
Abstract
Introduction:
The Centers for Medicare and Medicaid Services removed total hip arthroplasty (THA) from the inpatient-only (IO) list in January 2020. Given this recommendation, we analyzed Medicare-eligible patients undergoing outpatient THA to understand risk factors for nonroutine discharge, reoperations, and readmissions.
Materials and Methods:
The 2015-2018 American College of Surgeons–National Surgical Quality Improvement Program database was queried using Current Procedural Terminology code 27130 for Medicare eligible patients (≥ 65 years of age) undergoing outpatient THA. Postoperative discharge destination was categorized into home and non-home. Multivariate logistic regression models were used to evaluate risk factors associated with non-home discharge disposition. Secondarily, we evaluated rates and risk factors associated with 30-day reoperations and readmissions.
Results:
A total of 1095 THAs were retrieved for final analysis. A total of 108 patients (9.9%) experienced a non-home discharge postoperatively. Patients were discharged to rehab (n = 47; 4.3%), a skilled care facility (n = 47; 4.3%), a facility that was “home” (n = 8; 0.7%), a separate acute care facility (n = 5; 0.5%), or an unskilled facility (n = 1; 0.1%). Independent factors for a non-home discharge were American Society of Anesthesiologists Class >II (odds ratio [OR] 2.74), operative time >80 minutes (OR 2.42), age >70 years (OR 2.20), and female gender (OR 1.67). Eighteen patients (1.6%) required an unplanned reoperation within 30 days. A total of 40 patients (3.7%) required 30-day readmissions, with 35 readmissions related to the original THA procedure. Independent risk factors for 30-day reoperation were COPD (OR 5.85) and HTN (OR 5.24). Independent risk factors for 30-day readmission were HTN (OR 4.35) and Age >70 (OR 2.48).
Discussion:
The current study identifies significant predictors associated with a non-home discharge, reoperation, and readmission in Medicare-aged patients undergoing outpatient THA.
Conclusion:
Providers should consider preoperatively risk-stratifying patients to reduce the costs associated with unplanned discharge destination, complication or reoperation.
Introduction
Although total joint arthroplasties (TJA) were historically performed in an inpatient setting, the rising costs of healthcare, coupled with advancements in peri-operative care, have urged surgeons to consider transitioning these procedures to the outpatient setting. 1 -3 Surgeons have the option of performing outpatient surgery in 2 distinct types of facilities—a hospital-owned outpatient facility (HOPD) or a free-standing ambulatory surgical center (ASC). The distinction between outpatient surgical settings is often minimal, however ASCs must comply with a “Covered Procedures List” to minimize risk in these operational settings. 4 As of 2020, the Centers for Medicare and Medicaid Services (CMS) removed total hip arthroplasty (THA) from the CMS inpatient only (IPO) list and added total knee arthroplasty (TKA) to the Ambulatory Surgical Centers (ASC) Covered Surgical Procedures List. 5 With numerous single institution and national database studies reporting the outcomes after TJA in outpatient surgery settings, these provided support for transitioning specific procedures outpatient to meet the exceeding demand. 3,6 -14
Outpatient TJA has been effectively and safely performed on select patients within the last decade. The 30- and 90-day complication rates and readmissions are low with the careful selection of patients. 15 For TJA, single institution, national database studies, and large systematic reviews have reported no significant difference in total complications, major complications, readmissions, and wound complications between the outpatient and inpatient groups. 16 Patient selection for optimal outcomes is critical to ensure noninferior outcomes in the outpatient setting, specifically the elderly patient population.
Despite an overall increase in the utilization of outpatient TJA in the last decade, evidence remains limited on factors associated with non-home discharge, complications, and reoperations in Medicare eligible patients (≥ 65 years of age) undergoing outpatient THA. 17 Understanding these factors will play a crucial role in decision-making of providers to allow patients, who may require more care, to undergo a safe and expedited discharge to a facility while controlling costs associated with an unexpected destination. While numerous studies have evaluated TKA and THA in the outpatient setting broadly, few studies have focused investigations in Medicare eligible patients strictly in the outpatient setting. 17 -19 In light of the recent CMS change regarding removal of THA from the inpatient only (IPO) list, we sought to use a national surgical database to answer our primary research questions: 1) What is the frequency of non-home discharge to a facility for Medicare eligible patients (≥ 65 years of age) undergoing outpatient THA? and 2) What are the predictors for a non-home discharge in this population? As a secondary objective, we also evaluated rates and predictors of 30-day reoperation and readmission following outpatient THA in this population.
Materials and Methods
Database and Patient Selection
This study was a retrospective review of prospectively collected data from the 2015-2018 American College of Surgeons–National Surgical Quality Improvement Program (ACS-NSQIP) database. Details regarding how data are collected for the database can be found on the ACS-NSQIP website. The database was queried using Current Procedural Terminology code 27130 for Medicare eligible patients (≥ 65 years of age) undergoing outpatient Total Hip Arthroplasty. Patients <65 years of age or undergoing inpatient THA were excluded. Patients with missing data were removed from the study. The NSQIP database defines discharge destination into the following categories: 1) home; 2) skilled care facility, which was not patient’s home preoperatively; 3) unskilled care facility, which was not patient’s home preoperatively; 4) separate acute care unit; 5) rehabilitation; and 6) facility, which was patient’s home preoperatively. The variable definitions were used to group the study cohort into 1) home discharge and 2) non-home discharge to facility. Rates and risk factors associated with 30-day reoperations and readmissions were also evaluated. The data for this study was derived from a de-identified national surgical database, therefore the study was exempt from Institutional Review Board (IRB) approval.
Variables and Outcomes Studied
Patient demographic variables included as part of the study were age (dichotomized into ≤70 and >70 years), gender, race, body mass index (BMI; <25.0, 25.0-29.9, ≥30.0) and comorbidities (diabetes mellitus, history of smoking, presence of chronic obstructive pulmonary disease, congestive heart failure, hypertension, dialysis-dependent, disseminated cancer, chronic steroid use, bleeding disorder, dyspnea, and functional health status). Operative and postoperative data included American Society of Anesthesiologists (ASA) grade (dichotomized into I-II and >II), total operative time (0-80 vs. >80 minutes). All dichotomous variables were split at the median.
Statistical Analysis
Bivariate analysis using Pearson chi-squared tests were used to assess for significant associations for non-home discharge, complication, and reoperation for patients undergoing THA. All variables with a p value ≤.15 from unadjusted analysis were then entered into multivariate logistic regression models, and adjusted for each other, to identify significant independent predictors for non-home discharge and complication or reoperation. Results from multivariate regression models have been reported as adjusted odds ratios (OR) with 95% confidence intervals (CI). For all statistical purposes, a p value < .05 was considered significant. Statistical analysis was performed using SPSS v24 (IBM, Armonk, NY, USA).
Results
Baseline Clinical Characteristics
Following application of inclusion/exclusion criteria, a total of 1095 patients undergoing outpatient THA were included in the final study cohort from 2015-2018. The total number of outpatient THA procedures significantly increased over the study period
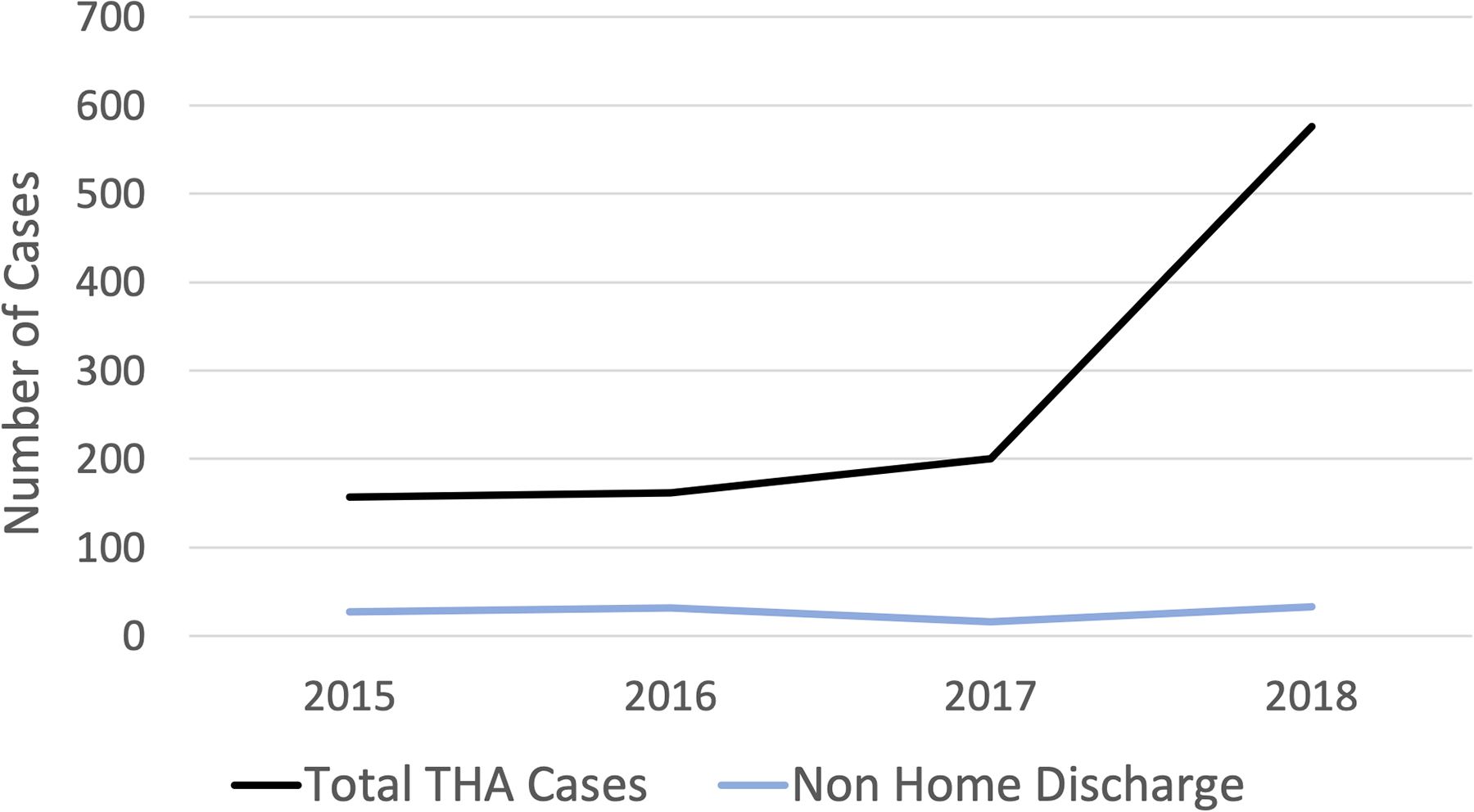
Number of outpatient THA cases and non-home discharges from 2015-2018 in patients ≥ 65 years of age. From 2015-2018, there was a significant increase in the total number of THA cases, with no significant change in the number of non-home discharges.
Patient Demographics of Medicare Eligible Patients Undergoing Outpatient THA.

Unadjusted analysis carried out using Pearson chi-squared tests.
Predictors of a Non-Home Discharge Disposition
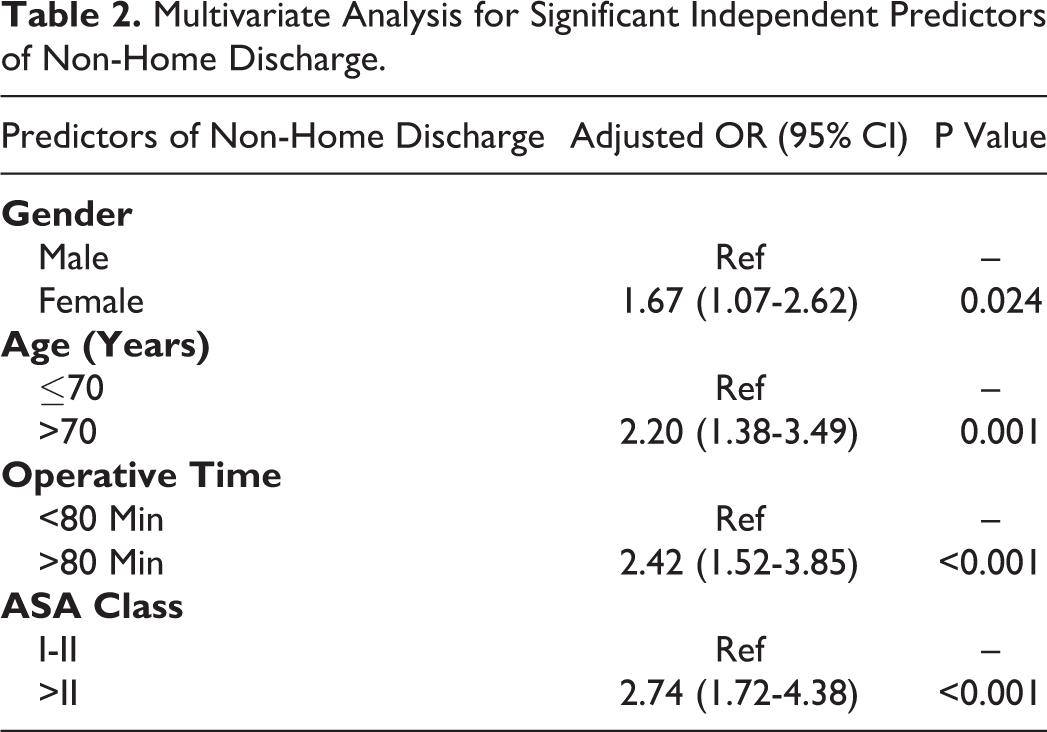
One hundred and eight (9.9%) patients were discharged to a destination other than home. Patients were discharged to rehab (n = 47; 4.3%), a skilled care facility (n = 47; 4.3%), a facility which was “home” (n = 8; 0.7%), a separate acute care facility (n = 5; 0.5%), or an unskilled facility (n = 1; 0.1%). Following adjusted analysis using a multivariate regression model, significant independent predictors for a non-home discharge disposition were, in descending order of effect, American Society of Anesthesiologists Class >II (odds ratio [OR] 2.74), operative time >80 minutes (OR 2.42), age >70 years (OR 2.20), and female gender (OR 1.67), Table 2.
Multivariate Analysis for Significant Independent Predictors of Non-Home Discharge.
Risk Factors for Readmission or Reoperation
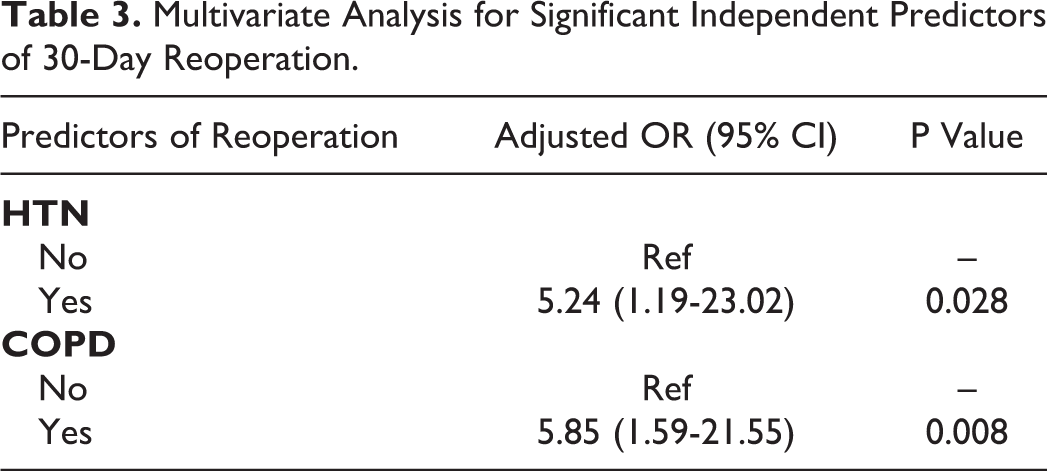
A total of 18 patients (1.6%) required an unplanned reoperation within 30 days. A total of 40 patients (3.7%) required 30-day readmissions with 35 readmissions related to the original THA procedure. Independent factors for 30-day reoperation after outpatient THA in Medicare aged patients were COPD (OR 5.85) and HTN (OR 5.24) Table 3. Independent factors for 30-day readmission after outpatient THA were HTN (OR 4.35) and Age >70 (OR 2.48) Table 4.
Multivariate Analysis for Significant Independent Predictors of 30-Day Reoperation.
Multivariate Analysis for Significant Independent Predictors of 30-Day Readmission.

Discussion
With limited literature specifically analyzing Medicare-eligible patients undergoing outpatient THA, the current study is the first to identify rates and significant predictors associated with a non-home discharge, reoperation, and readmission. Using a nationwide surgical database, we found that 10% of Medicare eligible patients undergoing outpatient THA required a non-routine discharge and were transferred to a facility. Despite the rise in THA procedures performed over the study period, there was no significant change in non-home discharges. Significant patient factors influencing discharge destination were a higher ASA class, longer operative times, increasing age, and female gender. Secondarily, 30-day unplanned reoperation and readmission rates were low (<4%) in this subset of patients.
Although previous literature on major joint replacement surgeries of hip, knee, and shoulder have explored factors associated with a non-home discharge destination broadly, 20 -22 no study has evaluated the same for Medicare-aged patients undergoing outpatient THA. Discharge destination following outpatient surgery is a relatively simple but important consideration following surgery. As the current health care system advances from volume-based to value-based payment models of care, there has been an increasing focus on identifying areas of cost-refinement in an attempt to enhance the quality of care, while curbing unnecessary health care resource utilization and associated costs. 23 It is believed that the healthiest patients are those who qualify for outpatient surgery to minimize surgical risk. However, unplanned discharge destination to a facility other than home is a financial burden to the healthcare system worth understanding in Medicare-eligible populations as more surgeries are being transitioned to an outpatient surgical setting. In our study, we found that 10% of Medicare-eligible patients undergoing outpatient THA required a nonhome discharge. Of these patients, the majority were discharged to rehab or a skilled care facility. Significant independent predictors for a non-home discharge disposition were higher American Society of Anesthesiologists Class, longer operative times, age >70 years, and female gender. The impact of increasing age and higher ASA class on influencing a non-home discharge disposition could be explained by the higher frailty and comorbidity burden present in these patients. With higher frailty levels reported to be associated with poor outcomes following total joint arthroplasty, 24 it is likely that providers are cautious about the postoperative course and may prefer having these patients undergo some degree of continued inpatient care in a facility, under surveillance. We did note that female patients were more likely to undergo a non-home discharge compared with male patients. An explanation for this effect could be lower muscle strength seen in female patients as they age, compared with male individuals, thus requiring the former to undergo more rehabilitative sessions in a facility. The prolonged operative times could be related to case complexity, which may influence a surgeon’s decision of discharging a patient to a facility to mitigate the occurrences of any avoidable adverse events. Our findings, in the context of previous studies who evaluated total joint arthroplasty of the hip and knee broadly, demonstrated similar findings of female gender and ASA grade >II influencing discharge to a facility. 20,25
The 30-day readmission and reoperation rate following outpatient THA was low (<4%) in our study, similar to complication rates reported in other studies with broader inclusion criteria. 17,19,26,27 In one large investigation by Berend et al, 1472 outpatient THAs performed at a stand-alone ASC were analyzed, and 44% of patients had 1 or more major comorbidity, with an overall complication rate of 2.2%. 2 In our study, the predictors for 30-day reoperation after outpatient THA in Medicare aged patients were COPD and HTN. Risk factors for 30-day readmission after outpatient THA were HTN and Age >70. Again, these findings in the context of previous evaluations are not entirely unexpected, 17 but with significant trends of increased operative cases being performed in the outpatient setting, this may allow for better risk stratification methods to prevent any avoidable readmission or reoperations. Larger multicenter studies are needed to provide a more robust sample size for predicting postoperative outcomes in the Medicare outpatient population.
There are a few limitations to the study. First, the ACS-NSQIP database does not contain insurance status information which has been shown to influence discharge destinations following other total joint arthroplasties. 28 In addition, the database lacks granular clinical information, such as post-operative pain and functional scores, as well as socioeconomic data, including availability of caregiver at home, which may influence the choice of discharge destination. Our readmission and reoperation evaluation was limited to 30 days postoperatively which may not capture patients who presented to the hospital after that time period. Also, for the purpose of this study, the indication for total hip arthroplasty was not considered, which may have some bearing on discharge destination. The Centers for Medicare and Medicaid Services recently removed total hip arthroplasty from the inpatient-only (IO) list in January 2020. Given this recommendation, we sought to analyze Medicare eligible patients (≥ 65 years of age) undergoing outpatient THA to understand patient risk factors for nonroutine discharge, reoperations, and readmissions. By doing so, this narrowed our inclusion criteria and the results of the study may not be applicable to younger aged cohorts or those undergoing surgery in the inpatient setting.
Conclusion
Using a select cohort of more than 1000 THAs from a national surgical database, the study is the first to analyze a specific inclusion criteria of patients undergoing outpatient THA. With limited literature specifically analyzing Medicare-aged patients undergoing THA in the outpatient setting, the current study identifies rates and significant predictors associated with a non-home discharge, reoperation, and readmission. Providers should consider preoperatively risk-stratifying these patients to reduce the costs associated with unplanned discharge destination, complication or reoperation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Committee Statement
This study did not require approval from the Institutional Review Board of The Ohio State University.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.