
Abstract
Objectives:
The purpose of this study was to use a nationally representative database to determine the differences in 30-day outcomes based on procedure type for management of proximal humerus fractures including complications, readmission, operative time, and length of stay. Further, we sought to determine patient characteristics and perioperative factors associated with poor outcomes.
Design/Setting:
This was a retrospective study of the National Surgical Quality Improvement Program (NSQIP) database. The NSQIP comprises a clinical database with systematic patient tracking at multiple hospitals across the United States.
Patients:
A total of 413 patients with proximal humerus fractures managed surgically were included.
Intervention:
Of 413 patients, 330 underwent open reduction and internal fixation (ORIF) and 83 underwent hemiarthroplasty.
Main Outcomes/Measurements:
The primary end points included major and minor complications, operative time, rate of return to the operating room, and length of stay.
Results:
Compared to the hemiarthroplasty cohort, patients in the ORIF cohort were significantly younger (64.2; 17-90 and 69.3; 20-90, respectively, P = .007) and were significantly less likely to be of functionally dependent status (17.5% and 27.7%, P = .036). Compared to the hemiarthroplasty cohort, the ORIF cohort demonstrated fewer postoperative bleeding complications (2.4% and 8.4%, respectively, P = .016) and shorter operative times (115 vs 131 minutes, P = .017). There were no significant differences between the groups with respect to complications, reoperation rates, or length of hospital stay. On multivariable analysis, hemiarthroplasty demonstrated increased risk of postoperative bleeding compared to ORIF (odds ratio = 7.06, confidence interval: 2.06-24.24; P = .002) as well as increased operative time (P = .01).
Conclusions:
Patients who undergo hemiarthroplasty for management of proximal humerus fractures are significantly older and often functionally dependent. When compared to ORIF, hemiarthroplasty is associated with longer operative times and greater risk of bleeding complications.
Introduction
Fractures of the proximal humerus are common and represent a spectrum of injury ranging from low-energy osteoporotic fractures in the elderly patients to high-energy fracture–dislocations. 1,2 While low-energy, minimally displaced, or valgus-impacted fractures are often treated nonoperatively with a relatively low rate of nonunion, 3 displaced and comminuted fractures have a greater risk of malunion and nonunion of the humeral head. 4,5 These complications can lead to significant disability for patients, and many authors advocate for plate osteosynthesis or humeral hemiarthroplasty for displaced Neer 3- and 4-part fractures. 1,4,6 –11 Many surgeons suggest that young patients be treated with anatomic reduction and plate osteosynthesis in order to preserve bone stock and prevent glenoid erosion and arthrosis that could result from a hemiarthroplasty. However, no studies comparing open reduction and internal fixation (ORIF) to hemiarthroplasty in young patients (<50 years of age) exist. Debate remains whether ORIF or hemiarthroplasty is superior in adults with displaced Neer 3- and 4-part fractures and fracture–dislocations and few studies examine the difference in outcomes. 4,7,12 Recent studies suggest that reverse total shoulder arthroplasty (RTSA) for 3- to 4-part proximal humerus fractures may have improved outcomes and less failure rate compared to hemiarthroplasty. 13
When definitive scientific evidence advocating for a specific treatment regimen is lacking, surgical outcome databases are providing significant clinical information that may help guide surgeons. The National Surgical Quality Improvement Program (NSQIP) database is emerging as an important tool in evaluating patient characteristics and other factors associated with surgical complications, increased length of stay, prolonged operative times, and other problems that greatly influence patient outcome and compound health care costs. Previous work by Schilling et al 14 used the NSQIP database to identify the orthopedic procedures most associated with major complications. Several studies have subsequently evaluated these procedures using the NSQIP database to identify patient characteristics and surgical factors associated with an increased risk of postoperative complications. 15 –19 To our knowledge, there has been no reporting of early and late patient outcomes or incidence of complications using this database with regard to proximal humerus fractures in the literature. The goal of the present study is to use the NSQIP database to identify patient characteristics and surgical factors associated with surgical complications in 30 days following surgery with ORIF or humeral hemiarthroplasty for management of proximal humerus fractures. We hypothesize that hemiarthroplasty is being performed in older patients with fewer functional demands and that hemiarthroplasty is associated with a greater risk of surgical complications, readmission, and length of stay.
Methods
The American College of Surgeons NSQIP Participant User File comprises a clinical database with systematic patient tracking at hospitals that voluntarily participate. Sampling strategy, data abstraction, and included variables have been previously described. 20 In brief, rigid adherence to set protocols with interval auditing is a necessary component for participation. Dedicated nurse reviewers are trained to collect parameters until 30 days postoperatively including 60 preoperative patient characteristics, 18 intraoperative factors, and 22 postoperative occurrences (refer to http://site.acsnsqip.org/ for full list). 20
Inclusion criteria were adult patients (>16 years) sampled in NSQIP from 2005 to 2010 with common procedural terminology (CPT) codes for open reduction and plate fixation (CPT = 23615, 23680) or humeral hemiarthroplasty (CPT = 23616) for management of proximal humerus fractures. A total 414 patients met inclusion criteria, 1 patient was excluded due to extensive missing data. Variable-specific parameters within NSQIP relevant to this study are detailed subsequently. Age was evaluated as a linear variable. Race was defined as white, black, or other. Preoperative functional status specifies the patient self-care level for activities of daily living (ADLs) observed 30 days before surgery and was defined as dependent or independent. The ADLs include bathing, feeding, dressing, toileting, and mobility. Independent status is designated for patients who do not require assistance from another person for any ADLs, including patients who are able to function independently with prosthetics or equipment. Dependent status is designated for patients who require some assistance from another person for ADLs.
Preoperative comorbidities were grouped by organ system: cardiac comorbidity, neurological comorbidity, respiratory comorbidity, renal insufficiency, and hepatic insufficiency as described previously. 21 –23 American Society of Anesthesiology (ASA) Classification of disease status was grouped as III, IV, and V compared to I and II. The NSQIP data set provides wound classification in accordance with the Center for Disease Control as an assessment to the degree of surgical wound contamination at the time of operation. A wound class of I is designated for clean, II for clean/contaminated, III for contaminated, and IV for dirty/infected cases. Laboratory values were captured as the last recorded value within 90 days prior to surgery. Albumin and anemia were evaluated as categorical variables with thresholds of 3.5 g/dL and a hematocrit less than 36%. Preoperative transfusion was also evaluated using the parameter collected by NSQIP representing greater than 4 units of blood transfused within 72 hours prior to the index procedure. Bleeding disorder was defined as any condition putting the patient at risk of bleeding due to a deficiency in blood clotting elements, that is, vitamin K deficiency, hemophilia, thrombocytopenia, or use of chronic anticoagulants (not including aspirin) in the perioperative period.
Per the Clavien-Dindo complication classification schema, postoperative clinical complications were classified as major (Clavien-Dindo 3, 4, and 5) or minor (Clavien-Dindo 1 or 2) and identified by organ system. 24 The methodology for outcome classification has been previously published. More specifically, major complications were defined as life threatening or debilitating and included organ space infection, sepsis, postoperative bleed requiring transfusion, dependence on ventilator (reintubation or failure to wean), cardiac event, neurologic event, pneumonia, venous thromboembolic event, return to operating room (ROR), graft failure, or acute renal failure. The ROR was recorded as any unplanned major surgical procedure within the 30-day postoperative period that is a result of an adverse outcome related to the principal procedure. Minor complications were defined as incisional infection (superficial to the fascia) and urinary tract infection. Clinical characteristics were assessed for association with end points including major complications, postoperative bleeding, length of stay, and operative time.
Statistical Analyses
Bivariate analysis was performed using Student t-test or Pearson chi-square analysis as appropriate. Factors with P value <.1 were included in multivariable analysis. Significance for multivariable predictors of each end point was set at 2-tailed P value of .05. Model performance was assessed using Hosmer and Lemeshow test and a c-statistic for an ROC curve using the predicted probability compared to each end point. Binary logistic regression were used for categorical end points and multivariable linear regression was used for continuous end points. The multivariable models were optimized for covariate inclusion based on model fit and the c-statistic as described previously. A subanalysis of patients older than 50 years of age was also performed in order to determine whether procedure choice impacted patient outcome to a greater degree in this patient population. All analyses were carried out using IBM SPSS Statistics software, Version 19 (2010 SPSS, IBM Inc., Armonk, NY).
Results
A total of 413 patients were included for analysis: 330 patients underwent humeral fracture fixation (ORIF) and 83 patients underwent shoulder hemiarthroplasty for management of proximal humerus fracture. The patient characteristics are outlined in Table 1. Patients in the ORIF cohort were significantly younger than patients in the hemiarthroplasty cohort (64.2; 17-90 and 69.3; 20-90, respectively; P = .007) There was a statistically significant difference in the cohorts with respect to gender, with the ORIF cohort comprising more males compared to the hemiarthroplasty cohort. Patients in the ORIF cohort were significantly less likely to be of functionally dependent status and were also significantly less likely to have a preoperative neurologic comorbidity compared to patients in the hemiarthroplasty cohort. No significant differences in the groups were noted with respect to race, obesity, and other medical comorbidities including bleeding disorder, smoking status, transfer status, or rates of emergency cases.
Patient Characteristics.
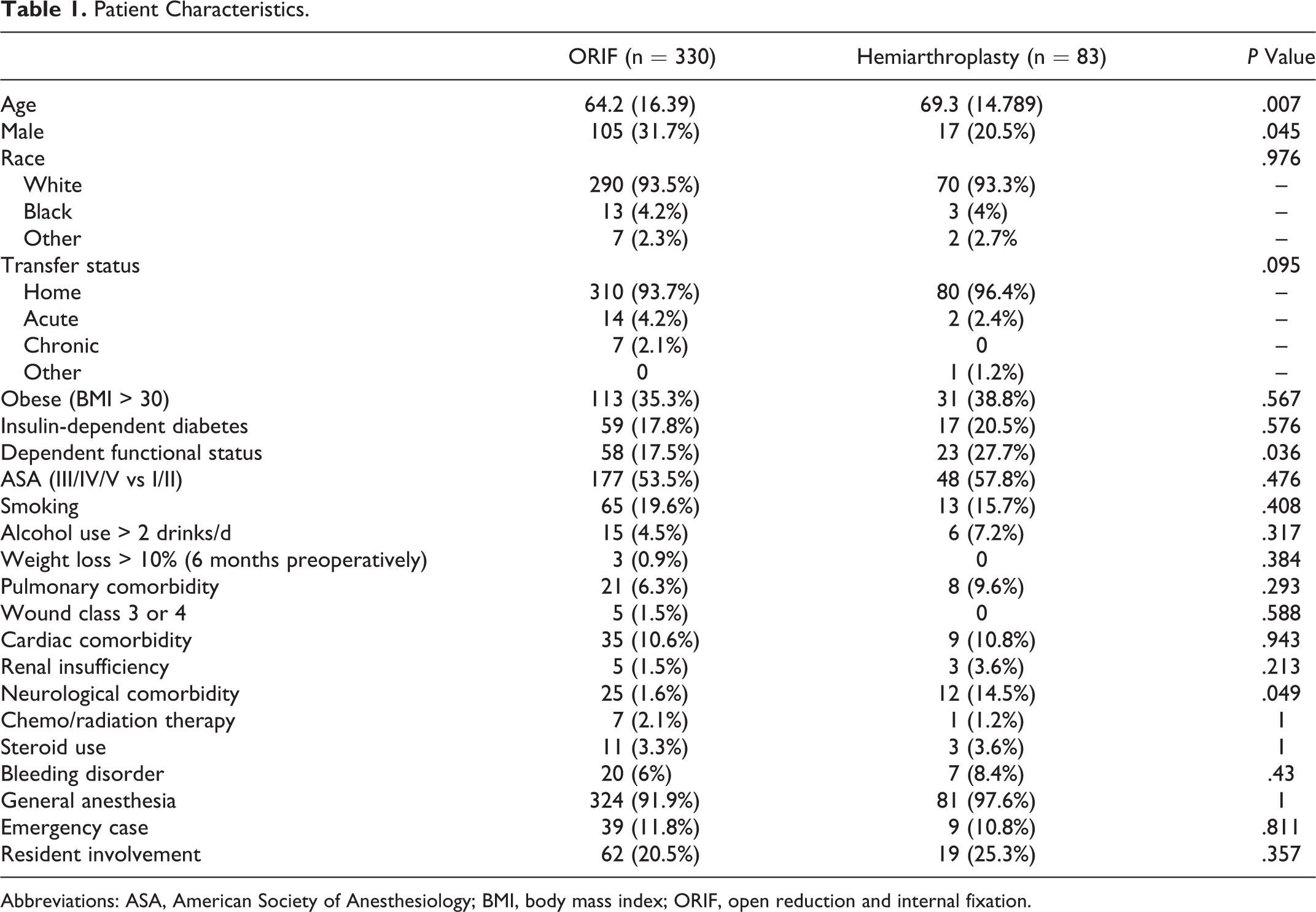
Abbreviations: ASA, American Society of Anesthesiology; BMI, body mass index; ORIF, open reduction and internal fixation.
Bivariate comparison of 30-day complication rates in patients managed with hemiarthroplasty and ORIF for proximal humerus fractures is presented in Table 2. The ORIF cohort demonstrated significantly fewer postoperative bleeding complications (8 patients, 2.4%) compared to the hemiarthroplasty cohort (7 patients, 8.4%; P = .016). Operative time was also significantly less in the ORIF cohort (115 minutes, standard deviation [SD] 57.4) compared to the hemiarthroplasty cohort (131 minutes, SD 43.8, P = .017). There were 4 deaths in the ORIF cohort (1.2%) and no deaths in the hemiarthroplasty cohort; this difference was not statistically significant. There were 23 (6.9%) major complications in the ORIF cohort and 7 (8.4%) major complications in the hemiarthroplasty cohort. There were no significant differences in the rates of major and minor complications, peripheral nerve injury, reoperation rates in the first 30 postoperative days, and total length of hospital stay.
Outcomes by Procedure Type.

Abbreviations: OR, odds ratio; ORIF, open reduction and internal fixation; SD, standard deviation.
On multivariable binary logistic regression, hemiarthroplasty was associated with an increased risk of postoperative bleed compared to ORIF (Table 3). Other independent predictors of postoperative bleed included preoperative transfusion and acute transfer from an outside designation as an emergency case trended toward significance.
Multivariable Analysis of Postoperative Bleeding.
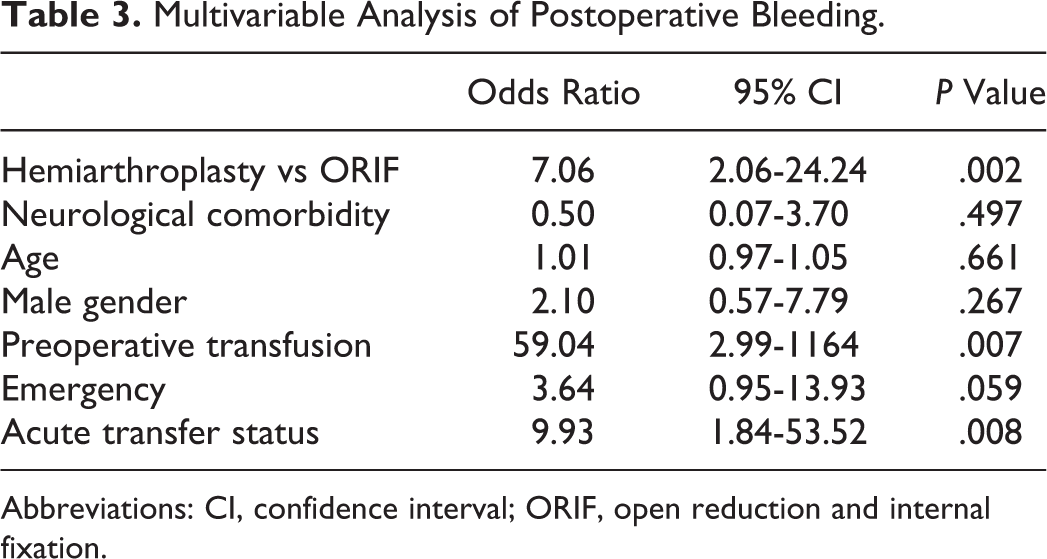
Abbreviations: CI, confidence interval; ORIF, open reduction and internal fixation.
Hemiarthroplasty was also associated with increased operative time compared to ORIF on multivariable analysis (P = .01; Table 4). The only other predictor of increased operative time was male gender.
Multivariable Analysis of Operative Time (Minutes).

Abbreviations: CI, confidence interval; ORIF, open reduction and internal fixation.
Hemiarthroplasty did not have a significant increase in major complications compared to ORIF on multivariable analysis (Table 5). Independent predictors of major complications include designation as an emergency case and a contaminated or dirty wound.
Multivariable Analysis of Major Complications.

Abbreviations: CI, confidence interval; ORIF, open reduction and internal fixation.
When limiting patients to 50 years of age and older, multivariable analysis demonstrated similar findings but with greater effect size. In this older cohort, there were 349 patients: 271 (77.7%) underwent ORIF and 78 (22.3%) underwent hemiarthroplasty. In regard to postoperative bleeding risk in older patients, hemiarthroplasty versus ORIF, preoperative transfusion status, and acute transfer status all demonstrated a larger associated risk of postoperative bleed when patients were limited to 50 years of age and older (Table 6). Hemiarthroplasty was again associated with increased operative time compared to ORIF, with stronger statistical significance (P < .001). Again, there was no significant difference in major complications between the ORIF cohort and the hemiarthroplasty cohort when limiting patients to 50 years of age and older. Designation as an emergency case and a contaminated or dirty wound again demonstrated a stronger association with major complications when limiting patients to 50 years of age and older.
Multivariable Postoperative Bleed Patients >50 Years of Age.
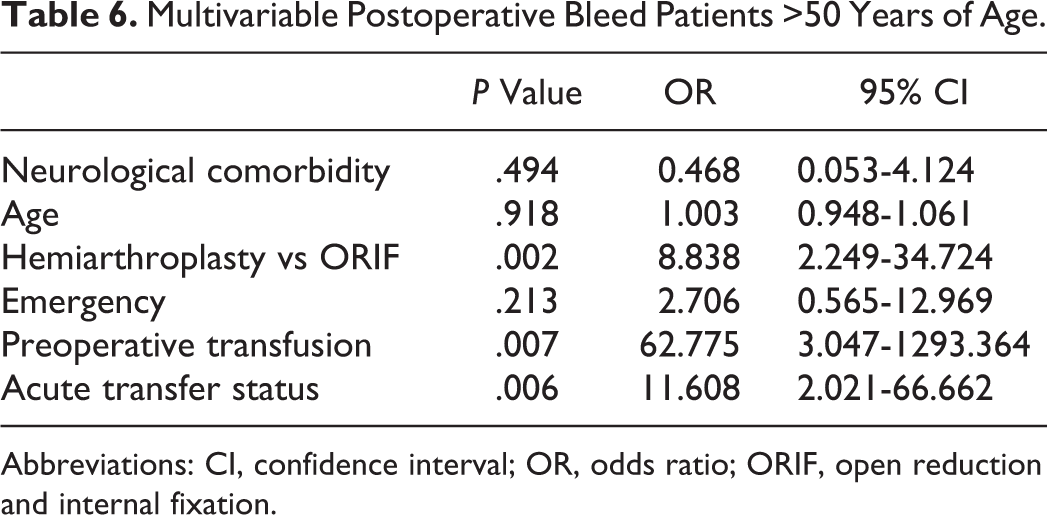
Abbreviations: CI, confidence interval; OR, odds ratio; ORIF, open reduction and internal fixation.
Discussion
With regard to patient characteristics, patients who underwent ORIF of proximal humerus fractures were significantly younger than those who underwent hemiarthroplasty (64.2 vs 69.3). This is consistent with other studies. 1,7,8,10,25 –37 This is expected, as younger patients typically have better bone quality than older patients and surgeons often elect for surgical fixation in younger patients regardless of fracture pattern. Older patients are expected to represent a larger population of the hemiarthroplasty group, as they not only have poorer bone quality but also have lower functional demands. Thus, they would not be expected to have the same functional impairments from the potential glenoid erosion and limited range of motion following a hemiarthroplasty as younger patients would. Patients who underwent ORIF were also more likely to be male, representing 31.7% of the ORIF cohort and only 20.5% of the hemiarthroplasty cohort. This is also consistent with the published literature. 1,7,8,10,25 –37 This may be partially explained by a lower likelihood of osteoporosis in male patients and thus better bone quality for adequate fixation with a plate and screw construct. Patients who underwent ORIF for their fractures were also significantly less likely to be of functional-dependent status as compared to patients who underwent hemiarthroplasty. The hemiarthroplasty cohort thus likely represents a larger fraction of patients who are older, have less active lifestyles, and are functionally dependent, suggesting that surgeons often elect for hemiarthroplasty in low-demand patients. Interestingly, there were no significant differences between the groups with respect to ASA score and comorbidities aside from neurologic, suggesting that the procedure of choice for these patients relies more so on age, functional status, and bone quality than on medical comorbidities.
To our knowledge, this is the first study to provide a comparison between these 2 cohorts with regard to multiple perioperative factors including length of stay, operative time, and bleeding complications. With regard to complications, the ORIF group demonstrated significantly less major bleeding complications (2.4%) compared to the hemiarthroplasty group (8.4%). After adjusting for patient differences, hemiarthroplasty remained associated with approximately 7 times the risk of a postoperative bleed compared to ORIF. Since there was no difference with regard to preoperative bleeding disorders between the groups, one possible explanation for this difference is the tamponade effect of anatomic fracture reduction in the ORIF group. As the NSQIP database suggests there are more fractures managed with ORIF than with hemiarthroplasty. Surgeon experience may explain the significantly increased operative time of hemiarthroplasty (131 minutes) compared to ORIF (115 minutes). However, despite a higher likelihood of a bleeding complication in the hemiarthroplasty group, there were no perioperative deaths, compared to 4 perioperative deaths (1.2%) in the ORIF group. This difference, however, was not statistically significant. Length of stay tended to be longer in the hemiarthroplasty group (3.1 days) compared to the ORIF group (2.4 days), but this difference was not significant (P = .098). On multivariate analysis, 2 variables were independently associated with major complications and included designation as an emergency case and the presence of a dirty or contaminated wound. Although not stated explicitly in the NSQIP database, dirty or contaminated wounds in orthopedic procedures are presumed to represent open fractures. There were no significant differences between the groups with respect to overall major or minor complications, including infection and neurovascular injury, or reoperation rates in the first 30 postoperative days. However, the incidence of complications was low in both the groups and a greater number of patients would likely need to be included in the analysis to detect true differences in complication rates.
There are several important limitations to the present study. The sample size is small, which may limit conclusions about the equivalency of ORIF and hemiarthroplasty particularly for differences in major complications. The follow-up is limited to 30 days only and the authors acknowledge that many complications may occur after the 30-day time period. Additionally, NSQIP combines high-energy and low-energy injuries together, which may complicate data analysis.
The choice between ORIF and hemiarthroplasty represents a selection bias of surgeon preference and other unmeasured patient factors that cannot be controlled for in NSQIP. Also, the NSQIP database does not record the fracture patterns but records the CPT code alone. Thus, the 2 cohorts may have dramatically different representations of the different fracture patterns, and so information regarding complications and other clinical parameters as they relate to fracture pattern cannot be ascertained from this study. The NSQIP database also provides no information on level of individual surgeon experience or subspecialty interest, which could significantly affect complication rates and operative time. Further, although complications including surgical site infection are included in the database, more orthopedic-related complications including implant-related complications are not specifically addressed in the database. Other important outcomes not addressed in this study include the use of rehabilitation facilities, functional outcomes, pain, and overall costs. Although functional outcomes and pain have been addressed in several studies comparing ORIF to hemiarthroplasty for the management of proximal humerus fractures, 4,7 no overall cost analysis has been performed. A cost analysis would be useful for these 2 procedures. Significant cost differences could influence the selection of the more cost-effective treatment. Further, because RTSA is becoming a popular treatment choice for management of these complex injuries, a separate analysis would have proved valuable for RTSA. However, this analysis is not possible using the NSQIP database as RTSA does not possess a unique CPT code with which to query the database.
Conclusion
To date, this is the largest report on proximal humerus fractures specifically evaluating predictors of short-term complications. This study has identified several important differences with respect to patient characteristics and outcomes when comparing ORIF to hemiarthroplasty for management of proximal humerus fractures. This knowledge may help clinicians counsel patients about potential risks of surgery. Patients who undergo hemiarthroplasty are significantly older, lower demand, and often functionally dependent, and the surgeon should anticipate longer operative times and potential bleeding complications. Knowledge of these factors should influence surgeons to be vigilant for blood loss and to identify social work needs early in the management of these patients. The ORIF is being performed on younger, more independent patients and was associated with lower bleeding complications and shorter operative times. Careful patient selection is paramount when choosing the appropriate treatment for these injuries.
Footnotes
Authors’ Note
This study was performed at University of Rochester Medical Center, Rochester, NY, USA. This manuscript is an original work that has never been published previously. It has been reviewed by all of the above-mentioned authors.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Ilya Voloshin is a paid consultant for “Zimmer,” “Pfizer,” and “Acumed.” This author receives speaking fees from “Arthrex” and “Acumed.” No other financial payments or benefits from any other commercial entity related to the subject of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Voloshin—Arthrex grant support, Dr Kates—Synthes Spine research grant paid to institution.