
Abstract
Background
The new edited AO/OTA-2018 classification of pertrochanteric fractures was revised and no longer based on the status of lesser trochanter. This paper aimed to explore the clinical and technical outcomes among the subgroups (31A1 and 31A2) of the new classification treated with cephalomedullary nails.
Methods
A retrospective research of 154 patients diagnosed with pertrochanteric fractures (AO/OTA-2018 31A1.2/3 and 31A2.1/2/3) treated with intramedullary nails was conducted. The baseline data and outcomes were compared among the subgroups. The outcomes included tip-apex distance (TAD), Cal-TAD, Parker ratio, neck shaft angle (NSA), blood loss, varus displacement, and over lateral sliding rate of the blade.
Results
There were 154 cases involving 48 males and 106 females. The average age was higher in the sub-classifications of A2.2 and A2.3 than A1.2. Furthermore, the subgroups of A2.2 and A2.3 presented inferior outcomes with regard to blood loss and reduction quality score than A1.2 and A1.3. The subgroup of A2.3 was further poor with respect to calcar fracture gapping in the anteroposterior view and excessive lateral migration occurrence rate than A1.2.
Conclusions
Complex pertrochanteric fractures indicated inferior outcomes compared to simple sub-classifications, which might lead by the incompetent of lateral wall and instability of the fracture. The newly proposed AO/OTA-2018 classification was conductive to forecast the prognosis.
Keywords
Introduction
With the population ages, pertrochanteric fractures continue to increase and remain a great challenge.1,2 For the classification of pertrochanteric fractures, the AO/OTA combined fracture classification system is widely accepted and discussed.3,4 In the 1996 and 2007 versions, the numbers of intermediate fragments are used for the classification of pertrochanteric fractures, which especially emphasize the importance of lesser trochanter. Researches have confirmed that the classification is benefit for the description of fracture characteristics and guiding the treatment in the clinical management.5,6
Based on the thickness of lateral wall, pertrochanteric fractures are revised in the AO/OTA-2018 fracture classification compendium. 7 It is worth noting that lesser trochanter is no longer used as the secondary classification index. A1 classification is characterized with simple fractures and intact lateral wall (thickness > 20.5 mm). A2 classification is defined as multi-fragmentary fractures with lateral wall incompetent (≤20.5 mm).8,9 Furthermore, the fracture in the coronal plane is also taken into consideration for the subtypes of A2 fractures. 10
In recent years, the intramedullary nails are increasingly favorable in the clinical practice.11,12 There are already researches explored the prognosis of pertrochanteric fractures fixed with intramedullary nails according to the old AO/OTA classification version,13,14 which indicated the outcomes of different subtypes. However, the baseline data and clinical prognosis based on the new revised AO/OTA-2018 sub-classification are still out of reach. We hypothesized that multi-fragmentary fractures with incompetent lateral wall suffered inferior outcomes compared with intact lateral wall fractures. This research was conducted to investigate the impact of the fracture classification in pertrochanteric fractures on outcomes and mechanical complications.
Methods
Patients and Inclusion Criteria
This retrospective research was approved by the institutional review board and all the patients enrolled had signed informed consent. From January 2017 to May 2020, patients diagnosed with pertrochanteric fractures and treated with PFNA-II (proximal femoral nail anti-rotation) were retrospectively reviewed. The inclusion criteria were as follow: (1) classified with AO/OTA-2018 A1.2/3 or A2.1/2/3 fractures; (2) an isolated fresh fracture; (3) age ≥60 years; (4) complete imaging data including preoperative CT (computed tomography) scans, immediate postoperative radiology and follow-up images at least 6 months postoperatively; and (5) fractured by low energy injury. Patients with pathological fractures, open fractures, and absent of radiographs were excluded. The A1.1 subtype was excluded owing to the rare occurrence and conservative management.
Data Collection and Parameters Measurement
The baseline data were collected from the medical record. The baseline characteristics comparison included age, gender, side involved, fracture type, ASA (American Society of Anesthesiologists) score, blood loss, and operation time. The fracture type was judged by the preoperative 3D CT images according to the version of AO/OTA-2018 classification.7,10
The reduction quality score was based on the criteria proposed by Prof. Chang. 15 Mechanical complications were defined as varus displacement (NSA reduced >10° during follow-up) 16 and excessive lateral sliding of the blade (lateral sliding ≥10 mm during follow-up). 17 The NSA, lateral sliding distance, calcar fracture gapping, and Parker ratio were measured and evaluated according to the methods previously reported.18-21 TAD is calculated by the distance from the tip of the blade to the apex of femoral head on the AP (anteroposterior) and lateral radiographs. 22 Cal-TAD differs from TAD on the anteroposterior radiograph changed as calcar-referenced tip-apex distance. 23 The classification and technical data were judged and measured by 2 independent researchers including a fellowship-trained orthopedic surgeon and an orthopedic resident. The software of Adobe Photoshop CC 2018 was used for the technical-related data calculation. The intra-class correlation coefficient (ICC) was also performed to judge the intra-observer reliability and was calculated as good (>.800). The mean value of the data calculated by the 2 observers was used for statistical analysis. Disagreements were settled by a senior researcher.
Surgical and Postoperative Management
Patients were positioned in the supine position on a fracture traction table for the fracture reduction and internal fixation. With the guidance of intraoperative fluoroscopy, routine closed reduction maneuvers were performed to get the fracture alignment. The rehabilitation process was individually performed according to the patient’s physical capability and willingness. With good physical strength, early weight-bearing standing and walking were encouraged; otherwise, bed rest was recommended for 1 month, with no sitting and turning restrictions.
Statistical Analysis
The SPSS 22.0 software was used for statistical analysis (SPSS Inc, Chicago, IL, USA). Continuous data were presented as mean and standard deviation. Categorical data were presented as count and percentage. For comparing the continuous variables among groups, the ANOVA (analysis of variance) test was performed. The Kruskal-Wallis test was used for nonnormally distributed variables. For the frequencies, the Chi-square or Fisher exact test was conducted. The P value <.05 was defined as statistically significant.
Results
Patient Characteristics and Grouping
Demographic Data Comparison Among Groups.

ASA, American Society of Anesthesiologists.
Clinical Outcomes and Complications
The Clinical Outcomes Comparison Among Groups.
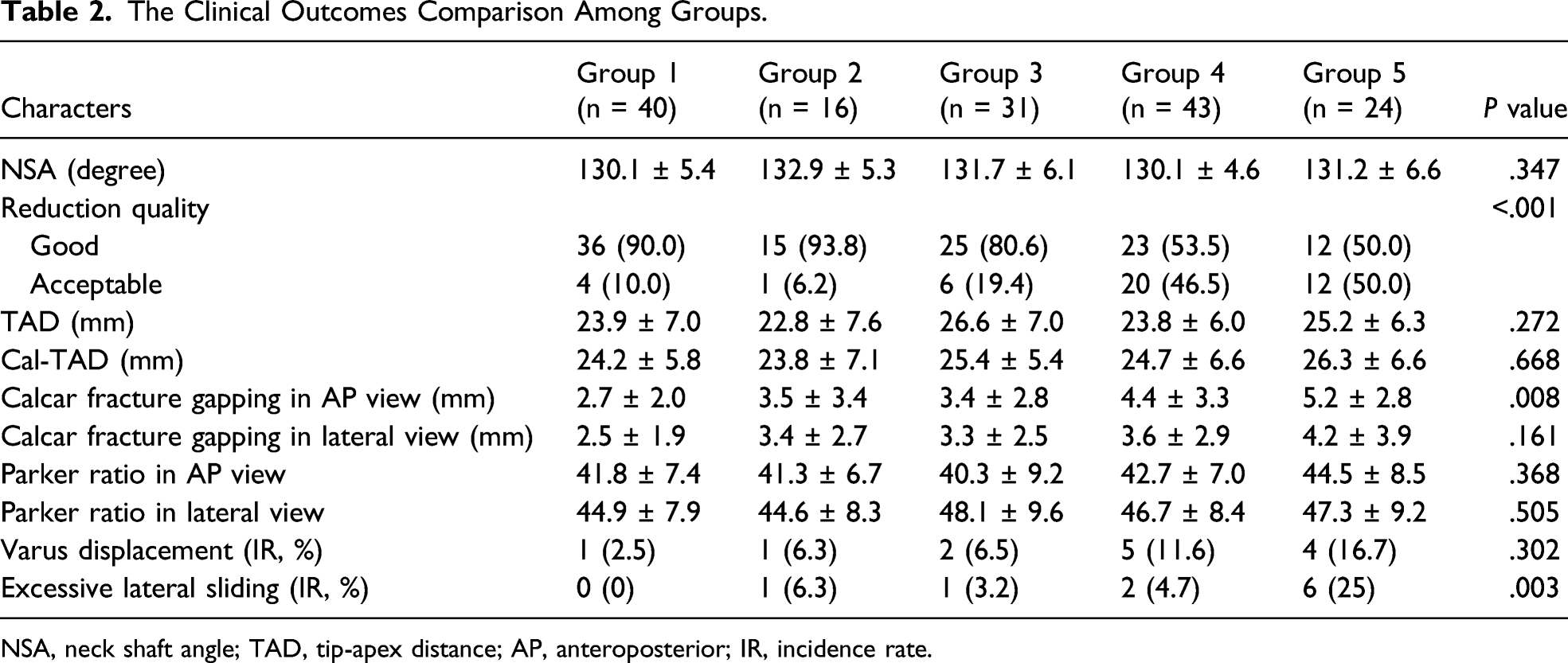
NSA, neck shaft angle; TAD, tip-apex distance; AP, anteroposterior; IR, incidence rate.
Discussion
There are already relevant researches analyzing the outcomes among different sub-classifications according to the previous AO/OTA classification. Von et al 24 revealed that A2 subtypes indicated higher incidence of implant failure compared with A1. Zhu et al 14 noted that the sliding distance was significantly different for A1 and A2.1 compared with A2.2 and A2.3. This study retrospectively analyzed 154 consecutive pertrochanteric fractures treated with intramedullary nails. The characters and outcomes were compared according to the new AO/OTA-2018 classification version. We concluded that complex pertrochanteric fractures with incompetent lateral wall indicated inferior outcomes compared to simple sub-classifications.
The concept of lateral femoral wall is defined as the cortex of the drilling site for screw or blade firstly introduced by Gotfried, 25 which provides a natural buttress support for the fixation. Researches have confirmed the importance of lateral wall in the management of pertrochanteric fractures. A large cohort study conducted by Prof. Palm 26 revealed that incomplete of the lateral wall was an independent risk factor for reoperation after sliding compression hip screw fixation. In 2013, Hsu and colleagues 8 quantified the definition of lateral wall thickness and confirmed that the thickness was associated with intraoperative lateral wall fracture and postoperative treatment failure fixed by DHS (dynamic hip screw). The reference line of the distance measurement was set as 30 mm below the innominate tubercle and angled at 135° upward to the midline between the 2 cortex lines in the AP view. The threshold value was set as 20.5 mm for predicting lateral wall fracture and usage of DHS to reduce the implant failure. This standard had been accepted and included in the AO/OTA-2018 version for the distinction of subtypes A1 and A2.
The fracture mapping showed that the coronal fracture line in A1 and A2 pertrochanteric fractures ran inferiorly through the lesser trochanter or the posteromedial cortex 27 and the lateral femoral wall would be partially fractured and incompetent. Therefore, the area of lateral wall in the coronal plane might be comprehensive to evaluate the possibility of lateral wall rupture. 28 The 3D CT reconstructions presented more details of coronal plane fractures compared with plain radiographs. 29 Therefore, the integrity of lateral femoral wall in the coronal plane should also be taken into account for the classification. 30 Afterward, we proposed10,30 to take both AP and lateral views into consideration for the A2 subtypes. The coronal plane was divided into the posterior greater trochanter, the intertrochanteric crest, the lesser trochanter, and the posteromedial cortex for the sub-classification. The blank space of A2.1 was filled with incompetent lateral wall and a large posterior coronal banana-like free fragment containing the lesser trochanter.
The greatest change in the AO/OTA-2018 fracture classification compared with the old version is that the lesser trochanter is no longer used as the secondary classification index. With a clinical perspective of the lateral wall, the intertrochanteric fractures are classified into 3 types: intact, vulnerable, and fractured. The change is also adapted to the current clinical management. Recently, most orthopedists prefer not to fix the lesser trochanter fragment routinely on account of complexity and uncertainty prognosis. 11 Researches have also verified that the status of the lesser trochanter makes no significant difference on the outcomes fixed by DHS or PFNA.31,32 Furthermore, Pradeep et al 33 revealed that lateral wall fracture was an independent risk factor leading to worse radiological and clinical outcomes.
The new classification also proposed a standard for the application of DHS, which is benefit for decreasing the treatment cost. The lateral wall is vulnerable and easy to rupture during operation for subtypes of A2. Therefore, the classification advocates implant fixation of A2 subtypes with intramedullary devices and A1 fractures with DHS. 8 However, it is worth noting that the biomechanical strength of lateral femoral wall is relatively weak in osteoporotic patients and the intact lateral femoral wall (A1) may also be fractured during operation.8,11,26,34 As a consequence, some surgeons prefer to choose cephalomedullary nails in all trochanteric hip fractures, regardless of intact (A1) or vulnerable patterns (A2).35,36
Some limitations should be taken into account in this research. This research was a retrospective analysis and had inherent bias. The amount of the cases enrolled in each group was relatively small and might lead to potential bias. Therefore, prospective study with a large sample size is necessary for drawing more powerful conclusions.
In conclusion, the AO/OTA-2018 classification for pertrochanteric fractures (A1 and A2) was effective to forecast the clinical prognosis, which was compared with the old version. Complex pertrochanteric fractures indicated inferior clinical outcomes compared to simple sub-classifications. More attention should be paid for the complex pertrochanteric fractures to improve the stability of the fixation and ensure better outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by funding from the National Nature Science Foundation of China (NSFC No. 81772323).