734 (AUD) compared to $8830 (AUD) for TBW including implants. This cost increases with admission and theater costs for TBW removal, on average costing $5917 (AUD).
Limitations of this study include the relatively small number of high-quality studies available with a small subject size in each study. The biomechanical studies stripped most of the soft tissues from the elbow that may have provided further stability in real human trials, maintaining reduction with cyclic loading post-surgery. The heterogeneity between studies with different outcome measures made consensus on the ideal material difficult. However, various biomechanical and human case series data suggest that fixation with FiberWire with or without suture anchors provides fracture fixation similar to TBW without the associated complications.
Conclusions
High-strength braided sutures can be a valid alternative for treating simple displaced olecranon fractures in the elderly where tension band wire would have been otherwise appropriate. We recommend bone tunnel fixation with a flat-braided suture. In addition, cumulative results from this systematic review suggest that this type of technique can reduce the rate of reoperation to remove traditional metalwork reducing healthcare costs. More high-quality randomized control human trials need to be performed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.