
Abstract
Introduction:
The Honda Walking Assist (HWA) is a hip-wearable exoskeleton robot for gait training that assists in hip flexion and extension movements to guide hip joint movements during gait. This study aimed to evaluate the effects of walking exercises with HWA in patients who underwent total knee arthroplasty (TKA).
Materials and Methods:
This study involved 10 patients (11 knees) in the HWA group and 11 patients (11 knees) in the control group who underwent conventional physical therapy. The patients assigned to the HWA group underwent a total of 17-20 gait training sessions, each lasting approximately 20 min from week 1 to 5 following TKA. Self-selected walking speed (SWS), maximum walking speed (MWS), range of motion (ROM), knee extension and flexion torque, and Western Ontario and McMaster Universities Osteoarthritis Index subscales of pain (WOMAC-p) and physical function (WOMAC-f) scores were measured preoperatively, at 2, 4, and 8 weeks following TKA.
Results:
Interventions were successfully completed in all patients, with no severe adverse events. A significant difference was noted in the time × group interaction effect between preoperative and week 2 SWS and MWS. Regarding knee function, there was a significant difference in the time × group interaction between preoperative and week 2 active ROM extension; however, no significant difference in knee torque, WOMAC-p, and WOMAC-f scores were observed. In the between-group post hoc analysis, WOMAC-f in the HWA group was higher than that in the control group at week 8.
Discussion:
Although the control group showed a temporary reduction in SWS and MWS 2 weeks after TKA, the HWA group did not. These results suggest that HWA intervention promotes early improvement in walking ability after TKA.
Conclusions:
The gait training using HWA was safe and feasible and could be effective for the early improvement of walking ability in TKA patients.
Introduction
Total knee arthroplasty (TKA) is the primary treatment modality for patients with severe knee osteoarthritis to eliminate pain and improve walking ability, physical function, and quality of life (QOL). 1 -5 However, previous reports have shown that after TKA surgery, temporary reduction in knee muscle strength, decline in knee range of motion (ROM), bodily pain, and a decrease in walking speed occur. 4 -8 The length of hospital stay after TKA surgery is trending downward, 9,10 and patients are often discharged before they have fully recovered their walking ability and knee function. Therefore, early postoperative improvements in walking ability and activities of daily living (ADL) are necessary, and they are important goals of postoperative rehabilitation
In general, physical therapy interventions, such as lower extremity strength training, ROM exercises, balance exercises, and ADL training, are provided to patients after TKA to minimize postoperative functional decline. 11,12 Recently, the effects of using robotics for walking exercises have been examined, 13 -15 and exoskeletal robotic exercises have been proposed for patients who have undergone TKA to improve postoperative knee function and walking ability. 16 -19 However, several of these devices are heavy and have a strong exoskeleton mechanism to provide lower leg support because they are intended to be used during repetitive walking exercises for severely paralyzed patients. As patients after TKA surgery do not have severe paralysis, these exoskeleton-type robotic devices may not be efficient in clinical settings because of the large scale of the devices and time it takes to fit them. Therefore, we focused on the Honda Walking Assist® (HWA) device, which is a light and simple wearable robotic device for gait training.
The HWA has actuators placed at the hip joint to assist with hip flexion and extension and to guide left-right symmetry of gait (e.g., temporal and spatial parameters including symmetry of stride length and symmetry of stance time) by adjusting the timing and intensity of the assist. Angular and torque sensors placed at the hip joint monitor the hip joint angle, and the “assist torque” assists hip joints based on an algorithm for regulating and correcting gait 20 (Figure 1A). We previously used the HWA for gait training and observed improved lower limb kinematic parameters (e.g., stiff knee gait pattern), as well as early improvement of walking ability after surgery in a patient who underwent TKA. 21 In addition to the aforementioned improvement of gait symmetry, we hypothesized that walking practice using a hip-driven exoskeleton-type robot can promote early recovery of walking and knee function in patients with knee joint diseases, since hip assist with the HWA can influence lower extremity kinematics during gait (Figure 1B). For this reason, we conducted a comparative study with a control group that received conventional physical therapy.

A, Gait training with the Honda Walking Assist (HWA)® device. B, The mechanism of knee flexion during the swing phase due to hip assistance using the HWA device. The HWA assistance has the effect of lifting the thigh (red arrow) during the swing phase (b and c), thereby promoting knee flexion (blue arrow).
The purpose of this study was to verify safety, feasibility, and effectiveness of the walking exercise with HWA in postoperative TKA patients would result in early improvement of walking ability and knee function.
Method
Participants
Between March 2015 and April 2020, 23 subjects (24 knees), excluding those who participated in other clinical trials and with a central nervous system disease such as cervical myelopathy, who underwent TKA at our hospital participated in this study. These patients were divided into 2 groups before surgery (HWA and control groups). Two patients were unable to continue the study, 1 due to postoperative delirium and the other due to wound infection. Finally, 10 patients (11 knees) in the HWA group and 11 patients (11 knees) in the control group completed the intervention period. Four patients in the control group were lost to follow-up at week 8 because they did not visit the hospital at the time of measurement (Figure 2).

Flowchart showing allocation of patients in the study.
The surgical procedure was similar to that described in previous reports. 19,21 With the patients under general anesthesia, we made a midline skin incision and reached the joint using a medial parapatellar approach. The patella was not replaced, and the posterior cruciate ligament was retained. We used a Persona® (Zimmer Biomet, Warsaw, IN, USA) implant for the femoral component and a NexGen® Trabecular Metal™ Monoblock Tibia (Zimmer Biomet) implant for the tibial component.
The ethics committee of Ibaraki Prefectural University of Health Sciences approved the study(no. e98 and e204). We explained the purpose of the study to the patients verbally and obtained written consent.
Intervention
The patients allocated to the HWA group underwent gait training using the HWA from week 1 to 5 following TKA. Training was conducted at the hospital and consisted of 4-5 sessions, each lasting ∼20 min (excluding resting time) per week, for a total of 17-20 sessions. Moreover, the patients in both groups underwent conventional rehabilitation during the intervention period, such as ROM exercises; stretching; muscle strengthening; balance training; ADL training such as toileting, bathing, and bedside tasks; gait training; and stair climbing training. Each HWA training session was integrated with the walking exercises during physical therapy sessions. The patients allocated to the control group underwent conventional rehabilitation only during the intervention period. In order to compare the amount of intervention, the total physical therapy time during the intervention period was investigated in both groups.
Adverse events such as exacerbation of knee pain and skin problems involving wounds were carefully observed during and after the HWA training. In addition, knee pain was assessed using the visual analog scale (VAS) during each HWA training session and compared to that of walking without HWA on the same day.
Methods of Assessment
Figure 3 summarizes the parameters and timing of measurements related to knee function and walking ability.

Parameters and timing of the measurements and intervention periods.
Knee function measurements included ROM in terms of knee flexion and extension during passive and active movement of the operated knee; knee extension and flexion torque (representing quadriceps and hamstring strength); and Western Ontario and McMaster Universities Osteoarthritis Index subscales of pain (WOMAC-p) and physical function (WOMAC-f) scores, modified for the Japanese context. 22 Isometric knee torque was measured using a Biodex System 4 dynamometer (Biodex Medical Systems, Inc., NY, USA), with the knee fixed at 60° of flexion. Each torque was measured 3 times for 5 s at a time, and the peak torque value was divided by the body weight for further analysis.
Measurements related to walking ability included self-selected walking speed (SWS), maximum walking speed (MWS), mean step length at SWS and MWS, and cadence at SWS and MWS. SWS and MWS tests were conducted without the HWA on a walking path with an extra path of 3 m before and after the 10 m measurement section. Steps were counted during these tests to calculate the step length and cadence. These measurements were performed before TKA and at 2, 4, and 8 weeks following TKA.
Statistical Analysis
A few missing values were included in the data. Multiple imputation is commonly practiced under the assumption that data are missing at random (MAR). Imputation was conducted using a fully conditional specification approach using PROC MI in SAS 6.4 (SAS Institute Cary, NC, USA). Student’s t-test was used to confirm the differences between the 2 groups at each time point. The effect size was calculated using Cohen’s d. The changes in the 8-week training after surgery in the control and HWA intervention groups were examined using generalized linear mixed models (GLMM), using the SPSS 26.0 (GENLINMIXED procedure; IBM Corp., Armonk, NY, USA). The main effects of treatment group and time, as well as the treatment group × time interaction effect, were examined using the mixed-effect models. Statistical significance was measured at the 5% level.
Results
Interventions were successfully completed in all patients, with no severe adverse events. No patient experienced skin trouble during gait training with HWA. In the initial phase of the intervention, 1 patient complained of mild pressure pain at the femoral cuff attachment site; however, this improved by changing to a larger attachment. Comparing knee pain during walking exercise with and without HWA, knee pain worsened in 1 case and decreased in 6 cases.
Table 1 summarizes the preoperative characteristics of patients, namely, age, sex, weight, height, body mass index (BMI), disease, TKA-operated side, contralateral side TKA, WOMAC-p score, and WOMAC-f score. The differences in patient characteristics between the 2 groups were not significant.
Preoperative Baseline Characteristics of the Patients.a

Abbreviations: BMI, body mass index; OA, osteoarthritis; RA, rheumatoid arthritis; TKA, total knee arthroplasty; WOMAC-P, Western Ontario and McMaster Universities Osteoarthritis Index subscales of pain scores; WOMAC-f, Western Ontario and McMaster Universities Osteoarthritis Index subscales of physical function scores.
a Values are expressed as numbers or as mean ± SD.
Walking Ability
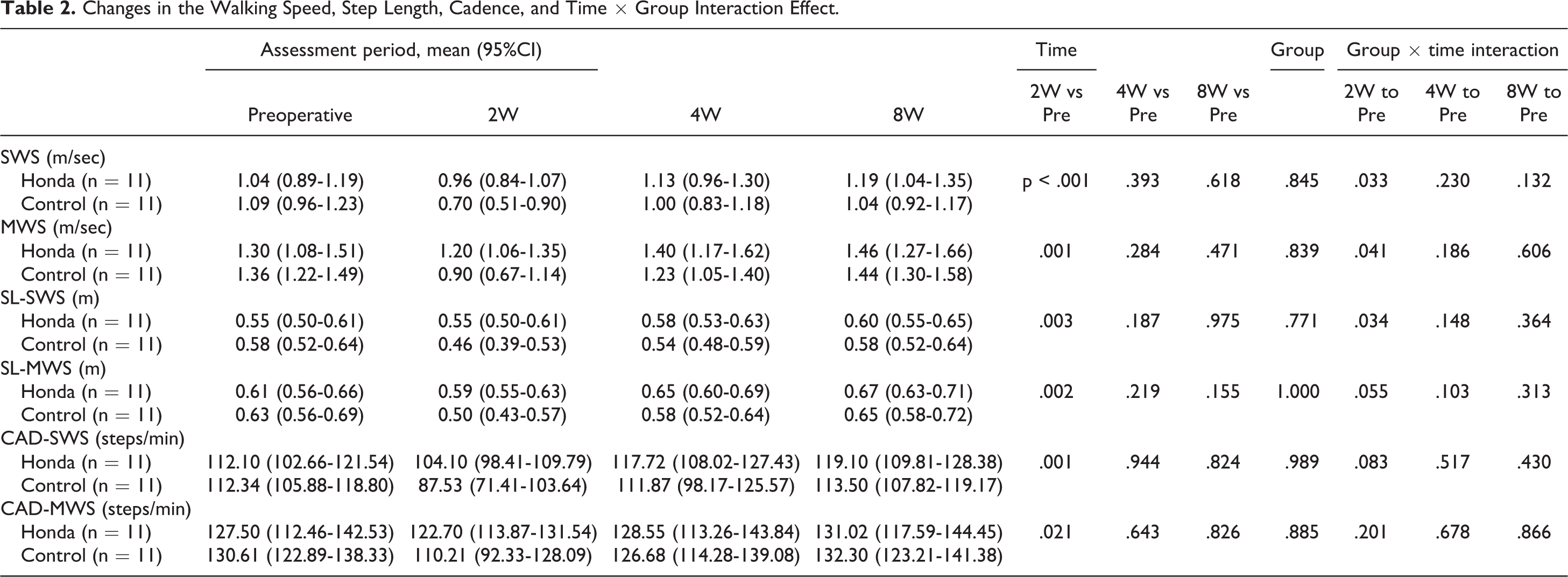
The results of walking ability are summarized in Tables 2 and 3. The main effect of time was significant between pre-operation and week 2 for all measurements, although the differences between pre-operation and week 4 or pre-operation and week 8 were not significant. The main effect of the group was not significant. Regarding the time × group interaction effect, there were significant differences in SWS, MWS, and SL-SWS between pre-operation and week 2. SWS in the control group decreased significantly from 1.09 m/s (95% CI, 0.96-1.23) to 0.70 m/s (95% CI, 0.51-0.90), whereas in the HWA group, it decreased minimally from 1.04 m/s (95% CI, 0.89-1.19) to 0.96 m/s (95% CI, 0.84-1.07). Similarly, MWS in the control group decreased significantly from 1.36 m/s (95% CI, 1.22-1.49) to 0.90 m/s (95% CI, 0.67-1.14), whereas in the HWA group, it decreased only slightly from 1.30 m/s (95% CI, 1.08-1.51) to 1.20 m/s (95% CI, 1.06-1.35). In the between-group post hoc analysis, the SWS (p = .022, Cohen’s d = 1.09), MWS (p = .025, Cohen’s d = 1.04), SL at SWS (p = .032, Cohen’s d = 0.94), and SL at MWS (p = .036, Cohen’s d = 1.02) were greater in the HWA group than in the control group at week 2.
Changes in the Walking Speed, Step Length, Cadence, and Time × Group Interaction Effect.
Walking Ability in the HWA and Control Groups.

a Independent sample t test.
b The effect size was calculated using Cohen’s d.
Knee Range of Motion
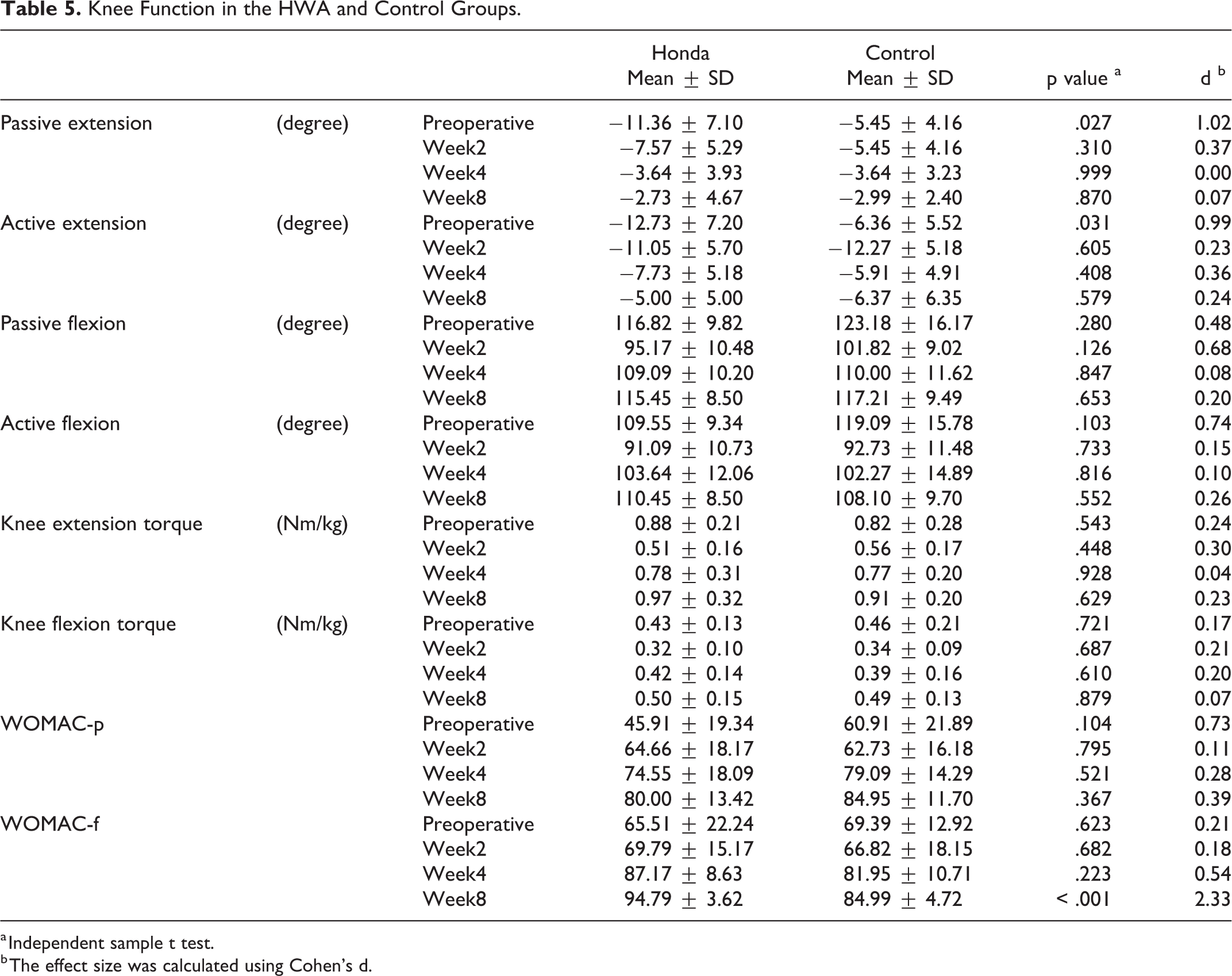
The results of the knee ROM are summarized in Tables 4 and 5. The main effect of time between pre-operation and week 2 was significant for ROM extension active, flexion passive and flexion active, pre-operation and week 4 for ROM flexion passive and flexion active, and pre-operation and week 8 for flexion active. The main effect of the group was not significant. Regarding the time × group interaction effect, there was a significant difference in ROM extension active between pre-operation and week 2. Extension active in the control group decreased significantly from −6.36° (95% CI, −10.07, −2.66) to −12.27° (95% CI, −15.75, −8.79), whereas in the HWA group, it increased from −12.73° (95% CI, −17.56, −7.89) to −11.05° (95% CI, 14.88, −7.22).
Changes in Knee Range of Motion, Knee Torque, WOMAC-p and WOMAC-f Scores, and Time × Group Interaction Effect.

Knee Function in the HWA and Control Groups.
a Independent sample t test.
b The effect size was calculated using Cohen’s d.
In the between-group post hoc analysis, the preoperative measurements of passive extension (p = .027, Cohen’s d = 1.02) and active extension (p = .031, Cohen’s d = 0.99) in the HWA group were lower than those in the control group.
Knee Torque
The results of the knee torque are summarized in Tables 4 and 5. The main effect of time between pre-operation and week 2 for torque extension was significant. The main effect of group and time × group interaction effect was not significant.
Knee Pain and Physical Function
The WOMAC-p and WOMAC-f scores are summarized in Tables 4 and 5. The main effect of time between pre-operation and week 4 for WOMAC-p and pre-operation and week 8 for WOMAC-p and WOMAC-f was significant. The main effect of group and time × group interaction effect was not significant.
In the between-group post hoc analysis, WOMAC-f (p < 0.001, Cohen’ s d = 2.33) in the HWA group was higher than that in the control group at week 8.
Discussion
The results of this study revealed a time × intervention interaction effect in SWS and MWS between pre-operation and week 2, indicating that the HWA group exhibited a significantly faster improvement from postoperative gait dysfunction. A previous report stated that improvement in walking speed after TKA is slow and inadequate even 3 months postoperatively. 23 Moreover, it has been reported that postoperative patients may have residual limitations in walking ability and knee function at least more than 1 year after TKA. 7,8 Although there are few reports on walking speed in the early postoperative period, SWS and MWS at 2 weeks 19,24 and 4 weeks 6 after TKA were decreased than in the preoperative period. In this study, although the control group showed a temporary reduction in SWS and MWS 2 weeks after TKA, the HWA group did not. These results suggest that HWA intervention promotes early improvement in walking ability after TKA.
Although the preoperative knee extension angle in the HWA group was significantly lower, the postoperative knee extension angle improved as much as that of the control group. It is unclear whether HWA intervention plays a role in this result; however, early improvement in walking ability may have had a positive impact.
According to studies that investigated the relationship between knee extension torque and walking ability, the 2 factors were reported to be strongly correlated in patients after TKA. 4,25,26 Knee extension and flexion torque at weeks 2, 4, and 8 were not significantly different between the 2 groups in this study, indicating that the improvement in knee strength was not causally related to the improvement in walking speed. In our previous reports, we demonstrated that HWA assistance promotes knee flexion by lifting the thigh during the swing phase, and HWA intervention is effective in improving stiff knee gait whereby knee flexion is reduced during walking. 21 Although gait kinematic parameters were not measured in this study, HWA intervention could contribute to the early improvement of walking ability with such a mechanism.
The HWA intervention did not exacerbate knee pain, as WOMAC-p showed comparable improvement to the control group. However, when comparing knee joint pain during the HWA intervention, in 6 out of 10 cases, there was a decrease in joint pain with HWA compared with that without HWA during walking exercises. This result suggests that HWA intervention may be effective in reducing the load on the patients during walking exercise. Although WOMAC-f showed no time × intervention interaction effect, in the between-group post hoc analysis, WOMAC-f in the HWA group was higher than that in the control group at week 8. This finding suggests that the HWA intervention improves postoperative physical function.
A review of the literature on walking speed showed that, as highlighted by Montero-Odasso, the low-gait-velocity group had a higher incidence of adverse events, such as predictors of hospitalization, caregiver requirements, and new falls in elderly people, than the high- and median-gait velocity groups. 27 According to Purser, walking speed reduction was associated with poorer health status, poorer physical functioning, more disabilities, additional rehabilitation visits, increased medical-surgical visits, longer hospital stays, and higher costs in hospital inpatients. 28 As walking ability and knee function are associated with postoperative patient satisfaction in TKA patients, 23 early improvement in walking ability is crucial for the benefit of patients. The HWA intervention improves walking ability after the early stage of surgery, which is expected to shorten the hospitalization and rehabilitation period. In addition, the improvement in physical function at week 8 could be expected to hasten the return to daily life and work and prevent falls. This device incurs a rental fee, so which is a potential cost. However, if the number of days spent in the hospital is reduced by encouraging patients to improve quickly, the total cost of medical care could be reduced. In order to make effective use of this device, there is room for consideration on how to make it available to more patients, for example, by giving them the opportunity to self-exercise by wearing the device themselves. The HWA is easy to wear and light-weight, making it ideal for rehabilitation after TKA. Moreover, it was safe to use and expected to be effective for the early recovery of walking ability and physical function after TKA. However, the improvements in muscle strength and ROM were similar to those in the control group. Rehabilitative modalities have been suggested for the recovery of strength and ROM after TKA, with a focus on the early incorporation of exercise therapy, balance training, aquatic therapy, cryopneumatic therapy, neuromuscular electrical stimulation, and transcutaneous electrical nerve stimulation. 12 Further benefits could be expected by combining the HWA training with training focused on the aforementioned parameters. The present study was a pilot study with an insufficient sample size that lacked randomization of patient allocation and a blinded intervention and evaluation. Furthermore, it is also necessary to examine which types of patients are most amenable to walking exercise using the HWA in the future.
Conclusions
Gait training using HWA was safe and feasible and could be effective for the early improvement of walking ability in patients who underwent TKA. Further validation is needed to determine those patients in whom the HWA intervention will be most effective and also identify strategies to achieve better results in the long term.
Limitations
This study had a few limitations. First, this was a pilot study, the number of cases was small, and some data were missing and were analyzed by interpolating them using statistical methods. Second, since the main objective of this study was to examine the early postoperative recovery of walking ability and knee function, we only followed the patients up to 8 weeks after TKA, and the long-term effects are unknown. Third, although there was no difference in patient characteristics between the HWA and control groups, the allocation was not randomized. Furthermore, the intervention and evaluation were not blinded; hence, there were various risks of bias. This study was a single-center validation, and future multi-center validations with larger sample sizes are required to increase reliability.
Footnotes
Acknowledgments
We would like to thank the Physical Therapy Department at Ibaraki Prefectural University of Health Sciences Hospital, represented by Kazuhide Tomita, the manager of the Department of Rehabilitation; Tomoyuki Matsuda, the manager of the Department of Physical Therapy; and Keiko Miyamoto, a robotic technical assistant. We would like to thank Editage (![]() ) for English language editing.
) for English language editing.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Honda Motor Corporation lent us the HWA free of charge for this research.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partly supported by a Grant-in-Aid for Project Research of the Ibaraki Prefectural University of Health Sciences (1961) and the Japan Society for the Promotion of Science KAKENHI (20H01147).