
Abstract
Introduction:
As the US population ages, the need for total hip arthroplasty (THA) is predicted to increase by 174% by 2030. The purpose of our study was to examine the rate and risks of 30-day complications and unplanned readmission in patients over the age of 80 years old.
Materials and Methods:
The National Surgical Quality Improvement Project database for the years 2008 to 2014 was queried for patients over the age of 80 undergoing THA. The risks of major complications, minor complications, bleeding occurrences, unplanned readmissions, and deaths over a 30-day period were examined using univariate and multivariate analyses.
Results:
A total of 7730 patients were included for analysis; 324 (4.2%) patients experienced a major complication, 1944 (25.1%) patients experienced a minor complication, 1776 (22.9%) patients had a bleeding occurrence requiring transfusion, and 376 (4.9%) patients experienced an unplanned readmission to the hospital within 30 days. A total of 33 (0.4%) patient deaths were recorded within 30 days postoperatively. Patients with congestive heart failure were at increased risk for developing a major complication, odds ratio (OR) 3.618 (1.052-12.437), and postoperative death, OR 11.920 (1.362-104.322). Patients with an American Society of Anesthesiologists >2, OR: 1.351 (1.131-1.613), and an operative time greater than 120 minutes, OR: 1.346 (1.084-1.670), had increased risks of minor complications. Patients with a body mass index greater than 30 had reduced rates of minor complications, OR: 0.609 (0.486-0.763). Increased risk of unplanned readmission was seen in patients with chronic obstructive pulmonary disease, OR: 2.403 (1.324-4.359).
Discussion/Conclusion:
Elderly patients undergoing THA have high complication and readmission rates. Surgeons should convey these increased risk factors and rates of complications in elective THAs to their elderly patients and work with primary care physicians to mitigate these risks.
Introduction
Osteoarthritis encompasses the majority of disability in the elderly population. Over the past 2 decades, the United States has seen a rapid expansion in the octogenarian and nonagenarian population, which has altered the demographic profile of the baby boomer generation into an even older cohort. 1 The demand for joint replacement will rise with the aging population as arthritis is a degenerative condition most commonly affecting the elderly population. As this elderly population continues to live longer, they have and will continue to see an increased demand for total hip replacements as well as revision hip replacements. It has been estimated that the demand for total hip arthroplasty (THA) will increase by 174% by the year 2030, and revision THA will double by 2026. 2
Overall, as people age, they tend to acquire more medical comorbidities, take more medications, and present with higher risk for surgical procedures, which can predispose them to higher incidence of postoperative complications. 3 Certain conditions that may predispose patients to readmission include chronic obstructive pulmonary disease (COPD), congestive heart failure (CHF), and American Society of Anesthesiologists (ASA) classification of >2. 4 However, there remains strong evidence to support pursuing operative intervention over conservative management as an effective treatment option for these patients. 5,6 Thus, it is imperative to appropriately screen these elderly patients for factors that may predict whether they will incur a postoperative complication for an elective procedure.
The primary purpose of our study was to examine the rate and risks of 30-day complications and unplanned readmission in patients over the age of 80 years old undergoing primary THA. We hypothesize an overall higher complication rate in octogenarians and nonagenarians when compared to younger sections of the population undergoing total hip replacement secondary to the increasing comorbidities associated with aging. The secondary purpose of this study was to (1) differentiate complications as major or minor, (2) determine which complications occur most often in this age group, and (3) identify any predisposing comorbidities or protective factors effecting outcomes after THA among this cohort.
Materials and Methods
A retrospective review of the American College of Surgeons National Surgical Quality Improvement Project (NSQIP) database for the years 2008 to 2014 was performed for this study. The NSQIP is comprised of data collected from multiple hospitals across the United States. The NSQIP database has been utilized for numerous orthopedic studies and has proven to be highly reliable with an interobserver disagreement of only 1.6%. 4 Data collected and included for analysis include demographic data, medical comorbidities, procedures performed, functional status, complications, readmissions, and mortality over the initial 30-day postoperative period.
Inclusion and Exclusion Criteria
Patients were included for analysis in this study if they were over the age of 80 years old and had a THA as determined by the Current Procedural Terminology code 27447. Patients who underwent a THA for conditions such as acute trauma, infection, or malignancy as identified by International Classification of Diseases, Ninth Revision (ICD-9) codes were excluded.
Outcome data of interest for this study were analyzed including mortality, major complications, minor complications, bleeding occurrences, and unplanned readmission. A major complication was defined by the authors as deep wound infection, wound dehiscence, cerebral vascular accident, pulmonary embolism, failure to wean intubation, unplanned reintubation, cardiac arrest, myocardial infarction, sepsis, and unplanned reoperation. A minor complication was defined by the authors as superficial wound infection, acute renal failure, deep venous thrombosis, peripheral neurological deficit, bleeding occurrence(s) requiring transfusion, and pneumonia.
Multivariate logistic regression models were utilized to determine and analyze factors that placed patients at risk of developing these adverse outcomes over the initial 30 postoperative days. The elderly patient cohort was divided into patients ages 80-84 years old and 85 years and older. The patient cohort was stratified with demographic data including gender, race, and ethnicity. Variables analyzed using multivariate logistic regression models resulting in odds ratios (ORs) included admission source, body mass index (BMI), functional status prior to surgery, history of COPD, history of CHF, and type of anesthesia. Operative variables included operative time and ASA classification.
Results
A total of 7730 patients over the age of 80 years undergoing THA between 2008 and 2014 were identified and included for analysis. Demographic data are presented in Table 1. Complications reported in patients over the age of 80 undergoing THA were analyzed. There were 324 (4.2%) patients with reported major complications. There were 1944 (25.1%) patients with reported minor complications. There were 1776 (22.9%) patients with reported bleeding occurrences. There were 376 (4.9%) patients with reported incidents of unplanned readmissions. There were 33 (0.4%) reported patient deaths. The overall complication and mortality data are presented in Table 2.
Patient Demographics.

Complications and Mortality

Multivariate logistic regression models were used to determine risk factors and ORs for patients over the age of 80 undergoing primary THAs. A history of CHF was a risk factor for a major complication (OR: 3.618 [95% confidence interval, CI [1.052-12.437]).
For minor complications, patients over the age of 85 were at higher risk of experiencing a minor complication (OR: 1.396 [95% CI: 1.177-1.655]). Male patients were at a lower risk than female patients (OR: 0.720 [95% CI: 0.601-0.863]). Patients with a BMI of 25 to 29 and patients with a BMI greater than 30 were at lower risk compared to patients with a normal BMI (OR: 0.768 [95% CI: 0.634-0.931]) and (OR: 0.609 [95% CI: 0.486-0.763]), respectively. Operative time >120 minutes increased the risk of experiencing a minor complication (OR: 1.346 [95% CI: 1.084-1.670]). Patients with an ASA classification greater than 2 were at increased risk for minor complications (OR: 1.351 [95% CI: 1.131-1.613]). The breakdown of minor complications is presented in Table 3.
Odds of Minor Complications.
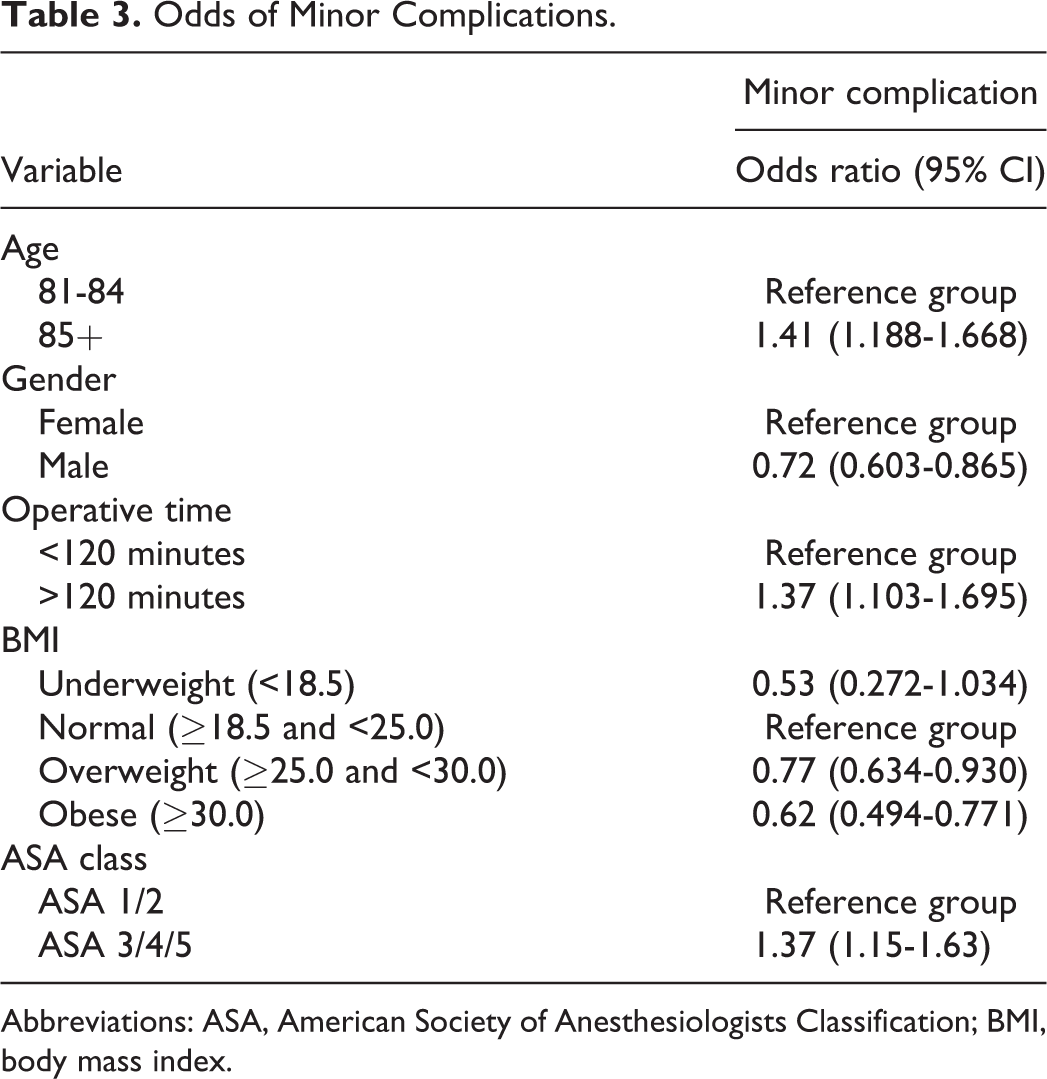
Abbreviations: ASA, American Society of Anesthesiologists Classification; BMI, body mass index.
Patients age 85 and above were at an increased risk of bleeding occurrences requiring transfusion (OR: 1.380 [95% CI: 1.162-1.638]). Male patients had a reduced risk of bleeding occurrences requiring transfusion (OR: 0.707 [95% CI: 0.588-0.848]). Overweight patients (BMI: 25-29.9) and obese patients (BMI > 30) had lower rates of bleeding occurrences requiring transfusion (OR: 0.711 [95% CI: 0.587-0.862], OR: 0.544 [95% CI: 0.433-0.683]), respectively. Operative time >120 minutes had higher rates of bleeding occurrences requiring transfusion (OR: 1.532 [95% CI: 1.235-1.900]). Patients with an ASA classification greater than 2 were at increased risk of experiencing a bleeding occurrence requiring transfusion (OR: 1.532 [95% CI: 1.235-1.900]). The breakdown of bleeding occurrences is presented in Table 4.
Odds of Bleeding Occurrence.

Abbreviations: ASA, American Society of Anesthesiologists Classification; BMI, body mass index.
Patients with a history of chronic pulmonary obstructive disease (COPD) were at an increased risk for unplanned readmission (OR: 2.403 [95% CI: 1.324-4.359]). Patients with an ASA group over 2 trended toward an increased risk for unplanned readmission but did not reach significance (OR: 1.284 [95% CI: 0.839-1.967]). Patients with a history of CHF were at increased risk of postoperative mortality (OR: 11.920 [95% CI: 1.362-104.322]).
Discussion
Chronic obstructive pulmonary disease was the only comorbidity that increased the risk for readmission within 30 days. This is in concordance with previous studies’ findings. Liao and Lu compared postoperative complications following THA in patients with and without COPD from the National Health Insurance Research Database. Chronic pulmonary obstructive disease was an independent risk factor for readmission, most commonly for pneumonia, as well as acute respiratory distress and postoperative mortality. This risk increases in patients who suffered from additional comorbidities, namely CKD. 7 In addition to preoperative medical optimization of these patients, an emphasis should be placed on postoperative chest care with frequent reinforcement to decrease the risk of postoperative pneumonia.
Congestive heart failure was the only comorbidity that increased the risk of major complication following THA. Patients with a history of CHF were also at an increased risk of postoperative mortality. Courtney et al evaluated risk factors for major medical complications following primary total joint arthroplasty (TJA), demonstrating that CHF (OR = 9.27) was an independent risk factor for in-hospital complications and postoperative mortality. 8 These patients should be identified as high risk during preoperative medical assessment, and surgical intervention must be considered only if benefits outweigh risks.
Our review of the NSQIP database showed that patients aged 85 years and older were at increased risk of minor complications and bleeding occurrences requiring transfusion compared to those ages 80 to 84 years. This is consistent with previous studies that have demonstrated a higher rate of complications in octogenarians, as well as a “snowballing” effect of multiple complications, leading to extended length of hospital stay postoperatively. 6
Male patients were at reduced risk of experiencing a minor complication or bleeding occurrence in the present study. This association has been demonstrated in prior studies. Frisch et al found that female patients were more than twice as likely (OR= 2.60) to require postoperative blood transfusion following total knee arthroplasty (TKA) or THA, 9.27% and 26.6%, respectively. 4 The same study also indicated the association between hemoglobin, increased age, operation time, and estimated blood loss (EBL) with need for transfusion. Considering female tendency for lower baseline hemoglobin and the increased operating time in THA compared to TKA, surgeons should consider intraoperative methods of decreasing blood loss such as use of tranexamic acid (TXA) and attention to meticulous hemostasis. 9
Patients who were overweight (BMI: 25-25.9) and obese (BMI > 30) had reduced risks of bleeding occurrences requiring a transfusion compared to the normal BMI cohort. This is contrary to a prior retrospective study (mean sample age = 66.2), which demonstrated an association between increased BMI (mean BMI = 31.9) and increased risk of requiring blood transfusion postoperatively. 4 Within the population assessed in our study, it is important to consider malnutrition, which may present in up to 38% of elderly inpatients. 10 In addition to addressing nutritional deficiencies preoperatively, the NSQIP/American Geriatrics Society Best Practice Guidelines recommend that older adults undergo daily nutritional evaluations postoperatively, including dysphagia evaluation and aspiration precautions. 10
Operating times longer than 120 minutes and ASA score >2 were both independently associated with increased risk of minor complications and bleeding occurrences. Prolonged operating time has known increased risks, such as an association with increased EBL. 4 The ASA grade has been validated as a useful predictor of perioperative health status in THA, specifically in-hospital postoperative complication and mortality in patients with ASA score >3 in prior studies. 11 However, in a more recent prospective study whose outcomes lacked any incidence of mortality, ASA was not a predictor of in-hospital postoperative complications. 12 Nonetheless, in the setting of hip arthroplasty in the elderly population, ASA grade serves as a valuable reminder of those patients who require particular attentiveness and high index of suspicion for potential postoperative decline.
Our study had several strengths. We were able to perform a powerful and comprehensive analysis in our study given the large patient sample (n > 7730) of patients over 80 years of age undergoing elective THA. Prior studies have used patients under 80 years of age as a comparison group. Our study in unique in that it focuses solely on the octogenarian population. Additionally, the NSQIP database has a high reliability, with only 1.6% interobserver disagreement. 13 The NSQIP database allows for in-depth analysis of various conditions and outcomes related to the elderly population undergoing elective THA due to the wide variety of patient outcomes and risk factors it provides.
The primary limitation to our study is that the NSQIP database is a retrospective review of patients undergoing elective THA. The NSQIP relies on voluntary input of data from hospital records as opposed to relying on insurance claims. We recognize that large data sets such as these are subject to compromising quality of data for volume. The quality of data used in our review would have been strengthened if it was sourced from a data set with less potential for human error. Future research contrasting results of the same analysis when performed on a voluntary database compared to insurance claims may reveal the reliability of such studies. Additionally, the NSQIP database lacks details that would have benefited the discussion of results in our study. For example, information on patient’s thromboembolic prophylaxis would have allowed for a further investigation contributing to increased risk of bleeding in this population. Furthermore, the NSQIP database only captures adverse outcomes and readmissions over the initial postoperative 30 days. We recognize that the adverse outcomes or readmission rates after the initial postoperative 30 days, though not captured in our study, are certainly abundant and should be examined in a future study.
Conclusion
As the US population ages, the need for THA is predicted to increase by 174% by 2030. 2 Studies have projected that the total percentage of the population over 80 years of age will nearly double by 2050. 1 It is the role of orthopedists to assist in facilitating the best functional outcome for patients who have maintained high activity levels later in life. Conservative management may be suboptimal in many of these patients. It is our goal to initiate preparedness in managing an increase in demand for surgical intervention in a population with inherently higher rates of comorbidities.
Our study provides surgeons and other treating staff with information regarding increased risk for complications secondary to type of anesthesia implemented, postoperative anticoagulation, healing potential, length of hospital stay, postoperative recovery and rehabilitation, and potential for readmission. With this information, the treating surgeon can risk stratify his or her patients and provide the patient with the proper expectations that will shape their decision-making process. We emphasize the importance of preoperative optimization and multidisciplinary management for elective arthroplasty for octogenarians. Future studies focusing on rehabilitation, functional outcomes, and overall cost have the potential to effect health care policy and financial planning.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.