
Abstract
Objective
Spinal osteochondromas are rare, and approximately less than 5% occur as spinal lesions. We report the case of a solitary osteochondroma of the spine and review and update the literature on spinal osteochondroma, including surgical treatment and subsequent results.
Case Description
A 73-year-old female patient complained of a 10-year history of back pain and a 4-year history of right-side lower extremity radiating pain with paresthesia. Computed tomography and magnetic resonance imaging (MRI) revealed a bony mass arising from the inferior articular process (IAP) of L3, presenting with features of compressive spinal stenosis at the L3–L4 level. The treatment strategy included the complete marginal excision of the lesion through the posterior approach, as well as complete decompression of the spinal canal and nerve roots. The patient’s symptoms resolved after surgery, and histopathological examination identified the lesion as an osteochondroma.
Review Results
This review study included 168 solitary osteochondroma cases. The most commonly involved spinal level was cervical (51.8%), and the most frequent spinal anatomic column involved was the posterior column (70.8%). Radiculopathy accounted for 30.3% of all cases, myelopathy accounted for 31.0%, and 7.7% exhibited both symptoms simultaneously. The recurrence rate was 6.0%.
Conclusion
Computed tomography and MRI can effectively diagnose spinal osteochondroma, and surgical treatment can effectively improve clinical outcomes. In almost all symptomatic cases, the best treatment is marginal excision of the tumor. Complete resection of the cartilaginous cap of the tumor is especially important to prevent recurrence.
Introduction
Among benign bone tumors, osteochondromas are a relatively common one. Osteochondroma is also known as osteochondrogenic exostosis or exostosis, which can be solitary or multiple. 1 Osteochondromas usually occur in the long bones in the appendicular skeleton, which involve the metaphyseal or diametaphyseal region. 2 Spinal osteochondromas are rare, and approximately less than 5% occur as spinal lesions. 3 They are usually asymptomatic; however, symptomatic myelopathy, progressive radiating pain, or both, if not diagnosed and treated early, may lead to serious neurological sequelae because it poses a threat to the spinal cord and surrounding vital structures.4,5
Here, we report a case of a solitary lumbar osteochondroma with neurological symptoms and conduct a review of the literature on the subject from 2004.
Case Report
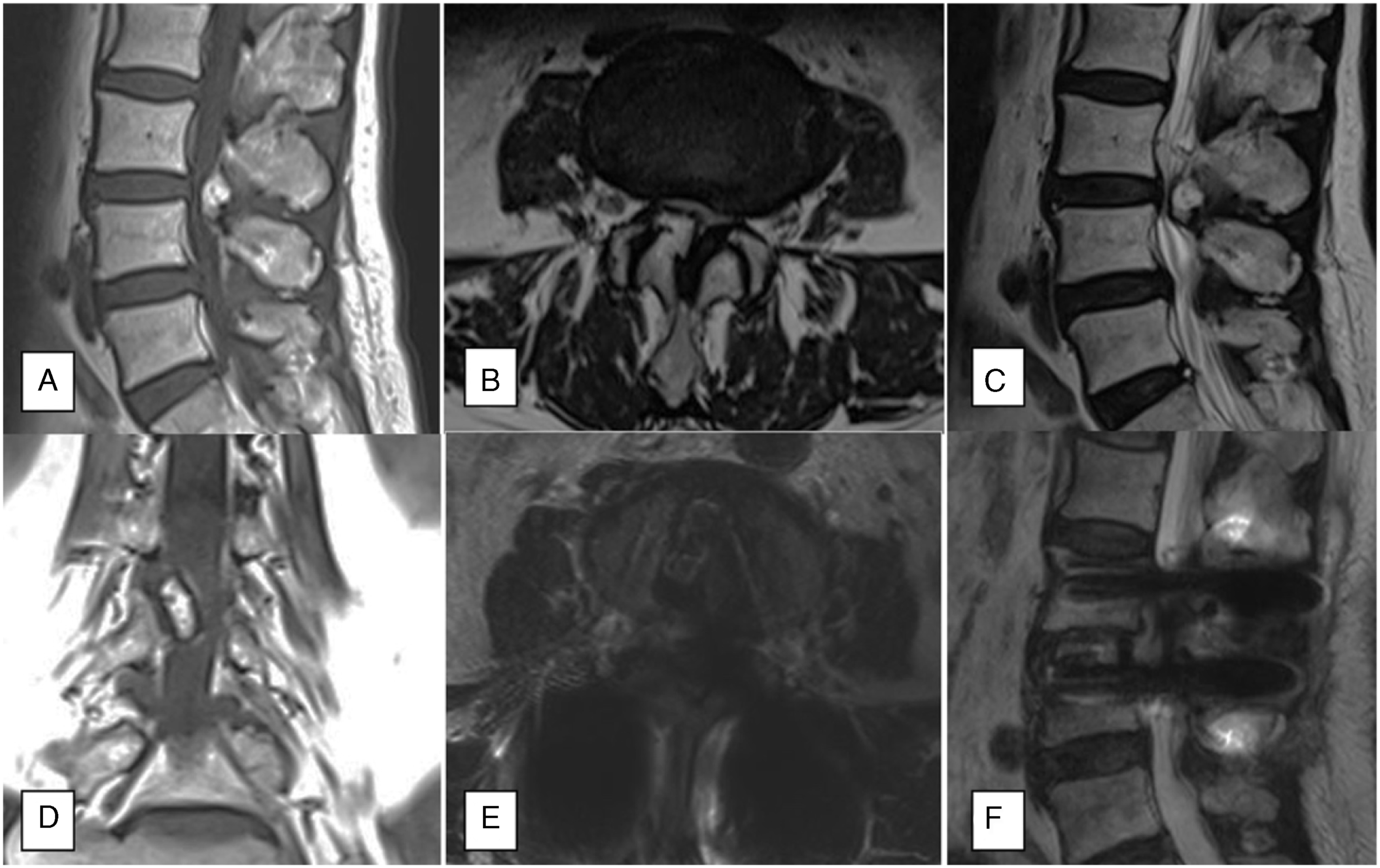
A 73-year-old female presented with a 10-year history of back pain and a 4-year history of right-side lower extremity radiating pain with paresthesia. Neurological intermittent claudication was 100 m, but no abnormalities in urination and defecation were observed. The patient had no prior history of bone masses or other tumors. Computed tomography and magnetic resonance imaging (MRI) showed an abnormal bony mass arising from the right-side inferior articular process (IAP) of L3 that projected into the spinal canal, resulting in marked spinal canal stenosis (Figures 1 and 2). Preoperative CT images. An abnormal bony mass arising from the right-side inferior articular process of L3 that projected into the spinal canal, resulting in marked spinal canal stenosis. A-D, preoperative MRI images; E and F, postoperative MRI.
A posterior median incision centered on L3 was made, the skin and subcutaneous tissue were incised, and the sacral spinal muscles on both sides were bluntly stripped to expose the L3 and L4 spinous processes and both sides of the lamina. The pedicle screws were inserted at the L3 and L4 pedicles. Then, the right portion of the lamina and IAP were removed to visualize the IAP and the 1.5 cm × 1.5 cm bony protrusion in front of the lamina (Figure 3). The protrusion was covered with white cartilage, and the ligamentum flavum, which was hypertrophic, was removed. A check for active bleeding was subsequently performed. The incision was closed layer by layer, and a drainage tube was placed. Finally, the wound was covered with a sterile dressing. Overall architecture of the lesion.
Histopathological examination of the resected tissue revealed a bony lesion with a three-layer structure with clear boundaries: a thickened fibrous capsule on the surface, a hyperplastic cartilage tissue in the middle layer, chondrified bone tissue and cancellous bone in the inner layer, and calcification in some areas; the above descriptions typical of an osteochondroma (Figure 4). Histopathological examination.
No adverse events were encountered peri- and postoperatively. The patient demonstrated immediate relief from back pain and right leg radiating pain. On postoperative day 3, an MRI scan showed no residual tumor and no compression of the spinal canal (Figure 2E and F).
Discussion
To search for relevant articles on solitary osteochondromas and spinal lesions, we conducted a comprehensive literature search on the database, including PubMed, Embase, and Cochrane Library for papers published from 2004 to August 2020. English language filters were applied, and standard searches were performed with the keywords: “osteochondroma” AND “spinal.” Titles and abstracts from all the reports identified were examined independently by 2 reviewers (G.X.L. and H.J.W.), and the full texts of suitable studies were retrieved. In addition, the reference lists of the selected articles and previous similar meta-analyses on solitary spinal osteochondromas were manually researched. In cases where disagreements could not be resolved, in-depth discussions were conducted, and ultimately decided upon by the senior author. The exclusion criteria were literature reviews, cases of other osteochondromas, and reports without details of the cases.
On reviewing the literature, a total of 207 articles were published from 2004 to August 2020, of which 92 articles4-95 (168 cases) met the inclusion criteria (Figure 5). The demographic data are shown in Table 1. The review included 100 male patients and 68 female patients. The mean age was 35.3 years (range from 2 to 83 years). The most frequent spinal level involved was cervical in 86 (51.8%) of the cases, followed by lumbar with 42 (25.0%), thoracic with 34 (20.2%), sacral with 14 (8.3%), and coccyx with 2 (1.2%). Among the 168 cases, 11 cases involved the vertebral junction, 5 involved the cervicothoracic junction, 2 the thoracolumbar, and 4 the lumbosacral. The most common spinal anatomic column involved was the posterior column with 119 cases (70.8%), followed by the anterior column with 22 (13.1%). In 16.1% of cases, the spinal anatomic column was not reported. Radiculopathy accounted for 30.3% of cases and myelopathy for 31.0%. In 7.7% of cases, both symptoms occurred simultaneously. Only 10 (6.0%) cases had recurrence after surgery. All 168 cases of solitary spinal osteochondromas are listed in Table 2. Among them, a total of 145 patients underwent surgery, and the clinical symptoms of 123 patients were improved. Two cases presented with worsening symptoms after surgery. A flow chart of the review study. Demographic Data of Spinal Solitary Osteochondroma of the 168 Cases. Reviewed Cases in Literature.


Many studies have been published since the first case of solitary osteochondroma was reported by Reid in 1843, 96 with an increase seen in recent years. Two literature reviews on spinal osteochondroma have been published: included 96 cases (1843–1992) 3 and 54 cases (1992–2003). 93 In present study, 168 new cases were updated from 2004 to 2020.
Osteochondromas are derived from the anterior cartilage and connective tissue. Most researchers believe that osteochondromas are hamartomas that occur in the metaphysis of long bones. Osteochondromas are divided into single and multiple forms. The latter is often referred to as osteochondromatosis or multiple exophytic chondroma, among other terms, and most of which are inherited in an autosomal dominant manner. Spinal osteochondromas are relatively rare, with an incidence rate of 1%–4%.9,12,16 Among these, those with neurological symptoms account for .5%–1%.19,20 Of spinal osteochondromas, nearly half of the patients occur in the cervical spine (C2>C3>C6).8,13,19 The second most common occurrence of spinal osteochondromas is thoracic lesions.14,17 Osteochondroma can occur during development due to abnormal development of the epiphyseal plate or frequent minor trauma. The high incidence of cervical osteochondroma is related to its high mobility and greater susceptibility to microtrauma of the epiphyseal plate of the vertebral body. In addition, secondary ossification centers with rapid growth and development have a greater chance of cartilage malformation, and thus of osteochondroma. The secondary ossification centers of the cervical spine ossify in adolescence, faster than the thoracic spine, and the lumbar spine ossifies the latest. Although the mobility of the lumbar spine is greater than that of the thoracic spine, but the ossification is later, so the incidence is lower. Spinal osteochondromas tend to occur in the appendages of the vertebral body, especially in the parts directly attached to the nerves or spinal cord. This tendency may be related to the appearance of secondary ossification centers of the spine during adolescence.
The etiology of osteochondromas is still unclear, and it may be related to the loss of the autosomal dominant tumor suppressor gene EXT-1 or EXT-2, excessive growth of cartilage tissue in the secondary ossification center, minor trauma, or X-ray irradiation.51,58 Several papers reported that bone hyperplasia is also related to the pathogenesis of osteochondromas.61,65 Furthermore, bone transformation may trigger out-of-control cell differentiation, leading to the occurrence of osteomalacia.69,76
In most patients, the cartilage cap and subcapsular fluid on the surface of the tumor are caused by excessive activity, trauma, strain, and other factors, and the tissues surrounding the tumor are edematous, causing compression symptoms.81,84 Spinal osteochondromas can have a variety of clinical manifestations depending on the tumor location, growth rate, and degree of compression. The most common symptoms of spinal osteochondromas are radiating pain, dyskinesias, sensory disturbances, and urinary incontinence. Patients’ subjective symptoms generally gradually worsen but rarely cause acute attacks.
Diagnosis is mainly based on the selection of appropriate imaging examinations based on the patient’s symptoms. Due to the complex anatomical structure of the location of the spinal osteochondroma and the overlap, the diagnosis rate of routine X-ray is low and is thus only used as a screening reference. CT and MRI examinations, on the other hand, are pivotal in determining the nature of the disease, the location and extent of tumoral invasion of the spinal canal, and compression of the spinal cord and nerve roots. Typical osteochondroma lesions are shown on CT as cortical and cancellous bones connected to normal bone at the base. On CT, osteochondromas appear as expansive cauliflower-like bony masses with clear and irregular borders, visible cartilage caps, formation of internal calcification foci, and uneven bone crests and separation shadows. MRI may show different signal characteristics because the size of the lesion and the degree of cartilage calcification are related to signal intensity.49,86 The cartilage cap exhibits different signals depending on the degree of calcification. If the cartilage cap is highly calcified, it will show a low signal on T1- and T2-weighted imaging. Conversely, if the cartilage cap is less calcified, it will show a high signal on T2WI or STIR image and a low to medium signal on T1WI. Thus, MRI is suitable for assessing the impact of tumors on surrounding tissues, such as the spinal cord and nerves. After enhancement, the fibrovascular tissues around, and between the cartilage will be strengthened. MRI can be considered the most accurate method for measuring cartilage cap thickness.
Although osteochondromas of the spine are benign tumors, they have a specific site of growth. The authors concluded that small, single osteochondromas growing outside the spinal canal are unnecessary to remove in the absence of clinical symptoms. However, larger osteochondromas or any osteochondroma that affects the spinal canal should be treated surgically to avoid causing or worsening spinal cord and nerve damage, especially when complete resection is complicated and difficult due to tumor enlargement. The tumor should be removed as much as possible during surgery because incomplete removal of the tumor body or cartilage cap can lead to tumor recurrence. The recurrence rate after resection is low, and the histological manifestations of recurring tumors are benign cartilage lesions and low-grade chondrosarcomas.10,34 However, considering that not all studies clearly report this parameter, many recurrences may not be reported.
The most serious complication of osteochondromas is malignant transformation. The typical malignant transformation usually occurs after bone maturation and rarely occurs before the age of 20. The prognosis of spinal osteochondromas is generally good and is related to the degree and location of preoperative nerve damage. A better understanding of tumor biology and the development of advanced imaging and surgical techniques have made the treatment in recent years more convenient and effective.
Conclusion
Surgical treatment of a rare, lumbar osteochondroma has achieved good clinical results through posterior decompression and fusion surgery to alleviate radiating pain with paresthesia. Our literature review found that spinal osteochondromas mostly occurred on the cervical spine and often involved the posterior spine column. Solitary spinal lesions have caused neurologic symptoms, such as radiculopathy and myelopathy. The ideal treatment in almost all symptomatic cases is marginal excision of the tumor. Complete resection of the tumor cartilaginous cap is especially important to prevent recurrence and negative clinical outcomes.
Footnotes
Author Contributions
Writing—original draft: Guang-Xun Lin
Investigation and Software: Hua-Jian Wu
Project administration: Chien-Min Chen
Supervision: Gang Rui
Writing—review and editing: Bao-Shan Hu.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This retrospective study was approved by the institutional Ethics Committee of the First Affiliated Hospital of Xiamen University. Informed consent was waivered due to the retrospective and non-interventional nature of this analysis.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Natural Science Foundation of Fujian Province, grant number 2021J05282, funded by the “Xiamen Health System Discipline Leaders and their Backup Candidates, Senior Management Talent Training Candidates Training Program.”