
Abstract
Introduction:
Hip fractures are a significant economic burden to our healthcare system. As there have been efforts made to create an alternative payment model for hip fracture care, it will be imperative to risk-stratify reimbursement for these medically comorbid patients. We hypothesized that patients readmitted to the hospital within 90 days would be more likely to have a recent previous hospital admission, prior to their injury. Patients with a recent prior admission could therefore be considered higher risk for readmission and increased cost.
Methods:
A retrospective chart review identified 598 patients who underwent surgical fixation of a hip or femur fracture. Data on readmissions within 90 days of surgical procedure and previous admissions in the year prior to injury resulting in surgical procedure were collected. Logistic regression analysis was used to determine if recent prior admission had increased risk of 90-day readmission. A subgroup analysis of geriatric hip fractures and of readmitted patients were also performed.
Results:
Having a prior admission within one year was significantly associated (p < 0.0001) for 90-day readmission. Specifically, logistic regression analysis revealed that a prior admission was significantly associated with 90-day readmission with an odds ratio of 7.2 (95% CI: 4.8-10.9).
Discussion:
This patient population has a high rate of prior hospital admissions, and these prior admissions were predictive of 90-day readmission. Alternative payment models that include penalties for readmissions or fail to apply robust risk stratification may unjustly penalize hospital systems which care for more medically complex patients.
Conclusions:
Hip fracture patients with a recent prior admission to the hospital are at an increased risk for 90-day readmission. This information should be considered as alternative payment models are developed for hip fracture care.
Introduction
Hip fractures in elderly patients are an increasingly significant economic burden to our healthcare system. The current cost of hip fracture treatment has been approximated as 10 to 15 billion dollars per year and has been estimated to increase to 240 billion dollars by the year 2040 as the population ages. 1,2 Bundled payment models have been proposed to help reduce this cost. These payment models include patients under certain Diagnosis Related Groups (DRGs) and set a target reimbursement based off of historical cost data for an “episode of care”. This is inclusive of all costs of testing, procedures and post-acute care, including readmissions within 90 days to the hospital. The purpose of these models is to provide an incentive for hospitals and physicians to improve quality of care and decrease costs. Bundled payment models, such as the comprehensive care for joint replacement (CJR) model, have shown promising early results for cost savings. 3,4 One issue, however, with the CJR bundle is that it includes elective arthroplasty patients as well as patients undergoing arthroplasty for hip fractures (DRG 469 and 470). The difference in these populations has led to the CJR bundle risk stratifying arthroplasty patients by including an arthroplasty for fracture modifier. 5 This was a result of multiple studies showing a higher rate of readmission, complication, non-home discharge and increased length of stay in arthroplasty for hip fracture patients compared to elective arthroplasty patients. 6 -8 The same factors that led to this separation should be considered as attention is directed towards creating a separate hip fracture bundle.
The surgical hip and femur fracture treatment (SHFFT) bundle was previously proposed to apply the bundled payment model to the treatment of femur fractures including hip fractures (DRG 480, 481, 482). The SHFFT bundle was cancelled due to concerns related to applying the bundled payment model, which was intended for elective arthroplasty, to fracture care. These concerns were mainly because of a lack of risk stratification for these non-elective patients with multiple medical comorbidities. 9 -11 Mahure et al. (2017) demonstrated that varying patient comorbidities led to a wide range of costs for femur fracture treatment. 10 Cairns et al. (2018) reported that payments varied significantly depending on age, co-morbidities, demographic factors, geographic factors and surgical procedure. These authors recommend risk-adjusting bundled payments for hip fractures accordingly. 11
One component of risk stratifying hip fracture patients would be identifying those at highest risk of readmission. Readmission following hip fracture is a common and costly issue that has been extensively studied. Prior studies have shown a readmission rate of up to 32%; of these, as high as 89% are due to nonsurgical diagnoses. 12,13 Kates et al. (2015) found that the average cost of a readmitted patient treated for a hip fracture was over $14,000. 14
Previous studies have not considered the frequency of prior hospital admissions as a risk factor for 90-day readmission in hip fracture patients. Patients recently admitted to the hospital prior to their hip fracture may represent a subgroup that is especially prone to hospital readmission and therefore increased costs under a bundled payment model. The recent interest in applying risk stratification to a potential hip fracture bundle has made identifying these high-risk patients particularly relevant.
This study retrospectively investigated readmissions and prior admissions for patients surgically treated for hip and femur fractures. It was hypothesized that patients recently admitted to the hospital prior to their fracture would be more likely to be readmitted in the 90 days following surgery.
Methods
Patient Selection
Institutional Review Board approval was obtained for this retrospective study with a waiver of informed consent. Patients were included who underwent surgical fixation of hip and femur fractures between February 2012 and February 2017. These patients were identified by current procedural terminology (CPT) code. Codes included surgical procedures for femur fractures including hip fractures and are representative of DRG 480-482 (hip and femur procedures except major joint), intending to replicate the population that would have been included in the SHFFT bundle. All surgeries were performed by one of 2 trauma fellowship trained orthopedic surgeons at a single institution.
Data Collection
Demographic data, type of fracture, type of surgery and the presence of major medical comorbidities were collected for all patients. It was also recorded whether or not the patient was readmitted within 90 days and whether or not the patient had been admitted to this hospital within one year before their injury. These admissions were identified through a completed history and physical in the electronic medical record. Patient’s readmission diagnoses were classified as either surgical or nonsurgical (medical). Surgical diagnoses were defined as those that could be directly related to the surgical procedure. The complete list of surgical and non-surgical diagnoses can be found in Figures 1 and 2. For readmitted patients that also had a prior admission it was recorded if their readmission diagnosis was the same as their prior admission diagnosis. Additional variables collected included the development of a nosocomial infection, oral anticoagulation prior to admission, time greater than 24 hours to surgery, blood transfusion requirement, and length of stay. These factors were collected from their hospitalization at the time of their surgery to assess other variables that may be associated with readmission. Collected data was stored on the RedCap electronic data capture system. 15

Medical readmission diagnoses (n = 121). Abbreviations: Urinary tract infection (UTI), Altered mental status (AMS), Acute kidney injury/Chronic kidney disease (AKI/CKD), Gastrointestinal bleed (GI bleed), Chronic obstructive pulmonary disease (COPD), Congestive heart failure (CHF), myocardial infarction (MI), cerebrovascular accident (CVA).

Surgical readmission diagnoses (n = 40). Abbreviations: Deep Venous Thrombosis (DVT), Pulmonary Embolism (PE).
Statistical Analysis
The primary outcome measure was whether a prior admission within one year was associated with 90-day readmission. Secondary outcome measures included determining if additional variables collected were associated with 90-day readmission. Bivariate statistics compared patients that were readmitted within 90-days after surgery with those that were not. Specifically, categorical variables were analyzed using chi-squared statistics and continuous variables were analyzed using t-test statistics; non-parametric testing was used as appropriate. Continuous variables were tested for normality using a Shapiro-Wilk test. A p-value less than 0.05 was considered statistically significant. Subgroup analysis was also performed for the geriatric hip fracture population, which was defined as patients age >60 years, undergoing treatment of a peri-trochanteric or femoral neck fracture sustained from a low energy mechanism. Another subgroup analysis was performed for all 90-day readmission cases to compare medical versus surgical readmissions.
Binomial logistic regressions were performed to determine the effects of specific variables on the likelihood that the patient would have a 90-day readmission and, if so, the likelihood of having a medical readmission. Variables were considered for inclusion in the model in a hierarchical manner (lowest p-value first) based on bivariate statistical significance (p < 0.15) and kept within the model if the adjusted p-value was less than 0.3. Ninety-five percent confidence intervals (95% CI) are calculated for odds ratios within the regression models.
Results
A total of 635 patients were identified and reviewed for this study. After review, 37 patients were excluded due to undergoing prophylactic fixation of the femur, without having a femur fracture. The remaining 598 patient charts were included, with 161 (26.9%) being readmitted within 90 days. Having a prior admission within one year was significantly associated (p < 0.0001) with 90-day readmission (Table 1). Out of the patients readmitted, 59.7% were admitted to the hospital within one year prior to their fracture. Only 16.7% of those not readmitted were admitted to the hospital within one year prior to their fracture. Additionally, for the readmission group, 43.8% of their prior admissions were for the same diagnosis as their eventual readmission.
Other patient factors significantly associated with having a 90-day readmission (p < 0.05) were the presence of Chronic Kidney Disease (CKD), Congestive Heart Failure (CHF), Chronic Obstructive Pulmonary Disease (COPD) and Hypertension (HTN). CKD and CHF were the comorbidities most strongly associated with a 90-day readmission (p ≤ 0.0026, Table 1). There was no significant association between the type of fracture or surgery and 90-day readmission. There was an increased prevalence of peri-trochanteric fractures and decreased prevalence of femoral shaft fractures in the readmission subgroup, however this was not statistically significant. Other demographic and comorbidity variables investigated were not significantly associated with readmission.
Bivariate Analysis Comparing Patients Who Were Readmitted and Not Readmitted.
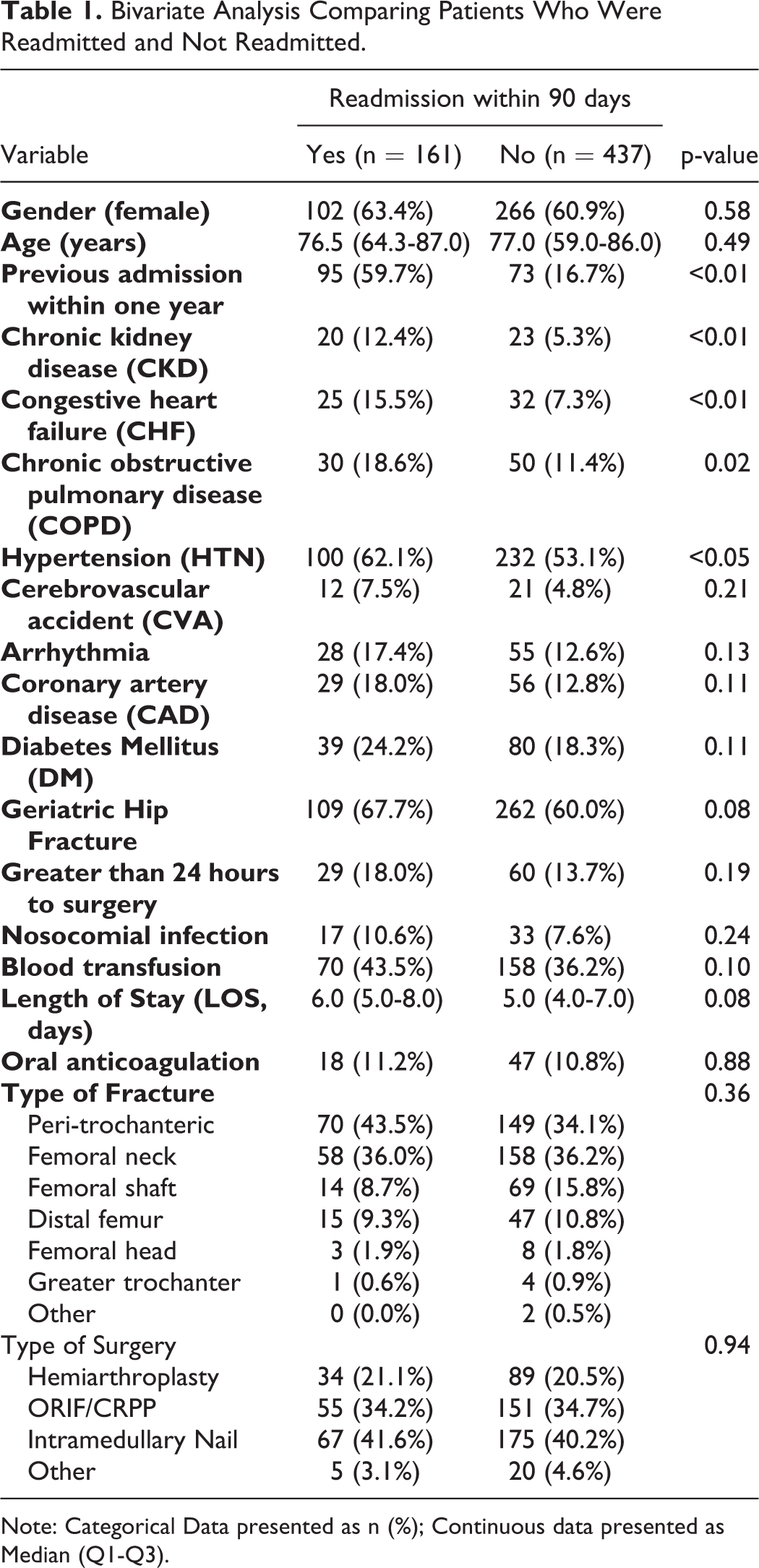
Note: Categorical Data presented as n (%); Continuous data presented as Median (Q1-Q3).
Multivariate logistic regression analysis revealed that having a prior admission within one year was a significant predictor (p < 0.0001) for 90-day readmission while adjusting for the presence of CKD and if the patient received a blood transfusion during their admission (Table 2); specifically, the odds of having a 90-day readmission were 7.2 (95% CI: 4.8-10.9) times higher if the patient had a prior admission within 1 year. No other parameter was included in the logistic regression due to a p-value >0.3.
Logistic Regression to Predict the Likelihood of Having a Readmission Within 90 Days.

Note: Variables are presence compared to absence, e.g. having chronic kidney disease compared to not having the disease.
Geriatric hip fractures occurred in 62% (=371/598) of the total population. Of this subgroup, 29.4% of patients were readmitted within 90 days. The non-geriatric hip fracture patients included 7 out of the 8 total patients readmitted for uncontrolled pain as well as 5 out of the 7 total patients readmitted for DVT. Out of the geriatric hip fracture patients with a 90-day readmission, 37.3% had the same diagnosis for readmission as for the previous admission within 1 year. Similar to the overall group, patients in the geriatric hip fracture subgroup with an admission in the past year were also significantly more likely to have a 90-day readmission with an odds ratio of 7.0 (95% CI: 4.2−11.5, p < 0.0001; Table 3).
Logistic Regression to Predict the Likelihood of Geriatric Patients Having a Readmission Within 90 Days.

Note: Variables are presence compared to absence, e.g. having a nosocomial infection compared to not.
The majority of the 90-day readmissions (n = 161) were related to medical diagnoses (75.2%) as opposed to surgical diagnoses (24.8%). Figures 1 and 2 show the rates of the different medical and surgical readmission diagnoses. In the geriatric hip fracture subgroup, 85.3% of the readmissions were for medical diagnoses and 14.7% were for surgical diagnoses. In addition, out of the patients readmitted within 90 days, 43.8% had the same diagnosis for the readmission as for the previous admission within 1 year. Subgroup analyses demonstrated that the odds of having a readmission for medical rather than surgical diagnoses was 4.2 (95% CI: 1.6-11.5) times higher for geriatric hip fracture patients and 4.7 (95% CI: 1.9-11.8) times higher for patients with a prior admission within one year (p < 0.005, Table 4). In addition, patients with hypertension had 3.3 times higher odds (95% CI: 1.3-8.5) of having a medical readmission diagnosis (p = 0.0125).
Logistic Regression to Predict the Likelihood of Having a Readmission Within 90 Days for a Medical Diagnosis as Opposed to a Surgical Diagnosis

Note: Categorical variables are presence compared to absence, e.g. having hypertension compared to not having the disease; ORIF—Open Reduction Internal Fixation; CRPP—Closed Reduction Percutaneous pinning.
Discussion
Identifying patients who are at higher risk for readmission after hip fracture surgery is an important aspect of developing an alternative payment model for hip fracture reimbursement. This study found that patients admitted to the hospital within one year prior to fracture were significantly more likely to be readmitted within 90 days of surgery. Early readmissions in this group may therefore be related more to the patient’s chronic medical co-morbidities than surgical complications. This is supported by the fact that a majority of patients (85% in the geriatric hip fracture subgroup) were readmitted for medical rather than surgical diagnoses. Furthermore, 44% of readmitted patients with a prior admission had the same diagnosis for their readmission as their prior admission. The 2 comorbidities most strongly associated with readmission were CHF and CKD. The presence of these comorbidities should prompt detailed preoperative and postoperative optimization in collaboration with medical services.
The data suggests that 90-day readmissions in this population are often caused by the patient’s overall health and comorbidities rather than factors controllable by the hospital or surgeon. Therefore, a hip fracture bundled payment model that includes 90-day readmissions may unjustly penalize hospital systems. In a recent review article, Malik et al. (2020) expressed their concern that the current structure of the BPCI model will create financial disincentives for providing care for the most medically complex patients. 5 This may result in some centers “cherry picking” healthier patients and transferring more medically complex patients to tertiary care centers. This would be unjust from a financial standpoint and would also delay patient care for a population that has increased complications and a higher mortality rate when care is delayed greater than 48 hours. 16 -18
A different approach towards developing an alternative payment model for hip fractures will have to be taken to ensure equal and timely care for hip fracture patients and fair reimbursement for hospital systems. Cairns et al. (2018) investigated variables involved in hip fracture reimbursement; they concluded that payments should be adjusted for age, comorbidities, demographic factors, geographic location and surgical procedure. 11 The specific comorbidities that were associated with the largest change in reimbursement in that study were COPD, CHF, DM, peripheral vascular disease (PVD), history of CVA, and CKD. 11 This correlates this study’s findings of CHF and CKD as comorbidities which were associated with the highest risk of readmission. This study is unique to the existing literature with regards to the finding that prior admission within one year was by far the most significant variable for predicting readmission. Existing comorbidities may contribute to the high association of patients’ previous admissions and those patients having a 90-day readmission. The findings in this study support the inclusion of recent prior admissions in risk stratification models.
The 90-day readmission rate in the overall patient group and geriatric hip fracture subgroup were similar at 27% and 29%, respectively. Readmission was due to non-surgical diagnoses in 75% of patients in the total study population, which was increased to 85% in the geriatric hip fracture subgroup. The readmission rates and rates of readmission for non-surgical diagnoses in our study were consistent with what has been previously reported in the literature. 12,13
Given the frequency of readmissions, and the high rate of readmissions unrelated to surgical factors, it may be more appropriate to remove readmission costs from the bundled payment model altogether. This is supported by the findings of Lott et al., who recently reported data before and after implementation of the BPCI bundle for the subset of arthroplasty patients that underwent arthroplasty for fracture. In that study readmission rates were similar before and after implementation of the bundle. The readmissions after the bundle was implemented in that study cost an average of $11,766 per readmission which corresponded to 24% of the total 90-day episode of care costs. 19
There are limitations to this study. The data is specific to this institution and the practices of the surgeons involved in the study. This was a retrospective chart review, subject to selection bias as well as missing or incomplete information in the EMR. Specifically, the chart review was only able to identify patients that were admitted to the hospital where this study took place. If a patient in the readmission population had been admitted to another hospital prior to their surgery, it would not be included in the data. This inconsistency in the data could mean the actual prior admission rate in the 90-day readmission population is higher than reported. One situation this study did not consider is patients with multiple prior admissions; future studies could investigate if there is further risk stratification with and increased number of recent admissions. An additional weakness is that this study simply looked at the presence of certain comorbidities, rather than investigating the total number of comorbidities or comorbidity scoring systems.
Conclusion
In conclusion, these findings should be considered as further efforts are made towards developing an alternative payment model for hip fractures. Reimbursement models should take into account patients with recent prior admissions to the hospital, as they are significantly more likely to have a 90-day readmission. In addition, readmissions and prior admissions are both relatively common in this patient population and are rarely due to surgical diagnoses. Rather than penalizing hospitals for readmissions, there are alternative aspects of hip fracture care that may be optimized to reduce healthcare spending.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.