
Abstract
Keywords
Introduction
Fractures of the distal radius tend to be the first fragility fracture among those caused by osteoporosis. Distal metaphyseal ulnar fractures often occur in conjunction with distal radius fractures, especially in elderly patients. Distal radius fractures are often associated with ulnar styloid fractures and less frequently with distal metaphyseal ulnar fractures. In metaphyseal cases, distal radius fractures are usually fixed, 1 but there is no consensus on the optimal management of the concomitant distal ulnar fractures. Several surgical treatment methods have been reported for distal metaphyseal ulnar fractures accompanied by distal radius fractures, such as the conventional plate, 2 locking plate,3,4 hook plate,5-7 intramedullary device,8,9 and primary resection. 10 Fixation of distal metaphyseal ulnar fractures can be challenging, 11 and several studies have shown the validity of conservative treatment alternatives.12-17 If clinical outcomes of the conservative treatment for distal metaphyseal ulnar fractures accompanying distal radius fractures are the same when compared with those of surgical fixation, there is a possibility that unnecessary surgery can be avoided. This study aimed to determine whether simultaneous fixation of both distal radius and distal metaphyseal ulnar fractures would improve treatment outcomes.
Materials and Methods
Study Design
This was a retrospective cohort study conducted among patients with distal radius fractures at a single center, based on the data extracted from the medical records. We compared patient clinical outcomes between two groups categorized based on their management: either operative or conservative. The study conforms to the principles laid down in the Declaration of Helsinki and its amendments. Informed consent, both written and verbal, was obtained from all patients for treatment and publication. This study was approved by the institutional review board of our institute (Teikyo University Ethical Review Board for Medical and Health Research Involving Human Subjects 17-057).
Study Setting
The study was conducted at the Trauma and Reconstruction Center of Teikyo University Hospital in Tokyo, Japan. All patients with trauma leading to orthopedic issues are managed at our center.
Participants
This study included patients with distal radius fractures who were treated surgically over a 4-year period at our trauma center.
Outcomes
The primary outcome was upper extremity disability, evaluated using the quick Disabilities of the Arm, Shoulder, and Hand (quick DASH) score. 18 Higher scores indicated additional disabilities. The secondary outcomes were range of motion and grip strength (physical findings evaluated and recorded by the physicians) and the ulnar variance compared to the healthy side and bone union (radiographic findings evaluated by the first author). The outcomes were evaluated at the time of the final follow-up. The final follow-up was conducted on the day the attending physician considered the patient to be healed.
Variables
Patients were categorized into two groups based on the treatment type. Data were collected from medical records and radiographic findings. In one group, distal metaphyseal ulnar fractures were treated using surgical fixation with a plate, screws, and wires; in the other group, fractures were managed conservatively. The following data were also extracted: patient demographic details, mechanism of injury, whether the fracture was closed or open, Gustilo classification, 19 AO/OTA classification, 20 immobilization period, and follow-up period.
Statistical Analysis
Data are expressed as means with standard deviations (mean ± SDs). Continuous variables were evaluated using the t-test, and nominal variables were evaluated using Fisher’s exact test. For the comparison of the nominal variables among the two groups, the chi-square test was used. Statistical significance was set at p-values <0.05. All statistical tests were performed using JMP software (version 9.0.2; SAS Institute, Cary, North Carolina, United States).
Results
Patient Characteristics
Of the 171 distal radius fractures treated during the specified period, 98 patients had ulnar fractures associated with distal radius fractures. Ulnar styloid fractures with distal radial fractures (62 cases) were excluded. We also excluded patients with <12 months of follow-up (n = 4), no displacement of the ulna (n = 3), ipsilateral upper extremity injury (n = 2), and contralateral upper extremity injury (n = 4). The remaining 23 patients were included in this study (Figure 1). Flow diagram of the study design.
Summary of Patients’ Characteristics.

Outcomes
Outcome Evaluation and Statistical Analysis.
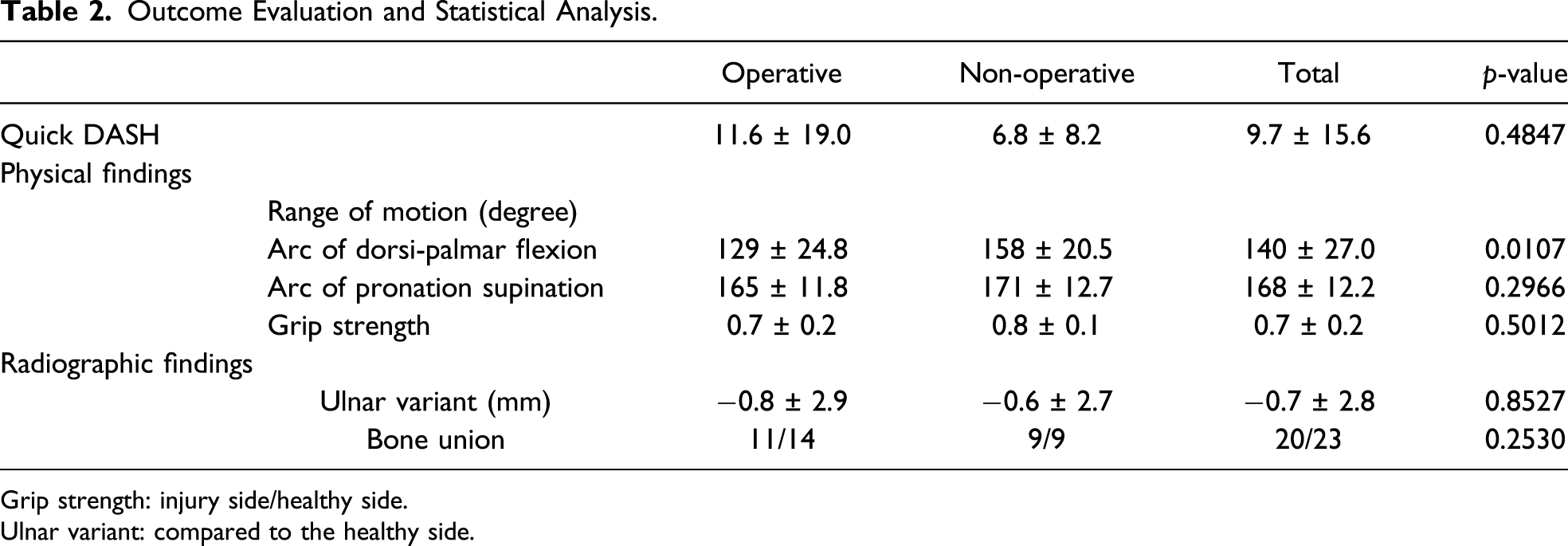
Grip strength: injury side/healthy side.
Ulnar variant: compared to the healthy side.
Discussion
We conducted a rtetrospective cohort study among patients with distal radius fractures in a single center based on data obtained from our medical records. This study determined whether simultaneous fixation of both distal radius and ulnar fractures improved the treatment outcomes. While the quick DASH scores were not significantly different between the two groups, the arc of dorsi-palmar flexion was significantly more restricted in the operative group than in the conservative group. Radiographic findings were not remarkably different between the two groups, except for three cases of non-union of the ulna that required surgery. We wondered if the severity of the open fracture, the type of fracture of the radius, or the type of fracture of the ulna had an effect, but there did not seem to be a significant difference between the two groups (Table 1). There is no clear evidence that the ulnar fixation techniques affect the arc of dorsi-palmar flexion, but at least if the results are comparable, it may not be necessary to add surgical intervention. Thus, the simultaneous fixation of both distal radius and ulnar fractures did not improve the treatment outcomes; we can conclude that distal metaphyseal ulnar fractures can be managed conservatively.
Fixation of distal metaphyseal ulnar fractures can be challenging because of comminuted fractures causing difficulties in reduction, osteopenia, or concerns of hardware impingement on the thin, soft tissue envelope. Additionally, a triangular cross-sectional shape of the bone at the subcutaneous border of the ulna can lead to hardware prominence and necessitate implant removal. 11 Interestingly, 78% of fractures were open, and these wounds were located mainly on the ulnar side in our series. All open fractures were classified into Gustilo type I-IIIa, and primary skin closure was possible. However, in some cases, there were some compromised skin conditions at the open fracture site.
Several studies have shown the validity of conservative treatment.12-17 Namba et al. described a technique wherein the distal radial fractures were securely fixed with a palmar plate, leaving the associated ulnar fractures unfixed. 12 Fourteen patients with a mean age of 74 years were treated and followed up at approximately 18 months after surgery. The results were excellent in 11 cases and good in three, and all fracture sites had displayed union, with no instability of the distal radioulnar joint. A widening of the distal radioulnar joint space was present in one patient. Angular deformity of the distal ulnar metaphysis was seen in five wrists. It was concluded that this treatment could be an alternative to open reduction with internal fixation for intra-articular distal ulnar fractures in older adults. 12
Cha et al. also reported their findings from a prospective case–control study of two treatment methods for unstable distal ulnar fractures associated with distal radius fractures in patients over 65 years of age. 13 The first 29 ulnas were treated surgically, and the next 32 ulnas were treated conservatively. All radial fractures were fixed internally in both groups, and clinical and radiological outcomes were evaluated. The mean duration at the final follow-up was 34 months. There were no significant differences in the clinical and radiological outcomes, including ulnar variance and union rate, between the two groups. No participants from either group demonstrated symptomatic arthritic changes in the radiocarpal joint or distal radioulnar joint at the final follow-up. Thus, in this population, distal ulnar fractures can be successfully managed conservatively when they occur in combination with distal radius fractures.
Liang et al. reported that the stability of the distal forearm afforded by soft tissue stabilizers, namely, the triangular fibrocartilage complex (TFCC) and the distal oblique band (DOB) of the interosseous membrane, was a key consideration in the management of concurrent distal radius and ulna fractures. 14 With adequate reduction of the distal radius, the structural integrity between the DOB and TFCC is restored. They postulated that this is a crucial factor in maintaining the distal ulnar metaphyseal and articular fracture reduction. This supports the view that if the distal radius fracture is anatomically and rigidly fixed, distal ulnar fractures can be successfully managed conservatively.
Several issues remain to be addressed regarding the age of the patients. Özkan et al. reviewed the management of ulnar neck fractures associated with fractures of the distal radius. 15 They used a large database to study the incidence of unplanned surgeries after surgical and nonsurgical treatment of distal metaphyseal ulnar fractures associated with a distal radius fracture and identified factors associated with these unplanned surgeries. They identified 277 patients with an ulnar neck fracture associated with a distal radius fracture. Fifty-six (20%) ulnar neck fractures were initially treated operatively, and six of them (11%) had a second, unplanned surgery. Of the 221 conservatively treated fractures, only one (0.45%) had a subsequent unplanned surgery that seemed unrelated to the fracture. Bivariate analysis showed that younger age, open fracture, multi-fragmented fractures, and initial operative treatment of the ulnar neck fracture were significant risk factors for subsequent unplanned surgery.
Lutsky et al. concluded that routine surgical fixation of concomitant distal ulnar fractures during distal radius surgery using the open reduction internal fixation technique does not appear to be necessary. However, they noted that the limitation of their study was that it included a wide range of patient ages (range: 19–97 years). 16 Sato et al. evaluated all cases except in those younger than 60 years and concluded that the results of treating combined distal radius and ulnar fractures in older people using volar locking plate fixation for the distal radius fracture and leaving the distal ulnar fracture unfixed were encouraging. 17
The limitations of our study include the following: a high percentage of patients enrolled were older, the study is retrospective in nature, and the interventions and period of immobilization were determined individually by surgeons. Our study may be a comparison of two different treatments chosen by surgeons for similar injuries. Unfortunately, the current classification system alone does not take into account the degree of displacement. Moreover, only a small number of patients were included in the study. In AO C3 distal radius fractures or open fracture cases, soft tissue defect and periosteal stripping could affect the functional result and bone healing; therefore, we could not discuss those elements separately. Large-scale prospective studies will be required in the future to corroborate the findings of our study.
Conclusion
Our results did not show any merit of simultaneous fixation of both distal radius and distal metaphyseal ulnar fractures. This study supports the view that distal metaphyseal ulnar fractures associated with distal radius fractures can be managed conservatively, especially in elderly patients. However, further studies are required to provide evidence as to whether fixation of distal metaphyseal ulnar fractures can be avoided.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.