
Abstract
Introduction
Reportedly, wearable robots, such as the hybrid assistive limb (HAL), are effective in the functional recovery of various locomotor disabilities, including disrupted walking, restricted range of motion, and muscle weakness. However, the effect of walking exercises with a HAL on the kinematic and kinetic variables of lower limb joint function is not yet fully understood. Therefore, the purpose of this study was to elucidate the effect of HAL on the kinematic and kinetic variables of lower limb function in patients 5 weeks after total knee arthroplasty (TKA).
Materials and Methods
Nine patients (ten knees) in the HAL training group and nine patients (nine knees) in the control group underwent TKA. HAL training was initiated 1–5 weeks after TKA, and general rehabilitation was performed in the control group. Gait analysis was performed on each patient using a motion analysis system at 5 weeks after TKA. We compared the effects of the joint angles of the walking cycle between groups, and investigated the effect of the walking cycle’s joint angles on step length.
Results
In the HAL group, the odds ratio of hip extension was as large as 1.741, while that of knee swing was as large as 1.501. These 2 variables were significant between the 2 groups. Knee swing and varus significantly affected step length.
Conclusions
Our results suggest that training by wearing HAL after TKA increased the mobility of the knee and hip joints during early postoperative walking, and that walking ability was improved by increasing the step length.
Introduction
Total knee arthroplasty (TKA) is among the most common surgical procedures performed worldwide for knee osteoarthritis (KOA) and rheumatoid arthritis (RA). It is important to promote appropriate rehabilitation to regain walking and mobility at an early stage after TKA. 1 Thus, general rehabilitation is often performed after TKA to improve the range of motion of joints, muscle strength, and balance.2,3 The Western Ontario and McMaster Osteoarthritis Index is a tool used by patients to evaluate items related to pain and function after TKA, but the evaluation of walking ability is by no means sufficient. 4
In recent years, robots have been for exercise therapy in the field of rehabilitation.5,6 Wearable robots, such as the hybrid assistive limb (HAL, Cyberdyne Corporation, Tsukuba, Japan), are reportedly effective for the functional recovery of various locomotor disabilities, including disrupted walking, restricted range of motion (ROM), and muscle weakness.7,8 The HAL is an assisted training device that provides exercise in response to the wearer’s ROM or voluntary muscle contraction, or to ground reaction force signals caused by shifts in the wearer’s weight. 9 Yoshioka et al. conducted knee joint extension training using a single-joint HAL device to provide rehabilitation treatment targeted at improving knee joint function after TKA and reported immediate improvement of the extension lag without increasing knee pain. 10
The authors previously reported the effects of walking exercises with single-leg HAL in post-TKA rehabilitation. 11 It was shown that, compared to the control group, the group that practiced with HAL improved walking speed and step length at 2 and 4 weeks after surgery. However, that report did not mention changes in kinematic and kinetic variables, such as joint angle, joint moment, and ground reaction force during walking. Therefore, it is as yet unclear how walking exercises with HAL affect the kinematic and kinetic variables of lower limb joint function.
The purpose of this study was to verify the effect of HAL on the kinematic and kinetic variables of lower limb joint function at 5 weeks after TKA. In this study, we hypothesized that HAL intervention would increase the mobility of the lower limb joint movements and increase the exerted joint moment.
Materials and Methods
Participants
Patients’ preoperative baseline characteristics.

Values are expressed as numbers or as mean ± SD. Student’s t-test was used for the statistical test. BMI: body mass index; OA: osteoarthritis; RA: rheumatoid arthritis; TKA: total knee arthroplasty; SD: standard deviation.
This study was approved by the ethics committee of our institution (no. e155). We explained the purpose of the study to the patients in verbal and written forms, and written consent was obtained from all patients.
Surgical Procedure
The surgical procedure was similar to that described in our previous report. 10 Under general anesthesia, a midline skin incision was made, and a medial parapatellar approach was used. The patella was not replaced, and the posterior cruciate ligament was retained. The implants used were the NexGen® or Persona® (Zimmer, Warsaw, IN, USA) for the femoral component, and the NexGen CR Stem Tibia or NexGen Trabecular Metal Monoblock Tibia (Zimmer, Warsaw, IN, USA) for the tibial component.
Hybrid Assistive Limb Intervention
HAL training was conducted 1 to 5 weeks after TKA. The total number of HAL interventions ranged from 10 to 12 during the 4-week period. 11 There was no significant difference in the total physical therapy time, including HAL training, between both groups during the HAL intervention period. Five weeks after TKA, patients in both groups underwent the same physical therapy. The single-leg version of the HAL (medium size) was placed on the operative side, and the Cybernic Voluntary Control mode was used. The gain in assistive torque at each joint in response to the bioelectrical signals was controlled by a therapist so that the patient could move the knee joint sufficiently and easily within the ROM without aggravating pain or the presence of pain and extension lag, and the walk pattern was as normal and symmetrical as possible. First, repetitive knee flexion/extension exercises within the range in which pain was not aggravated or was absent were performed for less than 20 min with the patient in the sitting position. Second, gait training with HAL was conducted on a level ground at a comfortable speed while maintaining good gait posture for less than 20 min. To prevent falls, a wheeled walker was used during gait training with HAL.
Outcome Measurements
Gait analysis was performed on each participant in the HAL and control groups using a motion analysis system at 5 weeks after TKA. For the measurement, a 3-dimensional motion analysis system equipped with eight infrared cameras and two ground reaction forces was used. Prior to the gait analysis, we recorded the following patient data: height, weight, leg length (anterior superior iliac spine to medial malleolus), anterior superior iliac spine width, knee joint width, and ankle joint width. The patients walked barefoot along a level walkway at their habitual speed, and an average of three gait trials was collected for each participant and used for analysis. According to a lower extremity model of the Plug-In-Gait marker set, which is a widely used standardized marker arrangement for three-dimensional motion analysis, 9.5-mm-diameter reflective markers were placed directly over the following bilateral anatomical landmarks: anterior and posterior superior iliac spines, lateral thighs, lateral femoral epicondyles, lateral shanks, lateral malleoli, calcanei, and the tops of the feet at the base of the second metatarsal. After the reflective markers were attached, each patient was instructed to stand barefoot for a single static calibration in the standing position before gait analysis, and then instructed to step on a floor-mounted force plate using the lower limb. Patients were allowed to perform several preparation trials.
From the results of the walking measurement, the step length, angle change, and joint moment of the lower limb joint in a walking cycle were calculated. The step length was measured as the distance between the left and right heel markers when the heel of the lower limbs on the HAL training side touched the ground floor. The position data of the markers and joint angles acquired from the Plug-In-Gait model and ground reaction force data were low-pass filtered using a Butterworth filter. The results of walking measurement were time normalized to the percentage of gait cycle (100%: heel-strike to heel-strike) using spline interpolation. For the joint angles, the hip joint, knee joint flexion and extension, ankle plantar flexion, and dorsiflexion were calculated for a walking cycle, and the change in the knee joint in the varus direction at the initial stance phase was calculated. For the joint moment, the joint moment on the sagittal plane of the lower limb joints during the stance phase was calculated.
Statistical Analysis
Normality of the data was tested using the Shapiro-Wilk normality test. Differences in preoperative patient characteristics were analyzed using Student’s t-test for continuous variables and Fisher’s exact test for categorical variables. A t-test was performed on the joint angle of the walking cycle, the joint moment during the walking stance phase, and the step length and average values of the HAL and control groups were compared. When the normal distribution was not found as a result of the Shapiro-Wilk normality test, Mann-Whitney U-test was performed. The effect size (Cohen’s d) was also calculated.
Furthermore, using a generalized linear mixed model (GLMM), we compared the effect of the joint angle of the walking cycle on the HAL and control groups, and evaluated the effect of the joint angle of the walking cycle on the step length.
All analyses were performed using IBM SPSS Statistics version 25.0. (International Business Machines Corporation, Chicago, USA) The level of significance was set at P < .05.
Results
Average values of the joint angles in the walking cycle.

HAL: hybrid assistive limb; SD: standard deviation; Hip_ext: maximum hip extension during the stance phase; Knee joint angle: (+) flexion, (-) extension; IC: initial contact; LR: loading response; Mst: mid stance; TS: terminal stance; PSw: pre-swing; Sw: swing phase; Ankle-DF: Ankle Dorsal Flexion; Ankle-PF: Ankle Plantar Flexion.
†: P value are derivated from student’s t-test. ††: P value are derivated from Mann-Whitney U-test.
d: Cohen’s d.
Average values of the joint moment during the stance phase.

HAL: hybrid assistive limb; SD: standard deviation; Knee_ext: Maximum knee extensor moment; Knee_1abd: Maximum knee abductor moment during early stance phase; Knee_2abd: Maximum knee abductor moment during late stance phase; Hip_ext: Maximum hip extensor moment; Hip_flex: Maximum hip flexor moment; Ankle_PF: Maximum ankle plantar flexor moment
†: P value are derivated from student’s t-test. ††: P value are derivated from Mann-Whitney U-test.
d: Cohen’s d
The t-test (Welch’s correction) revealed a significant difference in step length between the HAL and control groups (t = 5.06, P = .001, d = 2.74). In the HAL group, the average step length was .63 ± .03 m, which was a relatively large value, while in the control group, the step length was .46 ± .09 m, which was small.
Generalized linear Mixed Models showing differences in the effect of joint angles in the walking cycle using a hybrid assistive limb.

Knee_varus: amount of change of the knee joint in the varus direction during the initial stance phase; AICc: corrected Akaike’s Information Criterion corrected, BIC: Schwarz’s Bayesian Information Criterion.
In Model 1, the groups (HAL/control) were used as the dependent variable, and the 3 variables (Hip ext, Knee Sw, and Knee varus) that showed a large effect on the joint angles of the walking cycle were used as explanatory variables. As a result of the analysis, the odds ratios of Hip ext, Knee Sw, and Knee Varus were 1.451, 1.407, and .384, respectively, among which only the Knee Sw was significant. The model goodness of fit was 23.144 for the corrected Akaike Information Criterion (AICc) and 24.064 for the Bayesian Information Criterion (BIC).
Model 2 used the two variables (Hip ext and Knee Sw) with a small P-value in Model 1. The model goodness of fit was 22.560 for the AICc and 23.794 for the BIC, which were smaller than those of Model 1, and the goodness of fit was improved, but Knee Sw, which was significant in Model 1, was no longer significant.
In Model 3, the interaction of Hip ext and Knee varus was added to the two variables of Model 2. As a result, the odds ratio of Hip ext was as large as 1.741, and that of Knee Sw was as large as 1.501; both of these variables were significant. However, the interaction between Hip ext and Knee varus was not significant. The goodness of fit of this model was 21.801 for the AICc and 22.722 for the BIC, which were the smallest values among the three models.
Among the three models, the goodness of fit of Model 3 was the best for both the AICc and BIC. The positive discrimination rate between the HAL and control groups was identical, at 84.2%, in all models.
Generalized linear mixed models showing the Effects of joint angles on step length in the walking cycle.
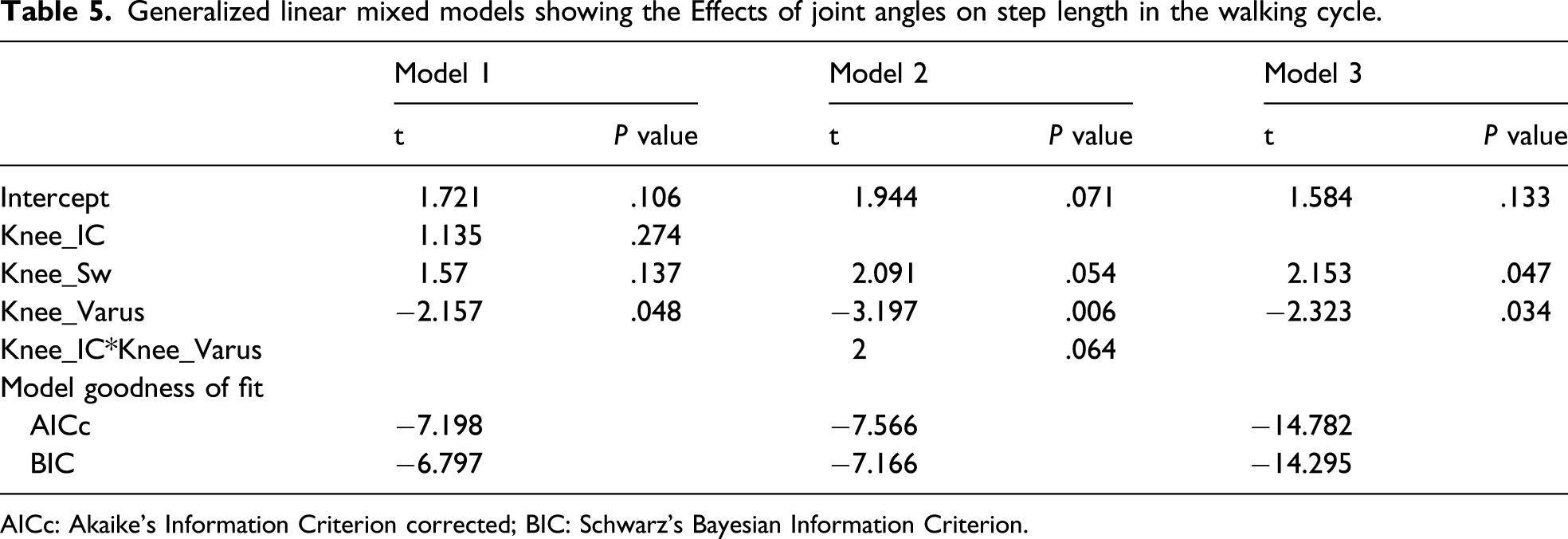
AICc: Akaike’s Information Criterion corrected; BIC: Schwarz’s Bayesian Information Criterion.
In Model 1, the step length, which was significantly different between the two groups, was used as the dependent variable, and the three variables (Knee at initial contact [IC], Knee Sw, and Knee varus) of the joint angle of the walking cycle, which were highly correlated with the stride length, were used as explanatory variables. The t-values of Knee IC, Knee Sw, and Knee Varus were .274, .137, and .048, respectively; only the Knee Varus was significant. The model goodness of fit was −7.198 for the AICc and –6.797 for the BIC.
In Model 2, the interaction between Knee IC and Knee Varus was used for the 2 variables (Knee Sw and Knee varus) whose P-values were small in Model 1. Similarly, only the Knee Varus was significant, and the model goodness of fit was −7.566 for the AICc and 7.166 for the BIC, which were smaller than in Model 1, and the goodness of fit improved slightly.
In Model 3, the interaction between Knee IC and Knee Varus was deleted from Model 2. As a result, these two variables were significant. The goodness of fit of this model was −14.782 for the AICc and –14.295 for the BIC, which were the smallest values among the three models. Comparing the goodness of fit of these models, the goodness of fit of Model 3 was superior for both the AICc and BIC.
Discussion
In the present study, to verify the training effect using HAL, we performed gait analysis at 5 weeks after TKA. Compared to the control group, in the HAL group, hip extension increased by approximately 1.7 times, and knee flexion during the swing phase increased approximately 1.5 times. Furthermore, step length was larger in the HAL group.
We reported an improvement in postoperative walking ability in a previous case report using a single-leg version of HAL. 12 Furthermore, in the HAL group, pain was significantly reduced 2 weeks after surgery, and both walking speed and step length improved 4 weeks after surgery. 11 In the present study, the mobility of hip extension in the late stance phase of walking was increased in the HAL group as a result of the pain reduction by HAL training and the promotion of sufficient load by wearing HAL. Increased mobility of hip extension in the late stance phase of walking stretches the iliopsoas muscle that acts on hip flexion, and it is thought that it enables the patient to exert greater power for the hip flexion movement toward the swing phase. 13 In the present study, there was no statistical significant difference in the hip moment between the HAL training group and the control group, but it was reported that hip extension in the late stance phase of walking exerts a hip flexion moment due to the passive structure of the ligaments around the hip joint. 14 Therefore, it is considered that the increased mobility of hip joint extension has an advantageous effect on hip joint flexion movement during the swing phase.
In particular, in the present study, HAL training contributed not only to improving the mobility of the knee joint but also to increasing the mobility of the hip joint, and it was considered that the effects of the HAL training effect may impact the entire lower limb.
Furthermore, based on the results of the present study, the hip joint extension in the late stance phase was increased to prepare for the forward swing of the lower limbs, and the flexion angle of the knee joint was increased in the swing phase to promote the body forward. In KOA, it has been reported that the knee flexion angle decreases from the late stance to the early swing phase, 15 and it is said that the decrease in flexion mobility after TKA needs to be improved at an early stage. 16 The fact that HAL training improved the mobility of knee flexion suggests that HAL training performed after TKA may improve walking function.
As shown in Table 5, the improvement in step length by HAL training was related to the improvement of knee varus thrust in the early stance phase and the increase in knee joint flexion angle in the swing phase. In addition to postoperative alignment improvement, training by wearing HAL was considered to have promoted pain improvement and increase the knee flexion angle during the swing phase due to increased hip extension mobility and step length.
In contrast, we found no statistical significant difference in the exertion moment of the lower limb joint between the HAL and control groups. Previous reports also showed improvement in quadriceps muscle strength at 8 weeks after surgery, but no significant improvement was observed at 4 weeks after surgery. 11 The weakness of the quadriceps femoris is prominent in KOA. 17 Therefore, after TKA, it takes a lot of time to improve muscle strength, and it is considered important to follow the long-term course in the future.
This study has some limitations. First, the number of patients was small, and the study was limited by its cross-sectional design; therefore, long-term functional improvement after surgery is not fully understood. Second, HAL is only available in a medium size, and the measurement target is limited to patients who can wear HAL. Despite some of the limitations mentioned above, this study suggests that training with HAL from the early postoperative period may contribute to increased mobility of the lower limb joints during walking in patients undergoing TKA.
Conclusion
From the results of this study, it was found that training by wearing HAL after TKA increased the mobility of the knee and hip joints during early postoperative walking, and that walking ability was improved by increasing the step length. In the future, the longitudinal intervention effects of HAL training after TKA should be examined to verify the long-term effects. In addition, future studies need some standardized functional ambulation outcomes and pain scores and not just joint mechanics and stride length as a measure of ambulation outcome.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.