
Abstract
Introduction
Hip fracture is a serious and debilitating condition among older adults. As the general population has aged, the number of hip fractures has increased, and the total number is expected to reach 4.5 million by the year 2050. 1 In Asia, the number of hip fractures and cost of treatment are projected to, respectively, increase from 1,124,060 and US$9.5 billion in 2018 to 2,563,488 and US$15 billion in 2050. 2 Additionally, the number of hip fractures is expected to increase from 18 338 in 2010 to 50 421 in 2035 in Taiwan, 3 inevitably having serious socioeconomic impacts in the near future.
Although evidence has proven that hip fracture repair is effective in facilitating the recovery of mobility and elongating long-term survival periods among elderly patients with hip fracture, 4 surgery-related mortality is an undesirable complication, especially when the patient dies shortly after receiving the operation. The reported in-hospital mortality rate following hip fracture surgery ranges from 2.1% to 2.4%.5,6 Among several prognostic factors associated with postsurgical in-hospital mortality that have been reported in the literature, advanced age has been identified as the most important risk factor in elderly patients with hip fracture.7-9
In clinical practice, for patients and their families, the patient’s advanced age is one of the main factors contributing to the difficulty of deciding whether to opt for surgical repair. Knowledge of potential prognostic factors predictive of a high in-hospital mortality risk following hip fracture repair would enable clinicians to discuss with patients and their families potential fatal complications and alternative choices such as palliative treatment. 10 However, in addition to advanced age, which has been a major research focus, there remains a paucity of available data in the literature regarding other age-independent predictors. 11 The prevalence of in-hospital mortality following hip fracture surgery in older adults is also a topic for which relevant data are insufficient and further investigation is necessary. The aim of the present study was to identify the prevalence of and age-independent risk factors related to in-hospital mortality in vulnerable elderly patients following hip fracture repair.
Material and Methods
Study Population
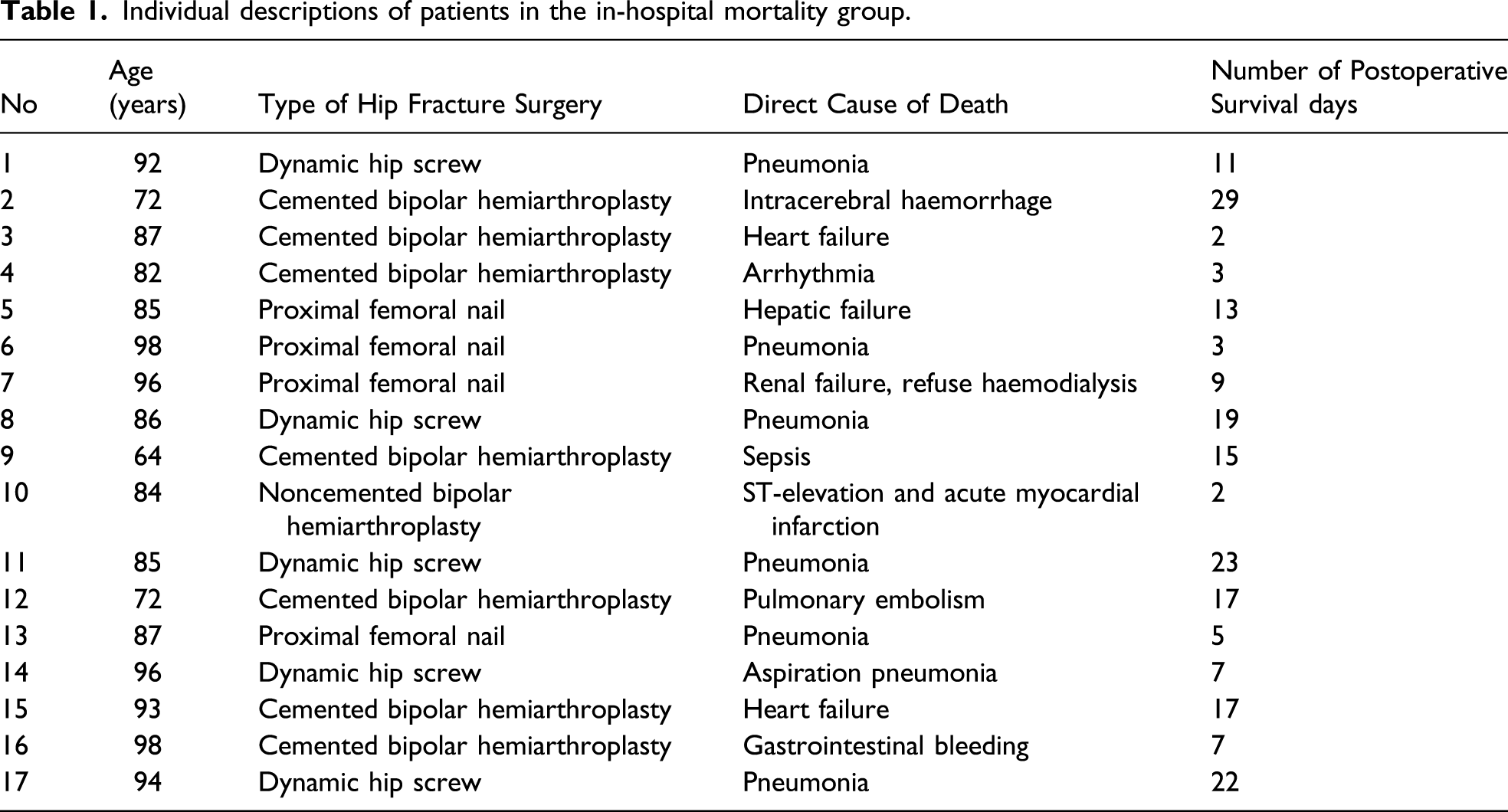
This retrospective review included 842 patients older than 60 years who had been diagnosed as having extracapsular or intracapsular proximal femur fracture and who had received operations that included hemiarthroplasty or internal fixation with intramedullary nails, in situ cannulated screws, or dynamic hip screws at our institution in Taipei, Taiwan from January 2016 to August 2020. Patients were excluded if they received hip surgery for a condition other than primary hip fracture, such as for osteoarthritis, trauma, tumour metastasis, infection, or avascular necrosis of the femoral head. Among the 842 elderly patients with hip fracture, 17 died during their hospital stay after receiving hip fracture surgery, yielding an overall postsurgical in-hospital mortality rate of 2.0%.
This case–control study was conducted to compare the two age-matched groups of elderly patients with equivalent age but with different survival outcomes after hip surgery (ie, members of the in-hospital mortality group were compared with aged-matched members of the survival group, who lived for more than 3 months after discharge). Because advanced age has been regarded as one of the most critical factors influencing a patient’s prognosis, we paired the two groups by age to examine other potential age-independent clinical factors that may also greatly affect short-term outcomes of older adults with hip fracture. A 1:3 ratio was adopted, meaning that each participant in the in-hospital mortality group was paired by age to 3 other older adults with hip fracture who had survived for more than 3 months following surgery. Participants in the survival group were selected from our previously established databank for patients older than 60 years who underwent hip fracture repair at the same institution and with the same experienced orthopaedics team. 12
Measurement of Clinical Parameters
Basic demographic data, including age, sex, body mass index (BMI) and underlying comorbidities, were collected, along with laboratory data such as sodium level and preoperative and postoperative haemoglobin and creatinine levels and platelet and white blood cell counts. We also recorded the specific amount of time that elapsed between a patient’s fall and the time of operation. The operation records of each patient were screened to extract the following associated information: type of hip fracture, fracture location, blood loss during the operation, type of anesthesia, and duration of the operation.
Statistics
All statistical analyses were conducted using SPSS Statistics for Windows, version 18.0 (SPSS Inc., Chicago, IL, USA). Categorical variables are presented as frequencies and percentages, and continuous variables are presented as means ± standard deviations. Univariate analyses were conducted on risk factors that may be associated with in-hospital mortality in patients with hip fracture. Chi-squared and independent Student’s t tests were performed to compare categorical variables and continuous variables, respectively. Factors that differed significantly (P < .05) in the univariate analysis were included in the binary multivariate logistic regression model to estimate the odds ratios (ORs) with 95% confidence intervals (CIs). A receiver operating characteristic (ROC) curve was drawn for each significant risk factor in the binary multivariate logistic regression model. The area under the curve (AUC) was used to quantify the discriminative power of the ROC curve, and the Youden index was applied to identify the best cut-off point. For all tests, a two-sided P value of <.05 was considered statistically significant.
Results
Individual descriptions of patients in the in-hospital mortality group.
Comparison of clinical characteristics between groups of patients with hip fracture.

*eGFR was chosen into the binary multivariate logistic regression model instead of serum creatinine.
Abbreviations: BMI, body mass index; eGFR, estimated glomerular filtration rate; SD = standard deviation; WBC = white blood cell
Basic clinical characteristics of these 2 cohorts are listed in Table 2. The two groups did not differ significantly in terms of sex, BMI, laboratory parameters, residence type, type of hip fracture and fracture location. The results of the univariate analysis revealed significant between-group differences in the amount of time between the time of the fall to the time of operation, the type of anaesthesia used, the estimated glomerular filtration rate (eGFR), the proportion of patients with type 2 diabetes mellitus (DM), the proportion of patients with hepatitis and history of malignant cancer. Therefore, these 6 factors were included in the binary logistic multivariate regression model for further analysis.
Second binary multivariate logistic regression model for the estimation of in-hospital mortality risk factors.

Abbreviations: CI, confidence interval; DM, type 2 diabetes mellitus; eGFR, estimated glomerular filtration rate.

Receiver operating characteristic (ROC) curve and area under curve (AUC) of (A) estimated glomerular filtration rate, (B) malignant cancer, and (C) diabetes mellitus.
Discussion
In the present study, each patient’s clinical history was thoroughly reviewed, and all serum samples were obtained within 24 h after admission, thus ensuring the comprehensiveness and reliability of the data. After patients were cross-matched by age, our results suggested that eGFR, DM and history of malignant cancer were the three most important age-independent risk factors predictive of the postoperative prognosis of older adults with hip fracture.
The long-term mortality rate following hip fracture surgery is high. A Korean nationwide retrospective study reported that the mortality rate of patients with hip fracture was twice as high as that of the general population at a mean follow-up period of 4.45 years. 13 However, in-hospital mortality after hip fracture surgery is rare and could result in a considerable psychological burden for orthopaedic surgeons and the patient’s family. Studies have reported that 2.1% to 2.4% of patients with hip fracture die during hospitalisation,5,6 which is comparable to the results of the present study. Male gender, the use of conservative treatment, advanced age and the presence of comorbid conditions on admission were identified as significant risk factors for in-hospital mortality in patients with hip fracture.7,14 Moreover, a UK study compared patients who died within 48 h after hip fracture surgery with those who survived more than 1 year after hip fracture surgery and found that the former were older and more likely to be receiving institutional care or to have fallen in the hospital. An American Society of Anesthesiologists physical classification system grade higher than 3, mental impairment and impaired mobility were also highly related to 48 h postoperative mortality. 11
Kidney function is a key factor in determining the long-term outcomes of patients with hip fracture. In a large population-based cohort study of 44 065 diabetic patients with different stages of renal function after hip fracture surgery, patients undergoing dialysis had the highest rates of mortality and short‐ and long‐term complications at 3 months and 1 year after surgery, followed by patients with chronic kidney disease (CKD) and those without CKD. 15 Patients with CKD were reported to have a high risk of malnutrition, anaemia and electrolyte imbalances; in particular, they had problems with calcium metabolism that disrupted bone remodelling and mineralisation (renal osteodystrophy). 16 Moreover, receiving dialysis is commonly associatedwith increased production of inflammatory cytokines and functional defects in the immune system, thus putting patients at an increased risk of infection.17,18 A Korean retrospective study categorised 119 patients with hip fracture into CKD and non-CKD groups and found that the CKD group had a significantly lower 5-year survival rate than that of the non-CKD group; moreover, 27% of patients in the CKD group experienced complications, whereas complications were reported in only 11.9% of patients in the non-CKD group. Infections and prosthesis dislocation were the two most common postoperative complications reported in the CKD group. 19 In the present study, the 77% of patients who died during their hospital stay had different stages of CKD, and nearly half of them died of pneumonia. This finding suggests that a more thorough preoperative risk assessment should be applied, along with intensive postoperative care. 20
A strength of the present study was that the timing of each hip fracture occurrence was reported by patients or their caregivers rather than being extracted from their admission or emergency records. Although the time between fracture occurrence and surgery was not significant in the binary logistic multivariate regression model, it was still a factor that potentially affected the likelihood of survival after hip fracture. Multiple studies have investigated matters related to surgery delay in patients with hip fracture. A Norwegian observational study of 83 727 patients with hip fracture found no differences in mortality if the fracture-to-surgery time was within 48 h; however, 3-day and 1-year postoperative mortality rates increased significantly when the fracture-to-surgery time exceeded 48 h. 21 Another large observational study reported that mortality increased significantly with increasing time between fracture occurrence and surgery. 22 Moreover, Fu et al. reported that performing surgery on patients with hip fracture within 24 h after admission could significantly reduce the risk of respiratory complications, including pneumonia, extubation failure and reintubation. 23 However, a recent randomised controlled trial reported no significance differences regarding mortality or major complications between patients who received accelerated surgery and those who received standard care. We posit that this between-study discrepancy could be the result of different fracture-to-surgery times; all patients in the randomised controlled trial received surgery within 48 h after hip fracture occurrence, 24 whereas other studies included patients who had longer fracture-to-surgery times. In the present study, the average fracture-to-surgery time in the in-hospital mortality group exceeded 4 days. Although we did not record the exact reasons for these delays, we suspect that the serious comorbidities in these patients interfered with hospital transportation, the decision to operate and the creation of plans for anaesthesia.
Types of anaesthesia differed between in-hospital mortality and control groups in the univariate analysis. Compared with the control group, the in-hospital mortality group included more patients who received general anaesthesia through endotracheal tube intubation and fewer patients who received epidural anaesthesia. Waesberghe et al. performed a meta-analysis and examined the outcomes of general and neuraxial (spinal and epidural) anaesthesia in patients with hip fracture and identified significantly lower rates of in-hospital mortality among the neuraxial anaesthesia group (OR .85, P = .004) but no difference in 30-day mortality rate between patients who received these two types of anaesthesia. 25 Moreover, two other retrospective cohort studies that focused on older adults with hip fracture also reported no difference in 30-day mortality rates between these two types of anaesthesia,26,27 and another study reported that spinal anaesthesia was associated with fewer and less severe adverse effects. 27 In fact, an increased use of spinal anaesthesia over general anaesthesia in older adults with hip fracture has already been observed, which may be attributable to lower interventional morbidity in older patients with frailty. 28
Several in-hospital mortality prediction models for patients with hip fracture have been proposed, but no reliable prediction model has been well documented. Karres et al. applied six prediction models to 1050 patients with hip fracture, and none of the models yielded convincing discrimination in predicting 30-day mortality. 29 Similarly, Nelson et al. directly compared three well-known predictive models for mortality in elderly patients following hip fracture: the Age-Adjusted Charlson Comorbidity Index, 30 the Physiological and Operative Severity Score for enUmeration of Mortality and Morbidity 31 and the Nottingham Hip Fracture Score. 9 Using acceptable AUC values, the authors concluded that these three models did not differ significantly in mortality prediction accuracy. 32 Future studies with larger sample sizes are warranted to establish an optimal scoring system for predicting short-term mortality in older adults with hip fracture. The three age-independent risk factors identified in the present study could nevertheless aid clinicians’ decision-making regarding hip fracture surgery for older adults.
Limitations
This study had several limitations. First, only 68 participants were retrospectively enrolled; thus, the study findings cannot represent the overall condition of older adults with hip fracture. Second, this study was conducted in the Taipei City metropolitan area, meaning that the findings may not be representative of the epidemiology of hip fracture among residents of urban areas in Taiwan. Third, limitations inherent in the retrospective investigation of medical records prevented us from being able to collect several important clinical parameters that may be highly correlated with in-hospital mortality, such as mental condition, preinjury mobility status and the use of medication. Additional studies with larger sample sizes are warranted to follow the natural course and assess the clinical effect of these risk factors in older adults shortly after they receive hip fracture surgery.
Conclusion
This case–control study identified poor renal function, malignant cancer history, and DM as three significant age-independent risk factors for in-hospital mortality in older adults undergoing hip fracture surgery. Renal function had an acceptable AUC value; when eGFR <35 mL/min/1.73 m2 was set as the cut-off point, patients vulnerable to in-hospital mortality following hip fracture surgery could be identified with high sensitivity.
Footnotes
Acknowledgements
The authors are grateful to like to acknowledge the Laboratory Animal Center at TMU for the English editing support and to Taipei Medical University (Grant numbers TMU110-AE1-B07) for financially supporting this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Taipei Medical University (Grant numbers TMU110-AE1-B07).
Ethical Approval
The Ethical Committee of Taipei Medical University approved the entire protocol and all instruments used (ethical approval number: TMU-JIRB N201709053). All participants consented to their inclusion in the study and the publication of data.