
Abstract
Introduction:
Evidence suggests that the distal radioulnar joint injury associated with an operatively treated displaced fracture of the distal radius does not benefit from specific treatment after the radius is realigned. To better understand variation in treatment of the distal radioulnar joint we performed a scenario-based experiment presenting radiographs of displaced distal radial fractures accompanied by clinical scenarios with randomized aspects.
Methods:
In a survey-based experiment, participants of the Science of Variation Group viewed a random subset of five of 10 sets of radiographs showing displaced fractures of the distal radius before and after anterior plate fixation. Each was accompanied by a clinical scenario with trauma energy level, age and gender randomized. Participants indicated their preferred distal radioulnar joint treatment: none, cast immobilization, operative reattachment of ligaments or ulnar styloid fixation, or distal radioulnar joint pinning. Factors associated with any treatment and with reattachment were sought in multivariable regression.
Results:
Surgeons recommended distal radioulnar joint treatment in 67% (404 of 607) of the scenarios, most commonly cast immobilization in 41% (247 of 607). Recommendation for any distal radioulnar joint treatment was associated with younger patient age, and for reattachment specifically, was associated with younger patient age, high-energy trauma and fracture of the base of the ulnar styloid.
Conclusions:
The observation of frequent recommendation for distal radioulnar joint treatment, relatively more so for younger patients with higher energy injuries, and some tendency to repair an aligned ulnar styloid base fracture may diverge from existing evidence.
Introduction
A distal radial fracture (DRF) that is sufficiently displaced is likely to disrupt the distal radioulnar joint (DRUJ) ligaments (part of the triangular fibrocartilage complex, TFCC) through either avulsion of their origin or fracture of the base of the ulnar styloid (Ramponi et al., 2022). Several randomized trials demonstrate no benefit to wrist immobilization of any duration after anterior plate fixation of a fracture of the distal radius (Deng et al., 2021; Lozano-Calderón et al., 2008; Quadlbauer et al., 2017, 2022; Souer et al., 2011). A systematic review of 12 studies and 2243 patients with displaced DRFs, both operatively and non-operatively treated, found similar levels of discomfort and incapability and similar assessments of DRUJ stability with or without a concomitant non-operatively treated ulnar styloid base fracture (Mulders et al., 2018).
Nevertheless, some surgeons may contend that measurable ‘instability’ with a ballottement test/piano key manoeuvre after fixation of the radius (Fricker et al., 2015; Johandi and Sechachalam, 2017) or arthroscopic identification of avulsion of the origin of the DRUJ ligaments (part of the TFCC) (Lindau et al., 2000; Mrkonjic et al., 2012) merits specific treatment. Basing treatment decisions on intraoperative assessments of DRUJ stability is inconsistent with the evidence that tests of DRUJ stability are unreliable (Giddins et al., 2025; Pickering et al., 2022). Initial laxity is to be expected, but addressing the DRUJ ligaments is not associated with differences in final levels of discomfort and incapability (Bakker et al., 2023; Miller et al., 2018; Schmitt et al., 2023).
A scenario-based experiment, where surgeons are presented with radiographs and randomized age, gender and energy of injury, can be an efficient and practical way to measure factors associated with variation in treatment of the DRUJ associated with DRFs among a large group of fully trained surgeons. This experiment generates associations rather than rates or rating, an approach that should lead to reproducible findings as long as there is sufficient variation in surgeon opinion. We asked: (1) are there any patient factors associated with surgeon recommendation for any treatment of the distal radioulnar joint after anterior plate fixation of a DRF; and (2) are there any patient factors associated with surgeon recommendation for reattachment of the origin of the DRUJ ligaments/open reduction and internal fixation (ORIF) of an ulnar styloid base fracture either open or arthroscopic after anterior plate fixation of a DRF?
Methods
Study design and setting
We obtained approval from the institutional review board to conduct this online survey and scenario-based experiment. Members of the Science of Variation Group (SOVG) were invited to complete an online survey (Qualtrics, Provo, Utah, USA) by e-mail with an initial request and two weekly reminders between February and March 2025. Participation in the survey was accepted as informed consent. The vast majority of surgeons on the SOVG e-mail list treat fractures of the distal radius. Surgeons who do not treat distal radial fractures were asked not to participate. The SOVG is an international consortium of musculoskeletal surgeons who study sources of variation in visits, diagnoses, classifications, tests and treatments. The participants to date are mostly White American and European men involved in academic care, but all musculoskeletal surgeons are welcome. The rates and ratings may not be reproducible in other settings, but the associations are likely to be reproducible in any sample with sufficient variation in opinion. There is no financial incentive to participate.
The survey consisted of five scenarios, paired randomly with one of ten sets of radiographs, including pre-reduction, post-reduction and post-anterior plate fixation posteroanterior and lateral radiographs of the wrist (Online Appendix 1). All radiographs were carefully selected to be compatible with all possible combinations. After selection, the survey was checked several times for strange combinations. Ten fractures were selected from a previous randomized trial with a separate IRB approval allowing secondary use of the material obtained. The ten fractures were selected by one researcher in chronological order with the following criteria: (1) dorsally displaced fracture; (2) treated with an anterior locking plate and (3) a complete set of pre-reduction, post-reduction and post-operative radiographs available. Three fractures of the initial set were excluded because of limited displacement and a debatable indication for surgery, and were replaced. One senior author confirmed the selection and quality of the final set of radiographs. To attempt to provide a representative spectrum of injuries, we chose ten fractures in consecutive order of treatment that met the inclusion and exclusion criteria. All identifying information was removed from the images. Accompanying each set of radiographs was a scenario including randomized gender (man/woman), age 18–89 years and energy of trauma (low/high). The scenario also stated, ‘You notice DRUJ laxity slightly greater than the uninjured wrist on intra-operative examination.’ This resulted in a large number of unique scenarios, each randomly associated with a set of radiographs. Each participant only viewed five of the ten radiographs, each paired with a unique, randomized scenario. The experiment depends on variation, and part of the variation (an explanatory variable) is the specific fracture (radiographs). This allows us to measure if specific radiographic features are associated with specialist recommendations.
Participants
Among the approximately 200 members of the SOVG who participate in at least one experiment a year, 142 (71%) surgeons started the survey and 127 (64%) surgeons completed at least one scenario as required for inclusion of their data. Eleven participants did not complete all five scenarios, accounting for 23 missing scenarios. Given the randomized nature of the experiment, any completed scenario could be analysed. We analysed 127 participants and 612 scenarios. Most participants were men (91%; 116 of 127), located in the USA (54%; 69 of 127), had initiated an independent practice before 2000 (40%; 51 of 127), had supervised trainees (76%; 97 of 127) and were orthopaedic surgeons (85%; 108 of 127) (Table 1).
Demographics of 127 surgeon participants.*
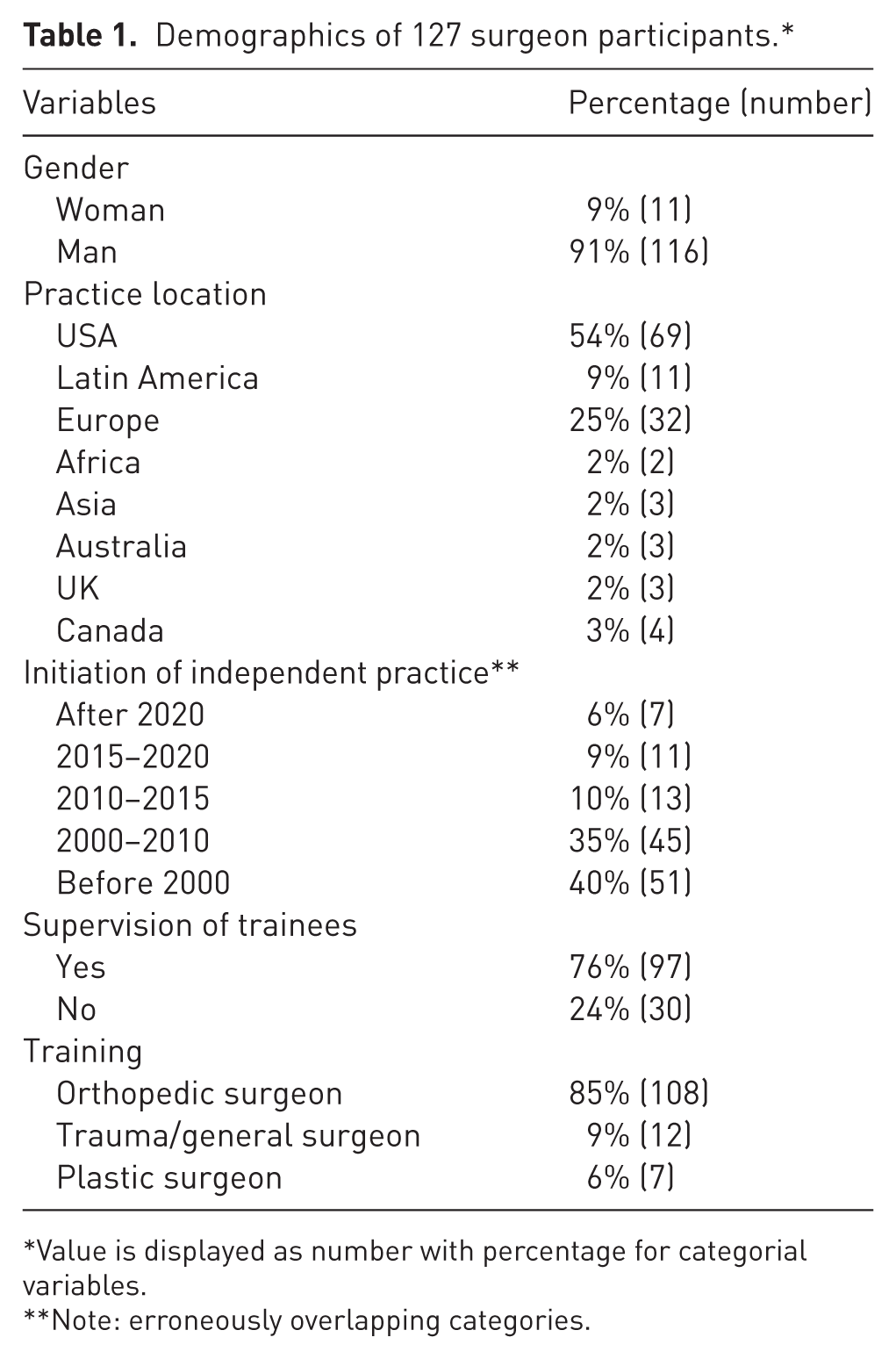
Value is displayed as number with percentage for categorial variables.
Note: erroneously overlapping categories.
Response variables
After reading the scenario and reviewing the radiographs, each participant selected one of four treatment options for the DRUJ component of the injury (often referred to as the TFCC): (1) temporary cast immobilization of the forearm (type of cast not specified); (2) reattachment of the origin of the DRUJ ligaments or ORIF ulnar styloid base fracture either open or arthroscopic; (3) temporary rigid DRUJ immobilization by pinning the ulna to the radius; or (4) no additional treatment. Our primary outcome was any DRUJ treatment compared to no treatment, and secondary outcome was reattachment of the DRUJ ligament origin or ORIF of the ulnar styloid base fracture, or not.
Explanatory variables
The explanatory variables were patient age randomized from 18 to 89 years, low or high level of trauma energy and gender (man or woman).
Statistical analysis
Descriptive statistics were performed for available surgeon characteristics and elements of the patient scenarios. Categorical variables were presented as a percentage with frequency and continuous variables were reported as a mean with standard deviation or a median with interquartile range dependent on data distribution. Data distribution was assessed using visual interpretation of histograms and Shapiro–Wilk tests.
We sought patient factors associated with surgeon recommendation for any treatment and reattachment of DRUJ using multilevel mixed-effects logistic regression models, accounting for nesting by surgeon. We also used Fisher’s exact and chi-squared tests to assess the proportional differences in surgeon recommendation for any treatment and reattachment for each presented set of radiographs. We did not seek surgeon factors associated with any treatment or reattachment because we noted that we often got misleading results owing to small and unrepresentative subsets of specialists. Additionally, we did not calculate a priori sample size owing to the fact that we cannot control participation in SOVG studies. All p-values below 0.05 were considered statistically significant.
Results
Accounting for potential confounders including patient factors and nesting by surgeon, we found that lower surgeon-rated likelihood of recommending any treatment of the DRUJ after anterior plate fixation of a DRF was slightly associated with older patient age (odds ratio (OR) = 0.95, 95% CI 0.93 to 0.97, p < 0.001), but not with presence of ulnar styloid base fracture, trauma energy level or gender (Table 2). Among the complete set of rated scenarios, 69 surgeons (54%) recommended an additional treatment of the DRUJ at least once, of which 48 surgeons (38%) always recommended additional treatment (in all scenarios). Some form of DRUJ treatment was recommended in 67% (404 of 607) of the scenarios. Surgeons mostly recommended cast immobilization 41% (247 of 607) (Table 3).
Multivariable analysis of randomized scenario factors associated with any treatment.
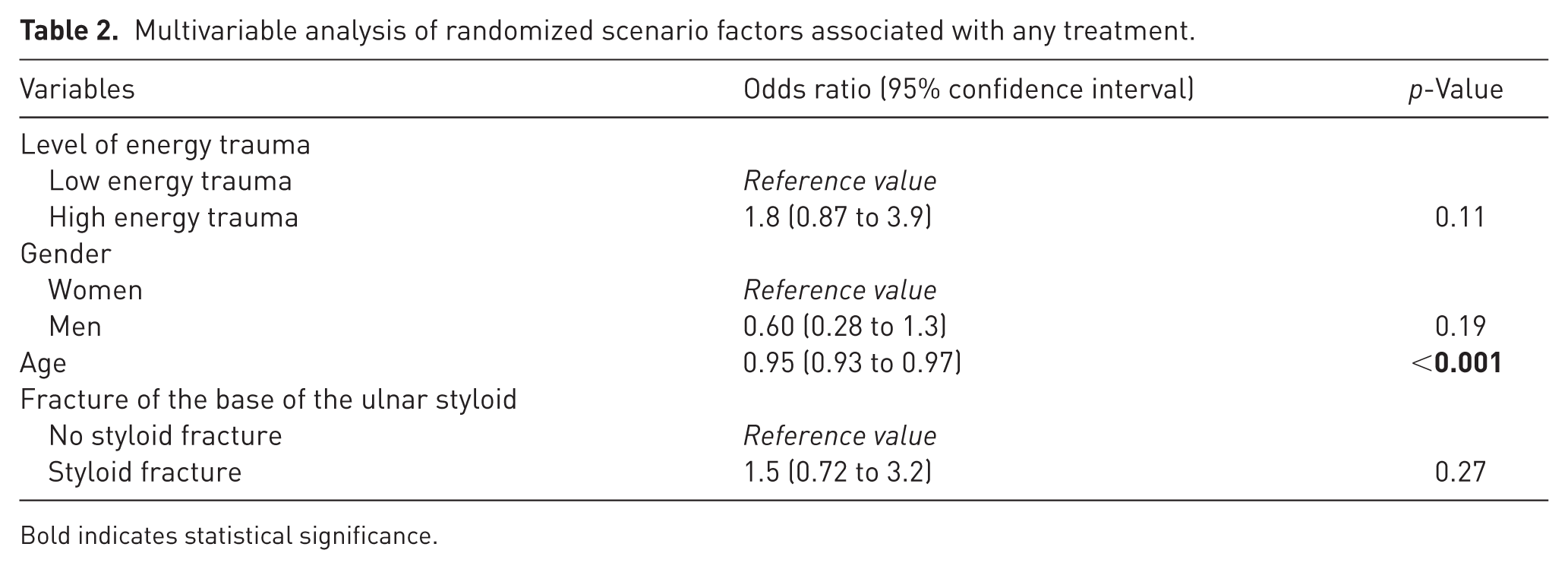
Bold indicates statistical significance.
Distribution of treatment choices per radiograph.
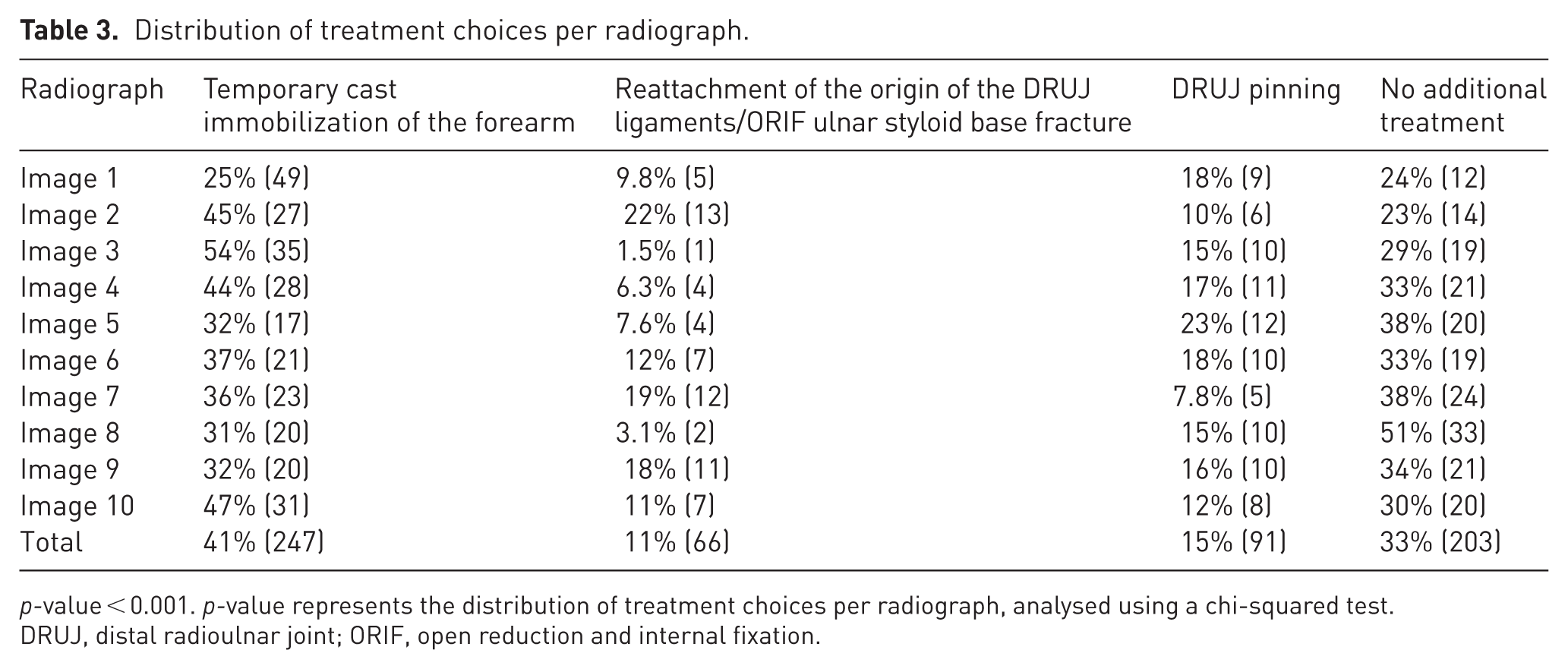
p-value < 0.001. p-value represents the distribution of treatment choices per radiograph, analysed using a chi-squared test.
DRUJ, distal radioulnar joint; ORIF, open reduction and internal fixation.
Accounting for potential confounders including patient factors and nesting by surgeon, we found that higher surgeon rated likelihood to recommend reattachment of DRUJ ligaments or ORIF of ulnar styloid base fracture was substantially associated with fracture of the base of the ulnar styloid (OR = 16, 95% CI 4.6 to 59, p < 0.001), strongly associated with high energy trauma (OR = 3.7, 95% CI 1.2 to 12, p = 0.03), and slightly associated with younger age (OR = 0.97, 95% CI 0.93 to 1.0, p = 0.044) (Table S1). Forty-four surgeons (35%) recommended reattachment of the origin of the DRUJ ligaments or ORIF of an ulnar styloid base fracture at least once, of which only two surgeons (1.6%) recommended reattachment in all scenarios. In total, reattachment of DRUJ ligaments or ORIF of ulnar styloid base fracture was recommended in 11% (67 out of 607) of the scenarios regardless of the randomized elements (Table 4).
Distribution of reattachment of the ulnar styloid choices per patient.
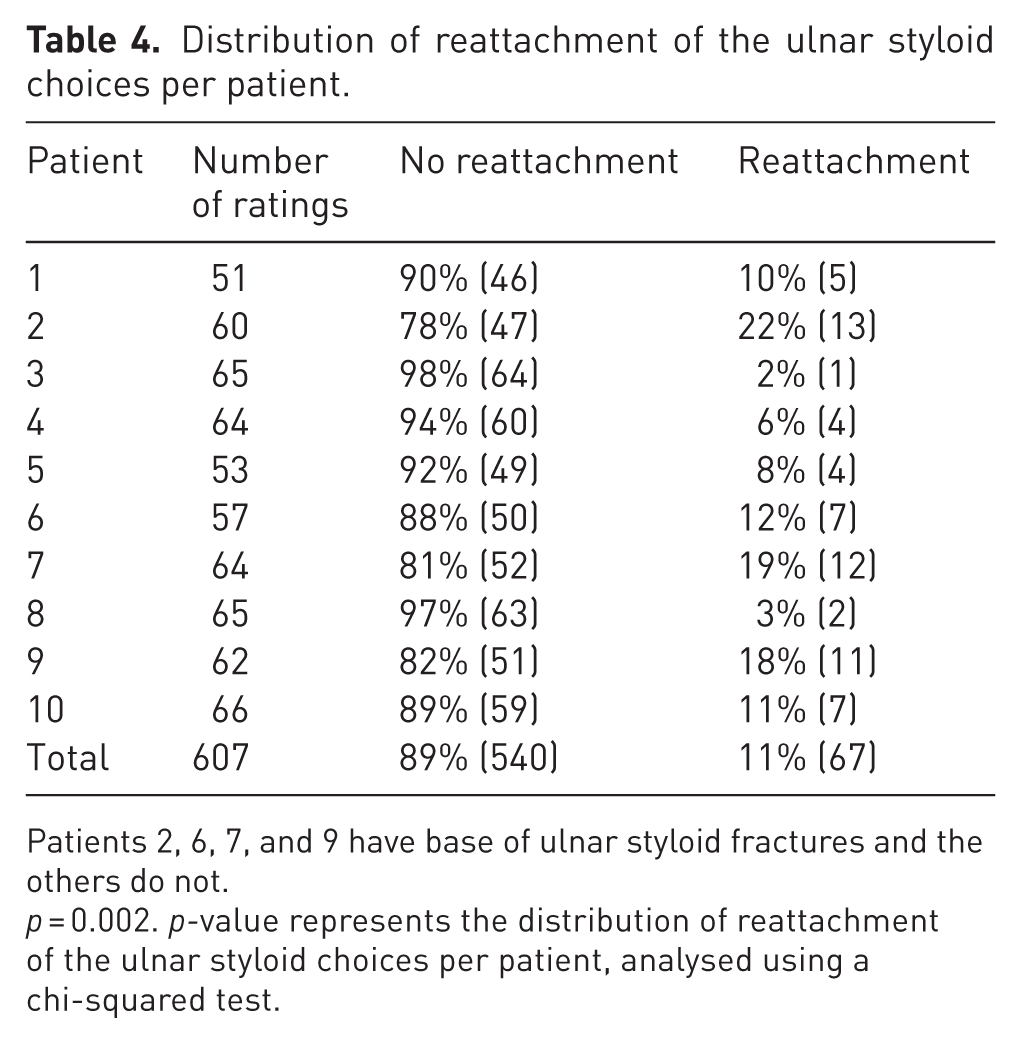
Patients 2, 6, 7, and 9 have base of ulnar styloid fractures and the others do not.
p = 0.002. p-value represents the distribution of reattachment of the ulnar styloid choices per patient, analysed using a chi-squared test.
Discussion
Available evidence suggests that, although a sufficiently displaced DRF probably ruptures the origin of the volar and dorsal DRUJ ligaments (the key stabilizing structures of the TFCC) or fractures the base of the ulnar styloid from which those ligaments originate, there is no benefit to specific treatment of the DRUJ when the DRF is well aligned and stabilized (Bakker et al., 2023; Mulders et al., 2018; Xiao et al., 2021). It is unclear how well this evidence has been implemented into daily practice. We studied the prevalence of specific treatment of the DRUJ associated with a displaced DRF and found that participating surgeons often recommend additional treatment of the DRUJ (67%; mostly cast immobilization), more so with younger patients, high-energy trauma and fracture of the base of the ulnar styloid.
This study can be considered in light of some limitations. First, members of the Science of Variation Group are not representative of the regular surgeon population (for instance,76% supervise trainees). It is mostly composed of white, male, academic surgeons located in Europe and the USA. This subset of surgeons might be expected to be relatively aware of current evidence and practising in line with it. The rates of specific recommendations are probably not reproducible in other samples, but the associations may be. Second, the awareness of being studied (Hawthorne effect) might have influenced the results. There is, however, evidence that the Hawthorne effect does not preclude the ability of experiments to measure relevant associations (McCambridge et al., 2014). Third, there are inherent limitations to online, scenario-based experiments compared with real-life situations, including practice-related stressors and interpersonal interactions. It is possible that the level of variation would be greater in the care of patients.
Fourth, participants viewed radiographs as internet images, which is different from how they usually view them. However, there is evidence that the method of viewing the radiographs does not contribute appreciably to variation (Mellema et al., 2017). Fifth, there were overlapping options for years of independent practice (after 2020, 2020–2015, 2015–2010, 2010–2000, before 2000 rather than after 2020, 2019–2015, 2014–2010, 2009–2000, before 1999) owing to human error, which we unfortunately did not notice up until the statistical analysis. This probably had limited effect on the findings. Sixth, we did not track fracture classification, involvement of the sigmoid notch or characteristics of the ulnar styloid fracture because they are unreliable. In SOVG experiments, how the participant regards and interprets the imaging is part of the experiment. The variability in classification and characterization of the injury is one source of variability in ratings or recommendations. Instead of classifying fractures we sought to provide a representative spectrum of injuries by selecting ten fractures in consecutive order of treatment that met the inclusion and inclusion criteria.
Seventh, the statistical power of SOVG experiments is derived from the number of observations, rather than the number of surgeons. In this regard, participants can rate a subset of radiographs, which we did for practicality. Part of the SOVG process is to limit the burden on participants. The specific radiographs are an explanatory variable, but each scenario–radiograph combination is unique and it does not matter experimentally which radiographs a specific participant reviews. Eighth, we did not collect the number of fractures treated each year and cannot comment on the relationship between volume of care and treatment of the distal radioulnar joint. Ninth, we did not discern whether cast immobilization was addressing DRUJ injury or if it was routine for some surgeons after anterior locking plate fixations of the distal radius. Either might be due to habits inconsistent with evidence, but it would have been useful to know the subset that were specific to the DRUJ. The question addressed treatment of the DRUJ, so the lack of inquiry regarding otherwise avoiding a cast should have limited the impact on the results. Tenth, in the review process it was suggested that surgeon participants may respond differently because they are not the treating surgeons. In our view, SOVG participants imagine that they are the treating surgeon when they complete these studies. It is a simulation of actual practice. Lastly, we did not calculate an a priori sample size because we could not predict participation. Because the statistical power is derived from the number of observations rather than the number of participants, even small cohorts of participants generate substantial statistical power. Our ability to measure statistically significant and clinically relevant differences establishes sufficient statistical power in this setting.
The finding that most surgeons recommended additional treatment of the DRUJ after anterior plate fixation of a displaced DRF, cast immobilization in particular, seems inconsistent with the evidence that neither DRUJ ligament injury nor its specific treatment are associated with differences in outcomes of DRF treatment (Xiao et al., 2021). The finding in the current study that higher surgeon likelihood to recommend any treatment of the DRUJ was slightly associated with younger age is common in studies of variation in recommendations for treatment of musculoskeletal injuries and may reflect an implicit bias that younger patients merit greater attention to anatomy and function (Brinkman et al., 2024). The variation in treatment of injury of DRUJ ligaments in conjunction with a displaced DRF may arise either from evidence that predates anterior plate fixation or overestimation of the reliability and importance of physical examination for DRUJ instability (Fricker et al., 2015), but we did not study the rationale for specialist ratings.
The observation that a base of ulnar styloid fracture is associated with surgeon recommendation for reattachment of the DRUJ ligaments is consistent with previous evidence that surgeons are more likely to recommend operative treatment of a DRF when there is a concomitant ulnar styloid fracture (Neuhaus et al., 2015a, 2015b). This tendency to be specifically concerned and motivated by a base of ulnar styloid fracture runs counter to the evidence that a base of ulnar styloid fractures, at least the majority that are close to normal alignment after volar plate fixation of the radius, are not associated with final outcomes and do not benefit from specific treatment (Gogna et al., 2014; Mulders et al., 2018; Souer et al., 2009). In addition, there is evidence that radiographic nonunion of an ulnar styloid base fracture is irrelevant (Buijze and Ring, 2010; Kim et al., 2011; Ozasa et al., 2013; Wijffels et al., 2014; Yuan et al., 2017; Zyluk et al., 2014). It is unclear whether surgeons who still tend to recommend specific treatment of the DRUJ ligament injury are unaware of this evidence or do not believe the evidence is sufficient or convincing.
Supplemental Material
sj-docx-1-jhs-10.1177_17531934261449057 – Supplemental material for Factors associated with variation in treatment of the distal radioulnar joint after plate fixation of distal radial fractures
Supplemental material, sj-docx-1-jhs-10.1177_17531934261449057 for Factors associated with variation in treatment of the distal radioulnar joint after plate fixation of distal radial fractures by Alexander Drost, Niels Brinkman, David Ring, Steven L Moran, Rohit Arora and Niels WL Schep in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-docx-2-jhs-10.1177_17531934261449057 – Supplemental material for Factors associated with variation in treatment of the distal radioulnar joint after plate fixation of distal radial fractures
Supplemental material, sj-docx-2-jhs-10.1177_17531934261449057 for Factors associated with variation in treatment of the distal radioulnar joint after plate fixation of distal radial fractures by Alexander Drost, Niels Brinkman, David Ring, Steven L Moran, Rohit Arora and Niels WL Schep in Journal of Hand Surgery (European Volume)
Footnotes
Acknowledgements
The authors would like to thank Sina Ramtin MD for helping to construct and distribute the survey.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Institutional Review Board of the University of Texas at Austin (STUDY00007354).
Informed consent
Informed consent and consent to participate were obtained by completion of the survey.
Supplementary material
Supplemental material for this article is available online.
Data availability
Data is readily available upon request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.