
Abstract
Introduction
In this study, our aim was to examine the relationship between the arthroplasty surgeons’ experience level and their aptitude to adjust the cable tension to the value recommended by the manufacturer when asked to provide fixation with cables in artificial bones that underwent extended trochanteric osteotomy (ETO).
Materials and Methods
A custom-made cable tensioning device with a microvoltmeter was used to measure the tension values in Newtons (N). An ETO was performed on 4 artificial femur bones. Surgeons at various levels of experience attending the IXth National Arthroplasty Congress were asked to fix the osteotomized fragment using 1.7-mm cables and the tensioning device. The participants’ demographic and experience data were investigated and recorded. The surgeons with different level of experience repeated the tensioning test 3 times and the average of these measurements were recorded.
Results
In 19 (35.2%) of the 54 participants, the force applied to the cable was found to be greater than the 490.33 N (50 kg) value recommended by the manufacturer. No statistically significant difference was determined between the surgeon’s years of experience, the number of cases, and the number of cables used and the tension applied over the recommended maximum value (P = .475, P = .312, and P = .691, respectively).
Conclusions
No significant relationship was found between the arthroplasty surgeon’s level of experience and the adjustment of the cable with the correct tension level. For this reason, we believe that the use of tensioning devices with calibrated tension gauges by orthopedic surgeons would help in reducing the number of complications that may occur due to the cable.
Introduction
Removing a well-fixed femoral component is a time-consuming task in revision total hip arthroplasty (rTHA) and is open to complications. 1 Therefore, extended trochanteric osteotomy (ETO) is one of the most preferred methods for providing greater exposure to the femoral stem and the acetabulum during complex rTHA surgeries. 2 Although a gold standard method still has not been reported for the fixation method after ETO, several techniques including the use of cerclage wires, cables, and combination of plate and cables have been described.3,4 Of them, while plate and cable combinations have been recounted to allow less migration and offer better stability than the horizontal cerclage wire and cable methods; studies reporting bursitis, pain, and abductor failure due to the combined use of plates and cables also exist.1,2,4-6 On the other hand, some studies reported that successful clinical and radiological results have been obtained with isolated cable fixations which require less soft tissue dissection and aim at minimizing the blood supply in the osteotomized fragment.1,2,7
Although some researchers suggested that there is a decreased risk of bursitis with fixation through the use of cables after ETO, and that the circulation of the bone fragment is less affected with less soft tissue dissection, complications with the use of cables were also reported.1,6,8 Abdel et al. 1 noted that the most common intraoperative and postoperative complication was fracture in the osteotomized fragment in the study where they used the ETO method during surgery and reported the results of the patients who underwent fixation using cables. While the authors had reported that the most important etiological factor in postoperative fractures was the increase in stress concentration around the cable, they also recounted that overtightening of the cable should be avoided in order to prevent this complication. In another study conducted with artificial bone models, it was reported that less tightening of the cables during fixation after ETO would cause instability in the greater trochanter, while overtightening may lead to fractures in the cable or the bone. 6 In order to avoid these complications, manufacturers have introduced a tensioning device with a calibrated tension gauge. 9 However, many of the cables currently available in the market do not have calibrated tension gauges in their tensioning devices, and manufacturers recommend adjusting the tension in line with the surgeon’s experience. 10
Our aim in this study was to examine the relationship between the surgeons’ experience level and their aptitude to adjust the cable tension to the value recommended by the manufacturer using cables and tensioning devices without calibrated tension gauges, when they were asked to provide fixation with cables in artificial bones that underwent ETO. We hypothesized that the surgeon’s experience and the application of the recommended cable tension value were not associated. Upon a review of the literature, we could not find any study conducted in line with this purpose and hypothesis.
Materials and Methods
Preparation of the Custom-Made Cable Tensioning Device
Two T-handle cable tensioning devices (Dall-Miles
Participants and Cable Installing
In our study, 4 synthetic femoral bone models (Synbone®) with proven reliability of their mechanical properties were used.11,12 All bone models were performed ETO using a 13-cm-long oscillating saw (Colibri II; DePuy Synthes, Raynham, MA, USA).
1
The model bones were fixed stably on the table in the anatomical position with the help of bench vise. Our study was carried out during the IXth National Arthroplasty Congress held annually in our country and included arthroplasty surgeons with different experience levels. The participants’ ages, characteristics of the center they work at (university-teaching hospital, state hospital, private practice), years of surgical experience, the number of revision hip arthroplasty surgeries performed per year, their trochanteric reattachment choice (cable, cerclage wire, trochanteric grip + cable, trochanteric grip long plate + cable), and the number of cables used per year were investigated and recorded. All participants were asked to fix the fragment obtained with ETO at 1 cm distal of the lesser trochanter on the model femur bone using one 1.7-mm cobalt-chrome cable (DePuy Synthes) with the help of a custom-made cable tensioning device (Figure 1). The maximum tension value of the cable recommended by the manufacturer was 50 kg (490.33 N). The tension values were recorded when the participants blindly stated that they achieved sufficient tension in the cables, in line with their own experiences. All participants repeated the same test 3 times and the average of the 3 measurements were recorded. The custom-made cable tensioning device with a microvoltmeter (Fludex®) which measures cable tension force values in Newtons (N) during the fixation of extended trochanteric osteotomy–performed fragment to synthetic femurs (Synbone® 2162).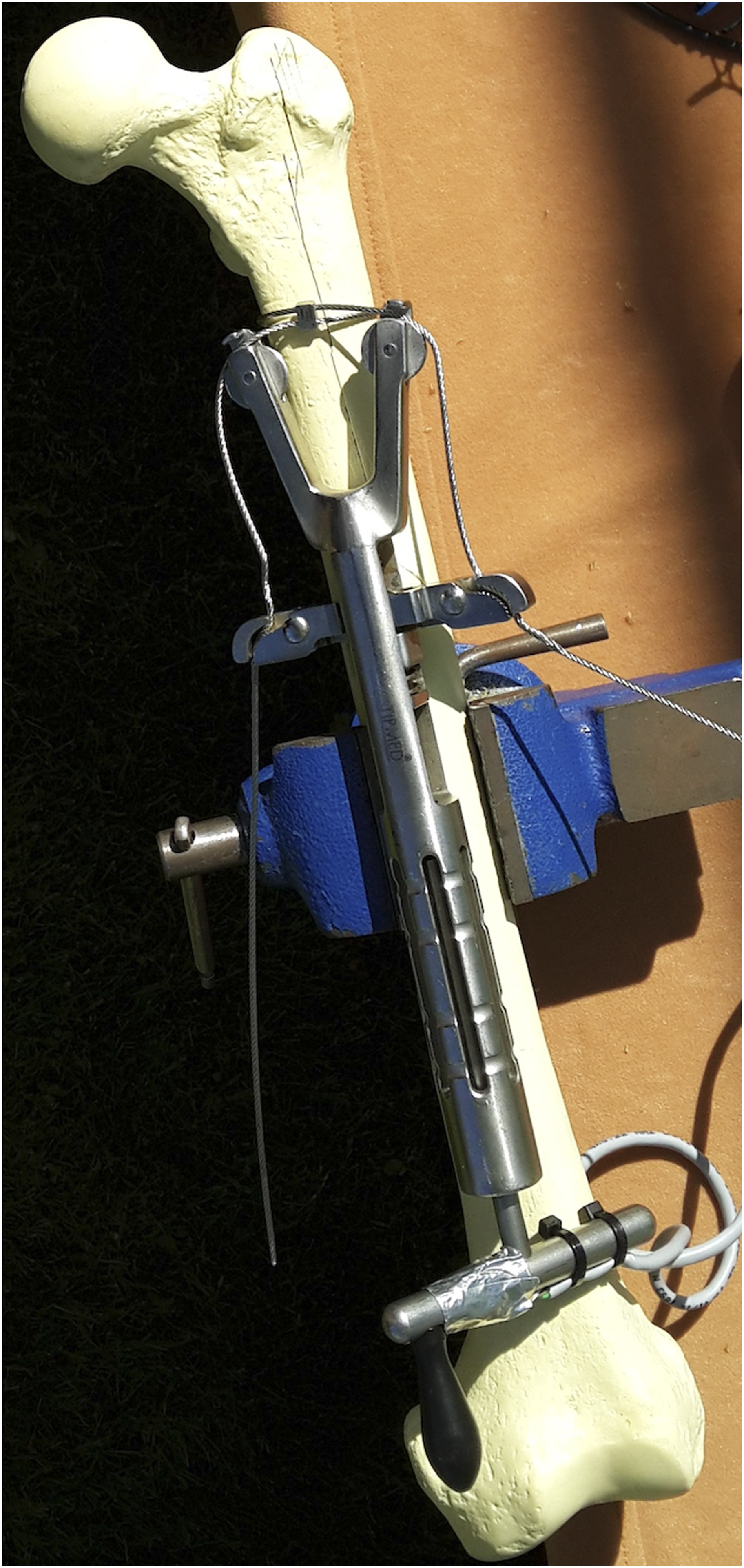
Testing and Data Processing
The system was set up at room temperature (20°C) about 20 minutes before the tensioning activity to allow for the optimal heating point for correct results to be obtained on the microvoltmeter. Before tensioning of the cables, the starting point of the microvoltmeter was noted. The participants applied tension to the cable until optimal tension was felt.
Statistical Analysis
Data obtained in the study were analyzed statistically using the SPSS v.19.0 software. Descriptive statistics were stated as median, minimum, and maximum values for the continuous variables and as number (n) and percentage (%) for the categorical variables. Conformity of the continuous variables to normal distribution was evaluated with the Shapiro–Wilk test. In the comparison of the 3 groups of variables not showing normal distribution, the Kruskal–Wallis test was applied. For subgroup comparisons, the Bonferroni-corrected Mann–Whitney U test was used. Pearson’s chi-square test was performed to compare groups of categorical variables. In all the statistical analyses of the study, a value of P < .05 was accepted as statistically significant.
Results
Participants’ Data.

The mean tension force value applied by the surgeons to the cable was determined to be 413.94 ± 186.44 (range: 97–764.5) Newtons in those with ≤5 years of orthopedic surgery experience, 495.74 ± 301.04 (range: 76.22–1251.18) Newtons in those with 5–15 years, and 435.44 ± 163.94 (range: 152–794) Newtons in those with >15 years of experience. Experienced orthopedic surgeons applied more mean tension than less experienced surgeons; however, the difference among the 3 groups was statistically insignificant (P = .679) (Figure 2). The tension force values applied to the cable by the surgeons according to their years of orthopedic surgery experience. The experienced surgeons applied more mean tension than the less experienced surgeons; however, the difference among the 3 groups was statistically insignificant (P = .679).
The mean tension force applied to the cable was 402.03 ± 185.14 (range: 76.22–764.5) Newtons by the surgeons who performed <20 revision hip surgeries per year, 561.38 ± 277.49 (range: 230.96–1251.18) Newtons by those who performed 20–40 revision hip surgeries per year, and 435.34 ± 149.51 (range: 152.4–628.21) Newtons by those who reported performed >40 surgeries per year. The tension force applied by the surgeons who performed more revision hip surgeries per year was greater than that of the surgeons who performed on fewer cases; however, the difference was statistically insignificant (P = .179) (Figure 3). The tension force values applied to the cable by the surgeons according to their number of revision hip surgeries per year. The tension force applied by the surgeons who performed more surgeries was greater than that of the surgeons who performed on fewer cases; however, the difference was statistically insignificant (P = .179).
The mean tension force applied to the cable was 470.13 ± 235.72 (range: 214.38–1251.18) Newtons for the surgeons who reported to have used <40 cables per year, 427.48 ± 208.26 (range: 76.22–692.8) Newtons for those who used 40–80 cables per year, and 400.37 ± 144.63 (range: 152.4–628.21) Newtons for the surgeons with a reported use of >80 cables per year. According to the number of cables used per year, the mean tension force applied was greater in those who used fewer cables compared to the surgeons who reported to have used more cables; however, the difference was statistically insignificant (P = .847) (Figure 4). The tension force values applied to the cable by the surgeons according to the number of cables they used per year. The mean tension force applied by the surgeons who used fewer cables was greater than those who reported to have used more cables; however, the difference among the groups was statistically insignificant (P = .847).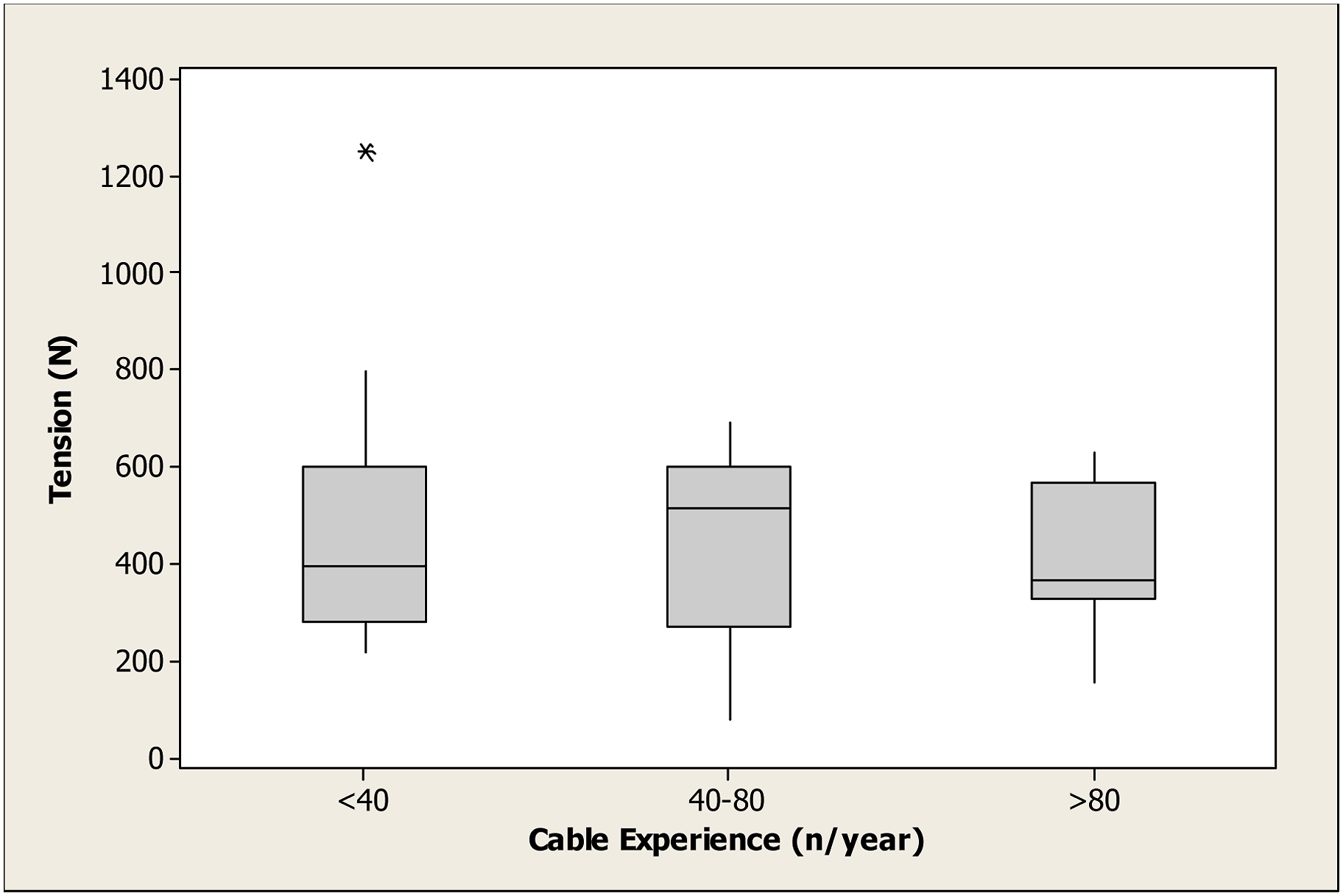
In 19 (35.2%) of the 54 participants, the force applied to the cable was found to be greater than the 490.33 N (50 kg) value recommended by the manufacturer for the 1.7-mm cobalt-chrome cable. No statistically significant difference was determined between the surgeon’s years of experience, the number of cases, and the number of cables used and the application of tension over the recommended maximum value (P = .475, P = .312, and P = .691, respectively). No breakage was observed in any artificial bone model or cable used in our study.
Discussion
In this study, the effect of the experience level of arthroplasty surgeons on correct tension adjustment of the cables commonly used in ETO fixation was investigated. Our first finding was that no statistically significant relationship could be established between the surgeons’ experience levels, the annual number of rTHA surgeries, and the number of cables used per year and their aptitude to adjust the cable tension at the values recommended by the manufacturer. Second, 35.2% of the arthroplasty surgeons included in our study applied more tension than the values recommended by the manufacturer during the experiment. Finally, no significant relationship was found between the application of the tension above the recommended value and the surgeons’ experience levels, the annual number of rTHA surgeries, and the number of cables used per year.
There are many previous studies that have examined ETO in patients who underwent complex total hip arthroplasty or total hip arthroplasty revision following periprosthetic fractures, infection, or aseptic loosening, and that have compared the results of the use of cables, and cable grip and cable plate systems used for fixation after ETO.1-3,13,14 In a retrospective study by Prudhon et al, 15 ETO was performed on 157 patients due to revision total hip surgery. In the fixation of the osteotomized trochanteric fragment, wires and cables were used with tension applied manually. During a 1-year follow-up period, no significant difference was observed in the patient series between wires and cables with respect to displacement. However, no additional information about the surgeons’ experience was given in the study. In another retrospective study including 612 ETO patients who underwent rTHA surgery, Abdel et al 1 stated that all ETOs were fixed horizontally using cables. The authors noted that the most common intraoperative and postoperative complication was fracture in the osteotomized fragment, adding that the cause of postoperative fracture might be the excessive tension applied to the most proximal cable. In many similar previous studies, the manual tension force applied without a calibrated tension gauge to the cable during fixation has been at the discretion of the surgeon applying the force, while there has been no detailed information about the surgeon’s experience.
There are very few studies related to the amount of tension that should be applied to the cables, which are widely used in the fixation of the osteotomized fragment or periprosthetic fracture, or that have evaluated the causes of complications [4-6]. Zhu et al 5 simulated a total hip arthroplasty revision surgery with ETO performed on the femurs of 10 fresh-frozen cadavers, and re-attachment of the osteotomized fragment was made with wires, cables and claw-plate. As a result of the vertical and lateral tension tests, the greatest movement with translation was reported to be in fixation with wire applied with manual tension. This was thought to be associated with the tension not being able to be checked. In a study by Canet et al, 6 trochanteric osteotomy was performed on a synthetic femur model; re-fixation of the osteotomized fragment was made with plate and cables after placement of the prosthesis, and a model was created that mimicked walking. The tension applied to the cables was at 50%, 100%, and 150% of the value recommended by the manufacturer. The researchers concluded that less tension applied to the cables reduced stability in the trochanteric osteotomy re-fixation and that the application of excessive tension provided no additional stability and could cause breakage of the cables. In these studies, while the stability of the tension values applied to the cables on the osteotomized fragment was evaluated, the relationship between the tension values and the experience level of the surgeon was not investigated.
Although the number of biomechanical and clinical studies about the tension applied to the cables in the literature are limited, there are some studies reporting about the disruption of the circulation to the bone due to excessive stripping of the vastus lateralis muscle or applying excessive tension to the cables as one of the most important causes of nonunion after ETO.3,7,16 Karakoyun et al 8 investigated the effect of excessive tension applied to the cable on bone circulation. In an experimental model, a cable of 2-mm thickness was placed in the mid-femoral diaphysis of 10 New Zealand rabbits and a tension of 400 N was applied. Blood flow changes in the femur were evaluated with scintigraphy and it was reported that the cables applied with tension significantly reduced the blood flow. In our study, however, it was found that 35.2% of the participants had applied tension above the values recommended by the manufacturer, while no significant relationship was detected between the application of excessive tension and the surgeon’s experience level.
This study had several limitations. First, the tests in our study were performed on a model bone, not a real one. Although it has been previously reported in other studies that the model bones we used in our study have very similar mechanical properties to real bones, it may be thought that cable tension adjustments on the real bone with varying bone stocks, encountered by surgeons in their daily practice, may be different.11,12 Second, in our study, no femoral stem was placed after ETO; thus, it can be deduced that this may affect the tension values applied by the surgeons. Finally, since our study was performed on artificial bones, we were incapable of reporting the clinical results of the application of excessive tension on cables.
Errors in tension adjustments of the cables commonly used by arthroplasty surgeons during fixation after ETO can lead to intraoperative and postoperative complications. As a result of our study, in which we included arthroplasty surgeons with different experience levels, no significant relationship was found between their level of experience and the correct adjustment of cable tension. For this reason, we believe that the use of tensioners with calibrated tension gauges by orthopedic surgeons will help in reducing the number of complications that may occur due to the cable.
Footnotes
Author Contributions
Kerem Başarır: Conceptualization/design, methodology, data curation, formal analysis, writing manuscript. Mahmut Kalem: Methodology; data curation, formal analysis. Ercan Şahin: Conceptualization/design, supervision/oversight. Emre Anıl Özbek: Methodology; data curation, formal analysis. Mustafa Onur Karaca: Methodology; data curation. İbrahim Küçükkarapınar: Methodology. Ergin Tönük: Methodology.
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Each author certifies that he has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article. Our study was performed Department of Orthopedics and Traumatology, Ankara University.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent to Publish
All authors have given consent to publish this manuscript.
Consent to Participate
All authors have given consent to participate in this manuscript.