
Abstract
Introduction
The reverse shoulder arthroplasty is nowadays a treatment option for a variety of shoulder problems. As its incidence rose, also the number of complications increased, including intraoperative fractures.
Significance
We performed a systematic review and critical analysis of the current literature following the PRISMA guidelines. Our purpose was to: 1) determine incidence, causes, and characteristics of intraoperative fractures; 2) evaluate their current treatment options, possible related complications, reoperation rates, and the patients’ outcome; and 3) determine the overall incidence of each complication related to reverse shoulder arthroplasty. The articles were selected from PubMed medical database in April 2020 using a comprehensive search strategy. Rayyan software was used to support the selection process of the records. A descriptive and critical analysis of the results was performed.
Results
The study group included a total of 13,513 reverse shoulder arthroplasty procedures. The total number of complications was 1647 (rate 12.1%). The most common complication was dislocation (340 cases, rate 2.5%). Forty-six studies reported a total of 188 intraoperative fractures among the complications (rate 1.4%). The intraoperative fracture rate was 2.9% and 13.6% in primary and revision settings, respectively. There were 136 humeral fractures, 60% of them occurred in revision RSAs, during the removal of the previous implant, and involved the shaft in the majority of cases (39%). Glenoid fractures were 51 and occurred mostly during the reaming of the glenoid. We observed 7 further related complications (rate of 4%) and 3 reoperations (rate of 1.5%). The outcome was satisfactory in the majority of cases.
Conclusions
A comprehensive review on intraoperative fractures in reverse shoulder arthroplasties is presented. Results suggest favorable outcomes for all treatment methods, with a modest further complication rate. This investigation may aid in the treatment decision-making for these complications.
Keywords
Introduction
The reverse shoulder arthroplasty (RSA), designed by Grammont in the late 1980s, 1 is nowadays a treatment option for a variety of shoulder problems. From the classical cuff tear arthropathy (CTA), the indications expanded to glenohumeral arthritis with or without deficient rotator cuff, displaced three- and four-part proximal humerus fractures in the elderly or their sequelae, massive rotator cuff tears with or without pseudo-paralysis, glenoid bone loss, failed previous arthroplasty, and proximal humeral tumors. 2
Reverse shoulder arthroplasty has already been performed for more than 25 years in Europe, while in the USA it was approved by the FDA only in 2003. Since that year, we observed such a large increase in its incidence that in 2011 RSA comprised one-third of all shoulder arthroplasties implanted in the USA.3,4
As its incidence rose, also the number of complications, reoperations, and revisions increased.
Complications related to RSA have been well described and the complication rate has been reported to be four-times higher than in the anatomical total shoulder arthroplasty, 5 ranging from 19 to 68%.6-11
This variability seems to be caused by the heterogeneity of the studies in terms of different underlying indications, primary or revision procedures, different component designs, different populations, and surgeon experience. Moreover, the definition and inclusion criteria for reporting complications vary between authors.
Scarlat et al classified complications into nonspecific (infections, phlebitis, hematoma, and neurological complications of the brachial plexus) and specific complications (humeral and glenoid side). Specific complications on the glenoid side include intraoperative and postoperative fracture of the glenoid and acromion, late fracture of the scapula, notching, glenoid loosening, and dissociation of the glenoid component (disassembly of the glenosphere). On the humeral side, specific complications include intraoperative and postoperative fracture of the greater tuberosity, metaphyseal area or shaft, humeral loosening, and stress shielding. Other specific complications are shoulder instability and stiffness. 12
Zumstein et al in a systematic review on the problems and complications of RSA reported an overall complication rate of 24%, with the most common complication being instability (4.7%) followed by infection (4%). In their study, it appeared that most of the complications occurred postoperatively (20.3%), while the intraoperative ones were 3.7%. Nevertheless, it’s interesting to consider that all of the intraoperative complications were fractures. 9
Shah et al in a more recent systematic review analyzed several complications, including intraoperative humeral and glenoid fractures. They reported a rate of 1.8% for humeral fractures and .3% for glenoid fractures. 13
To our knowledge, very few studies described extensively the intraoperative fractures including possible causes, treatment options, reoperation rates, and outcomes.
For this reason, we performed a systematic review and critical analysis of the current literature aiming to: 1) determine incidence, causes, and characteristics of intraoperative fractures; 2) evaluate their current treatment options, their possible related complications and reoperation rates, and the patients’ outcome; and 3) determine the overall incidence of each complication related to RSA.
Materials and Methods
A systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and MetaAnalyses (PRISMA) guidelines. 14 The articles were selected from PubMed medical database in May 2020. The search terms used were (((Arthroplasty, Replacement, Shoulder) AND reverse) AND fracture))) OR (((Arthroplasty, Replacement, Shoulder) AND reverse) AND complication))) OR (((Arthroplasty, Replacement, Shoulder) AND reverse) AND intraoperative fracture))). All Level-I to IV studies in English, Spanish, and French language, which were published between 1995 and May 2020, were considered for inclusion.
Inclusion criteria were the implantation of RSA for any possible indication both in a primary or revision setting; reporting of subjective and/or objective outcomes and/or complications.
Studies were excluded if they met the following criteria: the use of any shoulder prosthesis other than RSA; less than 20 cases; a minimum mean clinical and radiographical follow-up shorter than 12 months; use of national registers; reporting of only 1 single specific outcome and/or complication; reviews, editorials, technique articles without reported patient outcomes, cadaveric studies, kinematic/computed model analyses, clinical guidelines, instructional courses, and case reports.
Rayyan free web software was used to remove duplicates and select eligible studies from the database findings. Two independent reviewers (
Data extracted from the studies included demographic information and clinical results.
Demographic data included the total number of cases and the minimum and mean follow-up.
Clinical results included any type of complications related to RSA. Alike Kempton et al, 15 we initially divided complications into 2 main groups: local complications and perioperative systemic complications. Local complications included all intraoperative and postoperative problems involving the operative extremity. Perioperative systemic complications included all other health-related adverse events initiated within 2 weeks of the operation (embolism, pneumothorax, and myocardial infarction).
Local complications were secondary classified according to Zumstein’s definitions, 9 with some rearrangements. A “complication” was defined as any intra or postoperative event that was likely to have a negative impact on the outcome (periprosthetic intra or postoperative fracture, infection, dislocation, nerve problems, aseptic loosening of any component, disassociation of the components, or glenoid screw problems), and “problem” as any intra or postoperative events perceived as adverse, but unlikely to affect the outcome (hematoma, thrombosis of the brachial vein, clinical scapular notching, tuberosity malunion or nonunion, prominent hardware, polyethylene wear, rupture of subscapularis or deltoid tendons, shoulder stiffness, cement extrusion, clinical heterotopic ossification, and broken hardware).
The studies that reported intraoperative fractures were further investigated for the RSA indications. These were first divided into 2 groups, primary and revision, and then subclassified under the leading diagnoses. The mean age of the patients was registered. Moreover, surgical data were scouted to find eventual intraoperative fracture leading cause, fixation techniques, related further complications, reoperations, revisions, and outcome. Further complications were defined as any intraoperative fracture-related event that was likely to have a negative influence on the patient’s outcome.
A priori registration of this systematic review protocol in the international prospective register of systematic reviews (PROSPERO) was made on July 5th, 2020 and it’s available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020180977.
Results
The search strategy returned 528 MEDLINE studies. After duplicates were removed, there were 524 studies for review; 95 records were marked as ineligible by automation tools and 4 were retrieved. Of the remaining 433 studies, 81 were excluded by title, 125 by abstract, and 80 by full text. In total 381 studies were excluded and 147 were included for the final analysis.,16-27,27-78,78-118 see Figure 1. PRISMA flow diagram.
Because of substantial study heterogeneity and small sample sizes, the data obtained from the selected studies were not adequate to perform a metaanalysis. For these reasons, a descriptive approach and critical analysis of the data were performed.
Overall Adverse Events Incidence.

The local problems were 161, representing a local problem rate of 1.2%, with hematoma being the most represented (68 cases, rate of .5%), followed by shoulder stiffness (21 cases, rate of .14%), and clinical heterotopic ossification (15 cases, rate of .11%).
The local complications were 1463, representing a local complication rate of 10.8%, with dislocation being the most represented (340 cases, rate of 2.5%), followed by infection (262 cases, rate of 1.9%), and acromial postoperative fracture (149 cases, rate of 1.15%).
The perioperative systemic complication rate was .2%, with 12 cases of embolism, 6 cases of pneumothorax, and 5 of myocardial infarction.
The 10 Most Common Local Complications and Problems.

aFX: fracture.
Forty-six studies15,46,66,69,119-134,134–157 reported a total of 188 intraoperative fractures (IFx) among the complications, representing a global IFx rate of 1.4%.
Thirty-five Authors reported 136 intraoperative humeral fractures (IHFx) (rate of 1%).
Twenty-five Authors reported 51 intraoperative glenoid fractures (IGFx) (rate of .37%). One Author reported a coracoid fracture (overall rate of .007%).
The mean age of these studies’ population was 72 years old and female sex was predominant. However, most of the Authors did not report the sex of the patients who had IFx, therefore this data is not available in our analysis.
In the studies that reported IFx, 53% (99 cases) occurred among 3439 primary RSA (rate of 2.9%), whereas 47% (89 cases) occurring among 650 revision RSA (rate of 13.6%).
The 40% (54 cases, rate in primary RSA of 1.5%) of IHFx occurred in primary setting, whereas 60% (82 cases, rate in revision RSA of 12.6%) in revision setting. The 86% (44 cases, rate in primary RSA of 1.3%) of IGFx occurred in primary RSA, for which cuff tear arthropathy and rheumatoid arthritis were the predominant indications. The 14% (7 cases, rate in revision RSA of 1%) occurred in revision setting.
IHFx involved the shaft in 53 cases (39%), the greater tuberosity in 37 cases (27%) of cases, and the metaphysis in 22 cases (16%). Four studies (24 cases) did not report the humeral area involved.
Twenty-eight Authors reported the treatment for IHFx.
Twenty-nine (80%) of the 37 greater tuberosity fractures were treated with sutures, whereas 4 (10%) did not require any fixation and were treated conservatively. One study reported 4 greater tuberosity fractures but did not report the treatment option used.
Thirteen (59%) of the 22 humeral metaphysis fractures were treated with cerclage wires, whereas 7 (31%) were treated conservatively and 1 case was treated with bone suture. One study reported 1 humeral metaphysis fracture without reporting the treatment option used.
Twenty-six (49%) of the 53 humeral shaft fractures were treated with cerclage wires and in 3 of them additional bone grafting was required. In 9 cases (17%) the stem was replaced with a long stem and among these, in 8 cases cerclage wires were also used and in 1 case additional bone grafting was required. In 2 cases (4%) the fracture was treated conservatively. In 1 case, plate osteosynthesis was used. Four studies reported 14 humeral shaft fractures without reporting the treatment option used.
Intraoperative Fractures and Treatment.
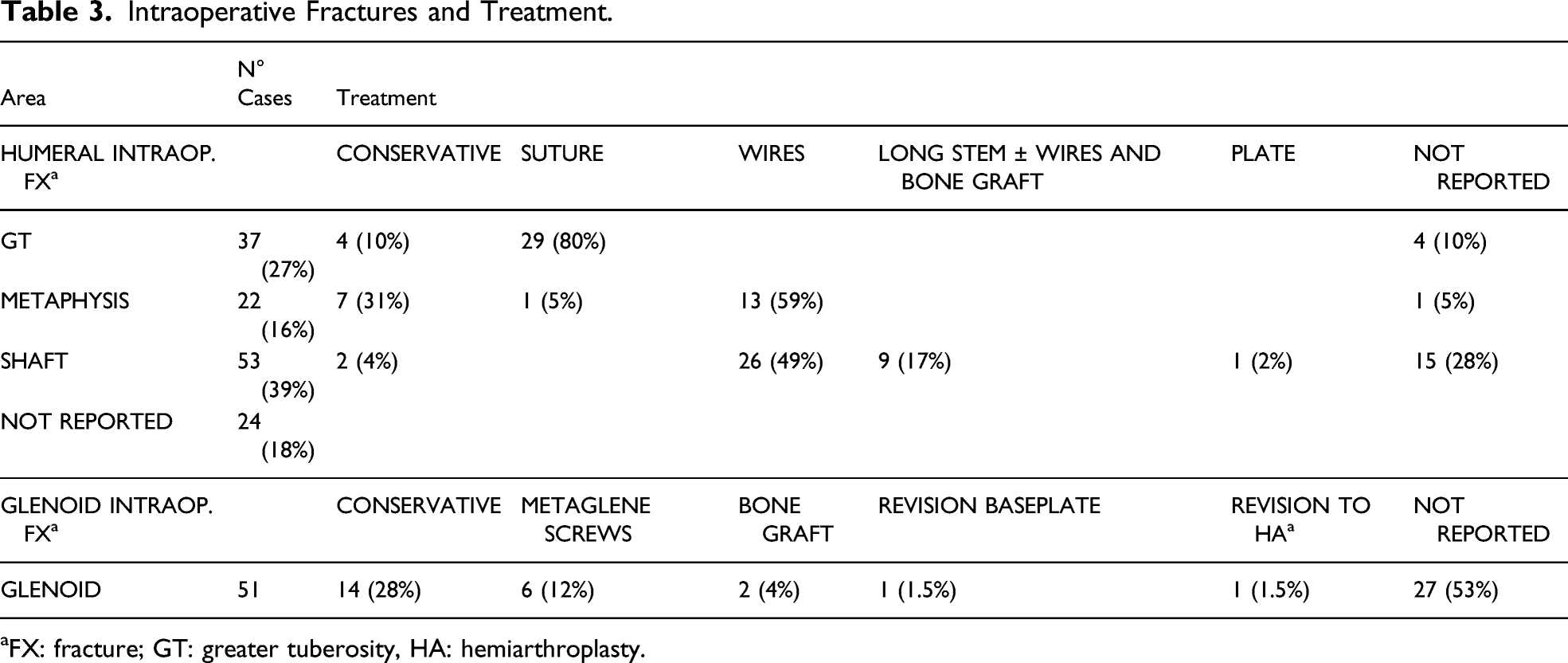
aFX: fracture; GT: greater tuberosity, HA: hemiarthroplasty.
Sixty-nine IHFx (51%) occurred during the removal of a previous implant or cement mantle, whereas 16 cases (12%) were caused by reaming of the humeral canal and 5 cases (3%) by final stem insertion. For the remaining 46 cases (34%) the intraoperative moment in which the fracture occurred or the leading cause were not specified.
Intraoperative Fractures and Cause/Intraoperative Moment.

aFX: fracture.
Fifteen of the 46 studies reported whether some type of further intraoperative fracture-related complication occurred or not. Among these, in 11 studies no further complications were reported, whereas 4 studies reported 7 further complications (rate of 4%): 3 nerve lesions caused by excessive compression from cerclage wires fixation used for 3 humeral shaft fractures; 2 instability cases in 2 humeral shaft fractures; 1 nerve lesion in 1 case of humeral shaft fracture; 1 glenoid loosening and 1 clinical scapular notching after 2 glenoid fractures.
There were only 3 reoperations (rate 1.6%) due to IFx: 2 revisions for instability occurred after 2 IHFx and 1 conversion to a hemiarthroplasty for glenoid loosening occurred after 1 IGFx.
Twelve of the 46 studies reported the outcome: this was satisfactory after 26 IHFx and poor after 1 IHFx complicated by nerve lesion that was not fully resolved at final follow-up. The outcome was satisfactory after 7 IGFx and poor after 1 IGFx complicated by glenoid loosening and required revision.
Discussion
RSA is a viable surgical treatment for many complex shoulder conditions and the interest in this procedure is growing as the indications continue to expand. Today it is commonly performed all over the world. However, it remains a difficult procedure and high rates of complications are still being reported. 134
By excluding any study focused on single specific complications or outcomes, we tried to give our review the most accurate possible design to evaluate the real complication rate.
In our analysis, the overall complication rate was 12.2%, which is much lower than the 68.5% reported by Zumstein et al, 9 but closer to the 15% and 16.1% reported by other Authors.158,159 Dislocation was the most common complication observed with a rate of 2.5%, lower than the 1 reported by Bohsali et al (5%) and Zumstein et al (4.7%).9,158
The second most common complication observed was infection with a rate of 1.9%. This data is in line with the 1.2% reported by Bohsali et al, 158 but lower than the 3.8% reported by Zumstein et al and the 2.4% reported by Shah et al.9,13
We observed a total of 469 periprosthetic fractures, representing a rate of 3.4%, lower than the 7.8% rate reported by Brusalis et al 159 Moreover, we observed a higher rate of postoperative fractures compared to intraoperative ones, while other Authors reported the opposite.13,158
These differences reflect the heterogeneity behind the study selection process, differences in inclusion and exclusion criteria, and large variability in reporting complications among Authors. For example, some Authors may decide to include perioperative systemic medical complications, such as pulmonary embolism, believing that this method of reporting provides a more complete picture of the perioperative and postoperative course, while most investigators only report complications related to the shoulder.141,149
We observed 188 IFx, representing a rate of 1.4%, lower than the 3% rate and the 2.1% reported by other Authors.9,13 IHFx were more common (rate of 1%) than IGFx (rate of .37%).
In the studies that reported IFx, the indications for RSA were usually reported for the whole cohort rather than specifically for the patients who had the IFx. This is why it was not possible to set up a correlation between indications and the risk of IFx. In general, we observed much less detailed reports for IGFx than IHFx. For example, for 53% of IGFx the treatment was not reported, and for up to 73% of IGFx the intraoperative cause was not explained. This may partially influence the precision in which an overview of IGFx can be provided.
We observed an IFx rate of 13.6% and 2.9% in revision and primary RSA, respectively. This data is mostly determined by the high rate of IHFx in revision RSA (rate of 12.6% in revision vs. 1.5% in primary RSA), occurring during the removal of a previous implant or cement mantle. Differently from IHFx, IGFx were far less related to the type of RSA procedure and occurred substantially at the same rate in primary (1.3%) and revision RSA (1%).
The choice of surgical approach may influence the fracture rate. In revision cases, Valenti et al. reported that a deltopectoral approach facilitates the extraction of both humeral stem and cement, thus preventing the fracture of the diaphysis. 122 Differently, an IGFx is observed more frequently in the superolateral approach, probably related to the strength applied on the inferior retractor. 1
Special attention must be given to arm positing through the whole procedure, as an extension, rotation, and translation to dislocate or reduce the humeral head often result in IFx. 159
Operative planning is mandatory, especially for revision surgeries, whereas modular revision sets, including long stems, revision components, as well as plate and cerclage systems or sutures, are mandatory, besides all the removal instrumentation. 133 Particular attention must be given to the quality of the humeral bone stock, component surface coating, and the thickness of the humeral cement, especially in elderly females, before attempting component extraction. Valid options are humeral osteotomies or humeral windows, but we need to remember that IFx may still occur despite these techniques.119,124
Alternatively, the use of the cement-within-cement technique and a shorter humeral stem to revise a cemented humeral component can be considered, to reduce the risk of distal fractures.122,133
The use of convertible or modular shoulder arthroplasty systems could reduce in the future the need to remove the stem and the incidence of humeral fractures. A comprehensive low incidence of IFx in revision RSA (4.3%), compared to other revision series, is shown when revision RSA is made on surface arthroplasties, due to the absence of stem or cement. 128
Finally, always remember that overstuffing the humeral canal while broaching or during press-fit humeral stem insertion can result in metaphyseal fractures. 160 Propagation of cracks can occur during cementation and implantation of the prosthesis and using cables can prevent this from happening.46,140
The treatment of IHFx depends on the location, the fracture displacement, the bone quality, and the stability of the component/bone interface. Greater tuberosity fractures may be treated with suture fixation if there is any displacement, or left in situ and observed if they are nondisplaced and do not extend distally. In our analysis, 80% of greater tuberosity fractures were treated with sutures and 10% conservatively.
In case of nondisplaced or minimally displaced fractures isolated to the calcar or metaphysis, with no extension into the humeral diaphysis, the stabilization of the stem with a press-fit implant or cemented stem and/or cerclage wiring allows having good stability of the implant and the consolidation of the fracture. In our analysis, 59% of metaphyseal fractures were treated with cerclage wires. A long-stemmed implant and adjunct fixation with wires should be used if the humeral implant stability is in question, for example in shaft fractures. In our analysis, 17% of shaft fractures were treated with a long-stem implant, while 49% with cerclage wires only. Bone grafts can be used in cases of bone loss.124,144,160
IGFx are usually focal and small. Partial fractures seem to not compromise the long-term fixation of the prosthesis and affect the postoperative care or rehabilitation. However, in case of complete IGFx, the effects may be dramatic and must be avoided. They occur mostly during reaming (20% of cases). Technical care is required to assess the glenoid and accurate placement and orientation of the central peg of the baseplate remain difficult. When the glenoid is extremely soft or brittle, hand reaming may be a good option as pneumatic power drills with high torque may cause a fracture. 161 A fracture can occur in case of cuff tear arthropathy, rheumatoid arthritis, and osteoporosis when the glenoid is eroded far medially and the bone is brittle. The danger may be anticipated on standard x-rays, but a CT scan is indicated to obtain more precise information concerning the orientation of the prosthesis and the relative danger to perforate and breaking the glenoid. When an IGFx occurs, it can be managed conservatively when the fragment is small (28% of cases). In case of a bigger fragment, it can be fixed using the metaglenoid screws (12% of cases), with or without the support of bone graft. In a completely unstable situation, conversion to hemiarthroplasty may be necessary.
Coracoid intraoperative fracture is extremely rare (overall rate of .007%).
The postoperative outcome was not extensively reported (12 studies among 46), however, IFx seem to not affect it substantially and it was satisfactory in the majority of cases.
Conclusion
Intraoperative periprosthetic fractures represent a major challenge for orthopaedic surgeons in reverse shoulder surgery. Further investigations are needed to reduce their risk. While these complications cannot be completely avoided, a better understanding of their causes and/or patient risk factors may help the surgeon to decrease their frequency. Moreover, convertible or modular shoulder arthroplasty systems could reduce the risk of fractures in the future.
The improvement of surgical techniques and the achievement of higher fracture union rates are the keys to overcome these complications, while still obtaining good shoulder function.
Footnotes
Author Contribution
All Authors equally contributed to this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.