
Abstract
Objective
To describe the surgical technique and evaluate the clinical efficacy of all-arthroscopic knotless anchor repair for talar-sided anterior talofibular ligament tears in the treatment of chronic lateral ankle instability.
Methods
This retrospective case series included 11 patients treated between February 2020 and October 2022. All patients presented with persistent lateral ankle pain and instability following an ankle sprain that did not respond to at least 6 months of conventional conservative management. Preoperative assessment included physical examination (positive anterior drawer and varus stress tests) and magnetic resonance imaging, which verified talar-sided anterior talofibular ligament insertion tears. The procedure was performed under complete arthroscopic visualization. Initially, the ankle joint was debrided to remove hyperplastic synovium and loose bodies. Then, the anterior talofibular ligament was tensioned using a suture tape passed through a two-wire loop sleeve. Finally, the ligament was secured with an absorbable knotless anchor implanted at the anatomical talar insertion site of the anterior talofibular ligament.
Results
All 11 patients were followed up for a mean duration of 13.27 ± 2.41 months. At the final follow-up, significant clinical improvements were observed compared with the preoperative status: the American Orthopaedic Foot and Ankle Society Ankle–Hindfoot score increased from 42.62 ± 2.2 to 95.73 ± 1.43 (p < 0.001), and the pain score on a visual analog scale decreased from 6.47 ± 1.25 to 1.73 ± 1.26 (p < 0.001). No postoperative complications occurred, including wound infection, cutaneous nerve injury, or recurrent ankle instability. All patients reported improved ankle stability and returned to daily activities without significant limitation.
Conclusion
For patients with chronic lateral ankle instability caused by talar-sided anterior talofibular ligament insertion tears, all-arthroscopic knotless anchor repair results in minimal surgical trauma, enables safe and reliable anatomical restoration of the ligament, and yields satisfactory short-term functional outcomes and pain relief. However, given the limitations of the retrospective case series design, including a small sample size and lack of a control group, further prospective studies with larger cohorts are needed to validate its long-term efficacy.
Keywords
Introduction
Ankle sprains typically result from excessive plantar flexion and varus of the ankle, 1 with tears of the anterior talofibular ligament (ATFL) predominantly localized to either the fibular or talar insertion site. Most acute ankle sprains resolve with conservative interventions, such as ankle bracing and physical rehabilitation. However, approximately 15%–20% of patients eventually progress to chronic lateral ankle instability (CLAI). 2 For patients who experience persistent pain and recurrent sprains despite 6–9 months of conservative treatment, surgical intervention is indicated. Surgical approaches for CLAI are categorized into anatomical repair, nonanatomical reconstruction, and anatomical reconstruction. 3 The open modified Broström–Gould procedure has long been regarded as the “gold standard” for lateral malleolar ligament stabilization 4 ; it is particularly effective for treating fibular-sided ATFL tears, whereas literature on talar-sided ATFL tears remains limited.
In recent years, there has been a growing body of literature on arthroscopic or arthroscopically assisted lateral ligament repair, 5 with multiple techniques available for arthroscopic ATFL repair. 6 These include anchor suture repair—where sutures are passed through the ligament and secured with knots—and subcutaneous suturing of the ATFL to the extensor retinaculum with knot fixation. 7 However, such knots often cause local soft tissue irritation; furthermore, passing sutures through the extensor retinaculum carries the risk of entrapping the superficial peroneal nerve, extensor digitorum longus tendon, or third peroneal tendon. Notably, anchor tails and knots placed on the talar side are prone to impinging on the medial malleolus, which may lead to restricted ankle joint mobility. 8 In the present study, knotless anchors were used for ligament repair to avoid nerve injury and knot-related complications associated with arthroscopic procedures. From February 2020 to October 2022, we performed all-arthroscopic knotless anchor repair on 11 adult patients with CLAI, yielding satisfactory clinical outcomes. The details are reported as follows.
Materials and methods
This retrospective case series study was approved by the Ethics Committee of Wuhan Fourth Hospital (Approval No.:KY2025-160-01) and conducted in accordance with the Declaration of Helsinki (1975, revised 2024). Given the retrospective nature of the study, written informed consent was waived by the ethics committee. All personally identifiable patient information was de-identified (e.g. removal of names, medical record numbers, and dates of birth) to protect privacy.
Indications and contraindications
Indications
The indications for all-arthroscopic repair of talar-sided ATFL insertion tears include the following: (a) persistent lateral ankle pain and instability following an ankle sprain; (b) failure to respond to conventional conservative treatment (including physical therapy, ankle bracing, and oral anti-inflammatory medications) for more than 6 months; (c) positive preoperative findings on the anterior drawer test and varus stress test (consistent with lateral ankle instability); and (d) confirmation of a talar-sided insertion tear of the ATFL on magnetic resonance imaging (MRI).
Contraindications
The following conditions represent contraindications this all-arthroscopic repair technique: (a) a history of lateral malleolar ligament repair or reconstruction surgery; (b) severe ATFL injury (e.g. complete ligamentous attrition or irreparable tissue damage); (c) generalized ligamentous laxity (e.g. Ehlers–Danlos syndrome or hypermobility spectrum disorder); (d) isolated subtalar joint instability (without concurrent ATFL injury); (e) body mass index (BMI) >25 kg/m2; (f) fibular tubercle larger than 1 cm (assessed via preoperative computed tomography (CT)); (g) systemic conditions that contraindicate surgery (e.g. uncontrolled diabetes mellitus, active infection, or coagulation disorders); and (h) preexisting nerve palsy or muscle dysfunction of the affected lower limb.
Preoperative preparation
All patients received low-molecular-weight heparin (LMWH) for thromboprophylaxis, with dosage adjusted based on body weight, 24 h before surgery. Surgery was performed only if preoperative assessment confirmed satisfactory soft tissue conditions, defined as no signs of skin erythema, edema, or infection around the ankle. Preoperative imaging included weight-bearing ankle radiographs to rule out bony deformities, CT to evaluate fibular tubercle size and bony anatomy, and MRI to confirm ATFL tear location and assess associated intraarticular pathologies. MRI revealed an avulsion of the talar-sided attachment of the ATFL (Figure 1(a)).

Imaging and arthroscopic views of the surgical procedure. (a) Preoperative MRI reveals a rupture of the ATFL at its talar insertion. (b) Arthroscopic view confirms avulsion of the ATFL from the talar footprint, with evident ligament laxity. (c) A suture passer is introduced from inferior to superior, carrying a looped suture. (d) The suture is woven through the ligament and tensioned. (e) A knotless anchor secures the ATFL to its native talar insertion point and (f) final arthroscopic assessment using a probe confirms appropriate ligament tension and stability after repair. ATFL: anterior talofibular ligament; MRI: magnetic resonance imaging.
Anesthesia and position
All procedures were performed by a single fellowship-trained orthopedic surgeon specializing in foot and ankle surgery. Anesthesia was administered as either combined spinal–epidural (CSE) or general anesthesia, based on patient preference and medical status. A pneumatic tourniquet was applied to the proximal thigh of the affected limb and set to 250 mmHg to maintain a bloodless surgical field.
Following anesthesia induction, the patient was placed in a supine position on the operating table. No joint distraction device was used. A sandbag was placed under the ipsilateral hip to achieve 10°–15° of internal rotation of the affected ankle, and the ankle was positioned at the edge of the table to maximize surgical access to the lateral compartment.
Surgical operation
All surgical procedures were performed using a standardized set of arthroscopic instruments, with detailed specifications provided to ensure methodological reproducibility. A 4.0-mm 30° arthroscope (Arthrex, Naples, FL, USA) was used for all procedures. Standard anteromedial (2 cm medial to the tibialis anterior tendon, at the level of the ankle joint line) and anterolateral (2 cm lateral to the peroneus tertius tendon) portals were established using a sharp trocar. An accessory lateral portal, located 1 cm distal to the anterolateral portal, was created to facilitate suture passing and anchor placement.
First, hyperplastic synovial tissue in the ankle joint was debrided using a 3.5-mm full-radius shaver (Arthrex) to optimize visualization of the lateral gutter and ATFL footprint. The lateral gutter was then cleared of fibrous adhesions, and a small segment (approximately 5 mm) of the distal fascicle of the inferior tibiofibular ligament (Bassett’s ligament) was resected to improve exposure of the distal fibula and lateral talus. Figure 1(b) provides an arthroscopic view confirming the avulsion of the ATFL from the talar footprint, with evident ligament laxity.
Subsequently, a curved 70° MicroSuture Lasso suture passer (Arthrex) was introduced through the accessory lateral portal. As shown in Figure 1(c), the passer was advanced from inferior to superior, carrying a looped 2-0 nonabsorbable braided suture (FiberWire, Arthrex), and passed through the torn end of the ATFL. The suture was retrieved, pulling both limbs through the ligament to form a “lasso” configuration. Figure 1(d) illustrates the suture being woven through the ligament and tensioned.
The talar footprint of the ATFL was then prepared using a shaver and radiofrequency ablation (Arthrex VAPR Plus) to remove residual fibrocartilaginous tissue and create a bleeding cancellous bone surface, thereby promoting biological tendon–bone healing. With the ankle maintained in 5°–10° of dorsiflexion and neutral rotation to restore physiological ligament tension, a 2.4-mm drill bit was used to create a pilot hole at the center of the prepared talar footprint. The suture limbs were manually tensioned to reduce the ATFL to its anatomical footprint, and a 3.0-mm bioabsorbable knotless anchor (SwiveLock RS, Arthrex) was inserted into the pilot hole to securely fix the ligament, as depicted in Figure 1(e).
Finally, Figure 1(f) shows the postoperative arthroscopic assessment using a probe, confirming appropriate ligament tension and stability following the repair.
Intraoperative assessment of ATFL tension and ankle stability was performed using a 2.7-mm arthroscopic probe to test ligament tautness and the anterior drawer test to assess anterior translation of the talus relative to the tibia. Excess suture tails were trimmed under direct arthroscopic visualization using a suture cutter (Arthrex). All portals were closed with 4-0 absorbable monofilament sutures (Vicryl, Ethicon, Somerville, NJ, USA), and the ankle was immobilized in a neutral position with a compressive elastic dressing and a short-leg non-weight-bearing plaster cast.
Postoperative treatment
All patients received prophylactic antibiotics (cefazolin sodium, 1 g intravenously) for 24–48 h postoperatively to prevent surgical site infection. A short-leg non-weight-bearing plaster cast was applied immediately after surgery and maintained for 2 weeks. Partial weight-bearing, at approximately 50% of body weight and assisted by crutches, was initiated at the end of the second postoperative week, with gradual progression to full weight-bearing by the fourth week.
Rehabilitation training was standardized and initiated at 4 weeks postoperatively:
Clinical data
Baseline characteristics
This study included 11 patients (6 males, 5 females) with a mean age of 25.32 ± 1.35 years (range: 19–48 years). All patients were diagnosed with CLAI based on the following criteria:
Persistent lateral ankle pain and instability for more than 6 months despite standardized conservative treatment, including physical therapy, ankle bracing, and oral nonsteroidal anti-inflammatory drugs; Positive preoperative anterior drawer test, defined as anterior talar translation >5 mm relative to the tibia, and varus stress test, defined as talar tilt >10° compared to the contralateral ankle; Preoperative imaging confirming CLAI: weight-bearing ankle radiographs ruled out ankle or hindfoot malalignment; CT excluded fibular tubercle hypertrophy (>1 cm) or bony lesions; MRI verified talar-sided ATFL insertion tears and ruled out significant calcaneofibular ligament injury or osteochondral lesions (grade ≥3).
Short-term outcomes
This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist. 9 Statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) version 20.0 software (IBM Corp., Armonk, NY, USA). Continuous variables, including age, follow-up duration, and functional scores, were presented as mean ± SD. Comparisons of preoperative and postoperative functional scores were conducted using paired t-tests, with a significance level set at α = 0.05.
All 11 patients completed follow-up, with a mean follow-up duration of 13.27 ± 2.41 months (range: 12–35 months). No patient was lost to follow-up. Significant improvements in functional outcomes were observed at the final follow-up compared with baseline:
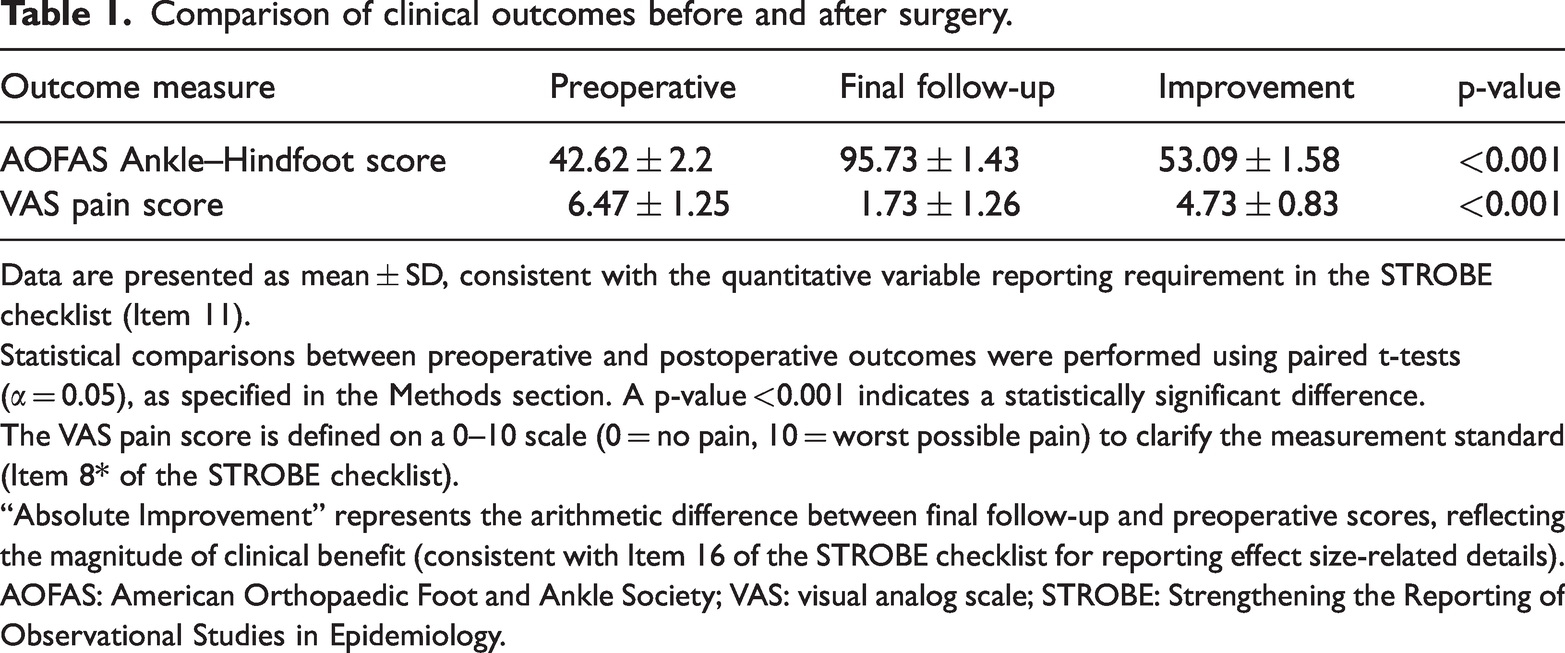
The American Orthopaedic Foot and Ankle Society (AOFAS) Ankle–Hindfoot Score increased from 42.62 ± 2.24 preoperatively to 95.73 ± 1.43 postoperatively (p < 0.001). Comparison of clinical outcomes before and after surgery. Data are presented as mean ± SD, consistent with the quantitative variable reporting requirement in the STROBE checklist (Item 11). Statistical comparisons between preoperative and postoperative outcomes were performed using paired t-tests (α = 0.05), as specified in the Methods section. A p-value <0.001 indicates a statistically significant difference. The VAS pain score is defined on a 0–10 scale (0 = no pain, 10 = worst possible pain) to clarify the measurement standard (Item 8* of the STROBE checklist). “Absolute Improvement” represents the arithmetic difference between final follow-up and preoperative scores, reflecting the magnitude of clinical benefit (consistent with Item 16 of the STROBE checklist for reporting effect size-related details). AOFAS: American Orthopaedic Foot and Ankle Society; VAS: visual analog scale; STROBE: Strengthening the Reporting of Observational Studies in Epidemiology.
No postoperative complications were reported, including surgical site infection, cutaneous nerve injury (superficial peroneal or sural nerve), wound dehiscence, or recurrent ankle instability. All patients reported subjective improvement in ankle stability at the final follow-up, with no restrictions on activities of daily living.
Discussion
For patients with CLAI who fail conservative management, surgical intervention is indicated to alleviate symptoms and restore pre-injury function capacity. The open modified Broström–Gould procedure has long been regarded as the “gold standard” for anatomical ligament repair10,11; however, recent technical advancements have established all-arthroscopic techniques as a viable and increasingly popular alternative, particularly for cases involving concomitant intraarticular pathologies, which are a limitation of the traditional open approach. 12
Although preoperative MRI demonstrates high specificity in identifying instability and chondral lesions, its sensitivity remains limited, especially for low-grade articular cartilage injuries. This diagnostic gap underscores the value of diagnostic arthroscopy, which enables direct visualization for accurate evaluation of intraarticular pathologies and targeted treatment in symptomatic patients with inconclusive preoperative imaging.13,14 Since the first report of arthroscopic lateral ligament repair in 1987, this approach has evolved into a well-established option for CLAI. The core indications for arthroscopic intervention include persistent symptoms despite 6 months of standardized conservative treatment, with surgical goals focused on pain relief, joint stabilization, and functional restoration.
Compared with open surgery, the all-arthroscopic approach offers distinct advantages. Most notably, it allows for the detection and simultaneous management of associated intraarticular pathologies, such as talar cartilage damage, synovitis, and loose bodies, which are present in over 90% of CLAI cases. 15 Consistent with the findings of Guelfi et al., 5 this technique is associated with shorter operative times, reduced postoperative pain and swelling, and minimized soft tissue trauma.15,16 The smaller incisions and limited soft tissue dissection also facilitate safer and earlier initiation of rehabilitation, with short- to medium-term clinical outcomes comparable to those of the open modified Broström–Gould procedure.17,18 Our postoperative rehabilitation protocol—including weight-bearing initiation at 2 weeks, range-of-motion training at 4 weeks, and gradual return to functional activities at 8–12 weeks—was developed in alignment with recommendations from the clinical practice guidelines for rehabilitation following surgical management of CLAI, 19 which emphasize evidence-based progression of load-bearing and motor training to optimize tendon–bone healing while minimizing re-injury risk. Notably, the significant improvements in AOFAS Ankle–Hindfoot scores and VAS pain scores observed in our patient series not only reflect the efficacy of the knotless anchor technique but also validate the rationality of our guideline-informed rehabilitation strategy. 12 The observed clinical improvements, in the absence of a control group, may partially reflect the combined effects of natural history, placebo effects, and the structured postoperative rehabilitation protocol.
Preoperative assessment is critical to identify contraindications for arthroscopic repair. Absolute contraindications include ankle or hindfoot malalignment, significant peroneal muscle weakness, isolated subtalar instability, advanced ankle osteoarthritis, systemic connective tissue disorders, or morbid obesity. Relative contraindications include a history of failed prior lateral ligament repair and excessively high patient expectations regarding postoperative function. From a biomechanical perspective, cadaveric studies have confirmed that arthroscopic knotless anchor repair achieves stability equivalent to that of open techniques, 20 supporting its reliability for anatomical ligament restoration.
Nevertheless, ankle arthroscopy is not without risks, with an overall complication rate ranging from 5.3% to 29%.21,22 The most common complications include iatrogenic nerve injuries involving the superficial peroneal or sural nerve and implant-related soft tissue irritation. Mitigating these risks requires surgical proficiency, thorough anatomical knowledge of the ankle’s neurovascular structures, precise portal placement, and appropriate use of specialized instruments. Existing arthroscopic techniques, such as Takao’s knotted suture repair 23 and Mangone’s percutaneous anchor fixation, 24 carry inherent risks of nerve entrapment, tendon injury, and knot-related soft tissue irritation. In contrast, the knotless anchor fixation technique used in our study simplifies the surgical workflow by eliminating the need for secondary suture passes and intraarticular knot tying, which reduces operative time and minimizes soft tissue irritation. 25 This advantage is particularly pronounced in talar-sided ATFL avulsion injuries, where limited access near standard arthroscopic portals makes knot placement technically challenging and increases the risk of iatrogenic injury. Intraoperative attention to ligament tension is paramount to successful repair. The reparability of the ATFL is determined by assessing ligament quality via gentle traction with the ankle in a neutral position; severely attenuated or deficient ligaments (e.g. due to chronic attrition) are not amenable to primary repair and thus represent a contraindication for this technique.
It is important to acknowledge the limitations of our study. First, the small sample size (n = 11), single-center retrospective design, and lack of a priori sample size calculation may compromise statistical power and introduce selection bias, limiting the generalizability and certainty of our findings. Second, the absence of a control group, such as open repair or other arthroscopic techniques, precludes direct comparison of efficacy or safety outcomes. Third, the mean follow-up duration of 13 months is insufficient to evaluate the long-term durability of the repair or the risk of late complications, including posttraumatic osteoarthritis. Finally, postoperative functional assessments were performed by the operating surgeons, who were not blinded to the surgical technique, introducing the potential for assessment bias. Due to these limitations, further prospective studies with larger cohorts are needed to validate the long-term efficacy of all-arthroscopic knotless anchor repair for talar-sided ATFL tears.
In conclusion, the all-arthroscopic knotless anchor technique for talar-sided ATFL insertion tears provides reliable mechanical stability, reduces the risk of nerve injury and knot-related complications, and enables early postoperative rehabilitation. This approach effectively restores ankle stability in selected patients with CLAI and represents a promising advancement in arthroscopic foot and ankle surgery. Future prospective, multicenter studies with larger sample sizes, control groups, and extended follow-up (≥24 months) are warranted to further validate its long-term efficacy and safety.
Footnotes
Acknowledgments
Not applicable.
Authors’ contributions
Ruo-kun Huang designed this retrospective clinical study and modified the manuscript. Feng Liu drafted the manuscript and contributed to the analysis and interpretation of the data. Hao Pan performed the data analysis. All authors read and approved the final manuscript.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
Ethical approval for this retrospective study was obtained from the Ethics Committee of Wuhan Fourth Hospital (KY2025-160-01).
Funding
No funding was received for this research.
Patient consent for publication
Not applicable.