
Abstract
Patients with osteogenesis imperfecta (OI) usually also show osteoporosis and bone fragility. Because these defects may also be combined with an airway that is difficult to manage, abnormal platelet function, and other problems, the perioperative management of anesthesia represents a substantial challenge. Therefore, it is important to be able to predict the risks during the perioperative period and to formulate and implement specific high-quality anesthesia management plans for such patients when they experience trauma. We report the case of a 59-year-old female patient with OI who experienced trauma resulting in fractures of the left proximal humerus and right hip. She required open reduction and internal fixation of her humerus and total hip arthroplasty. However, she also had obstructive sleep apnea syndrome, and an airway assessment indicated that her airway would be difficult to maintain. General anesthesia combined with a nerve block was administered. An ultrasound-guided bilateral superior laryngeal nerve block and cricothyroid membrane puncture were used to facilitate endotracheal intubation. An ultrasound-guided “hourglass-pattern” fascia iliaca block was performed for perioperative analgesia. The use of a regional block and preparation for the difficult airway access represented important and successful aspects of the management of anesthesia in this patient.
Keywords
Introduction
Osteogenesis imperfecta (OI) is a rare connective tissue disorder that is characterized by hereditary bone dysplasia, deformity, and fragility. 1 A diagnosis of OI is usually made on the basis of family history; genetic testing; and clinical characteristics, such as fracture while young, skeletal dysplasia, osteoporosis, and skeletal deformity. 2 It manifests as short stature, short neck, blue or grey sclera, defective dentition, brittle bones, coagulopathy, hypermobile joints, restrictive pulmonary disease, and craniovertebral junction anomalies. 3 OI also increases the risk of hemorrhage, and insufflation every 3 to 5 minutes during anesthesia in patients with brittle OI can cause iatrogenic fracture. 3 Therefore, orthopedic surgery in patients with OI continues to present a substantial challenge for anesthesiologists.
Here, we report the perioperative management of anesthesia in an adult patient with OI and multiple fractures caused by minor trauma. We obtained the patient’s consent for treatment and have reported this case according to the CARE guidelines. 4
Case report
The patient provided their written informed consent and approved the educational publication of the details of their case. A 59-year-old woman (body mass 86 kg, height 148 cm, body mass index 39.3 kg/m2, American Society of Anesthesiologists status III) was scheduled for the open reduction and internal fixation of a left proximal humerus fracture and right total hip arthroplasty (THA). The patient was admitted to hospital 3 hours after a fall, which caused a limitation of activity and pain in her right hip and left upper arm. The patient usually snored during sleep and regularly woke because of apnea, and this symptom was more marked in the supine position; therefore, she normally slept in a lateral position. After a specialist consultation, the patient was diagnosed with obstructive sleep apnea syndrome (OSAS).
A physical examination performed on admission showed that the patient’s upper and lower limbs were flexed and could not be straightened. Her neck was short and stiff, with a restriction of activity, and her mouth could only be opened to the width of two horizontal fingers. She had cervical spinal ankylosis, a short and thick neck, and poor neck mobility (Figure 1). The sclera of her eyes was blue, but her hearing was normal. The patient had bilateral hip dysplasia and had experienced bilateral hip joint pain since childhood, which had got significantly worse 10 years previously. She had also been treated conservatively for a previous hip fracture. Both her mother and daughter had histories of hip disease and skeletal dysplasia. X-radiographic images obtained at admission are shown in Figure 2. The patients also had a 12-year history of hypertension, for which oral nifedipine was prescribed. Previous cardiac Doppler ultrasonography had revealed poor cardiac systolic and diastolic function and moderate pulmonary arterial hypertension. Her cardiac function was class II.

Preoperative airway assessment of the patient. She was obese and had a broad, short neck.

Pre-operative X-radiographs of the patient. She was obese, had dysplasia of both hips, could not straighten her limbs, and had a fractured right hip and left proximal humerus.
Preoperative laboratory examination revealed a low hemoglobin concentration (86 g/L), a high white blood cell count (9.6 × 109/L), and a high C-reactive protein concentration (570.1 nmol/L). Her bleeding time, measured using the apparatus method, was >8 minutes. Preoperative blood gas analysis revealed a low partial pressure of oxygen (57.60 mmHg) and a pH of 7.46. With respect to renal function, she had a high serum β2-microglobulin concentration (552 nmol/L), a low enzymatic carbonate concentration (21.30 mmol/L), a high creatinine concentration (138.1 µmol/L), a high urea concentration (10.27 mmol/L), a high uric acid concentration (559.8 µmol/L), and a high cystatin C concentration (2.74 mg/L). The patient was diagnosed with renal insufficiency after consultation with a nephrologist. The other parameters measured did not show abnormalities.
After arrival in the operating room, the patient underwent routine monitoring. Her initial vital signs included an oxygen saturation of 93%, blood pressure of 168/95 mmHg, and heart rate of 89 beats/minute. After she was supplied with oxygen (6 L/minute) via a face mask, her oxygen saturation increased to 99%. Radial artery puncture was performed to monitor arterial blood pressure and for arterial blood gas analysis (Table 1). Airway assessment indicated that her airway would be difficult to manage; therefore, we aimed to perform a slow endotracheal intubation while the patient was awake. After sedation with 1 mg of midazolam, 10 μg of sufentanil, and 0.2 mg glycopyrrolate, we sprayed local anesthetic onto her tongue and epiglottal root via a laryngeal anesthesia tube, then 3 minutes later, we performed an ultrasound-guided bilateral superior laryngeal nerve block. 5 Four milliliters of 2% lidocaine was administered to facilitate an ultrasound-guided cricothyroid membrane puncture, then conscious endotracheal intubation was performed under the guidance of a fiberoptic bronchoscope 3 minutes later. A single-lumen endotracheal tube with an inner diameter of 7 mm was passed smoothly. The patient cooperated well during the entire process, and did not cough, feel nauseous, or experience significant discomfort.
Results of arterial blood gas analysis before, during, and after surgery.

PaCO2/O2, arterial partial pressure of carbon dioxide/oxygen.
Twenty milliliters of 0.33% ropivacaine was used for a left-sided ultrasound-guided interscalene brachial plexus block and 30 mL of 0.33% ropivacaine was used to perform a right-sided “hourglass-pattern” fascia iliaca block. 6 General anesthesia was maintained using a combination of propofol (10 mL/hour), a 0.015 volume-fraction of sevoflurane, and intermittent administration of a muscle relaxant (cisatracurium) and sufentanil, according to changes in hemodynamic parameters and the depth of anesthesia. An autologous blood recovery system was used to protect blood volume during the procedure. Because the patient’s proximal femoral shaft was accidentally split during the process of expanding the marrow cavity, open reduction and internal fixation of the right proximal femoral shaft fracture was performed (Figure 3).
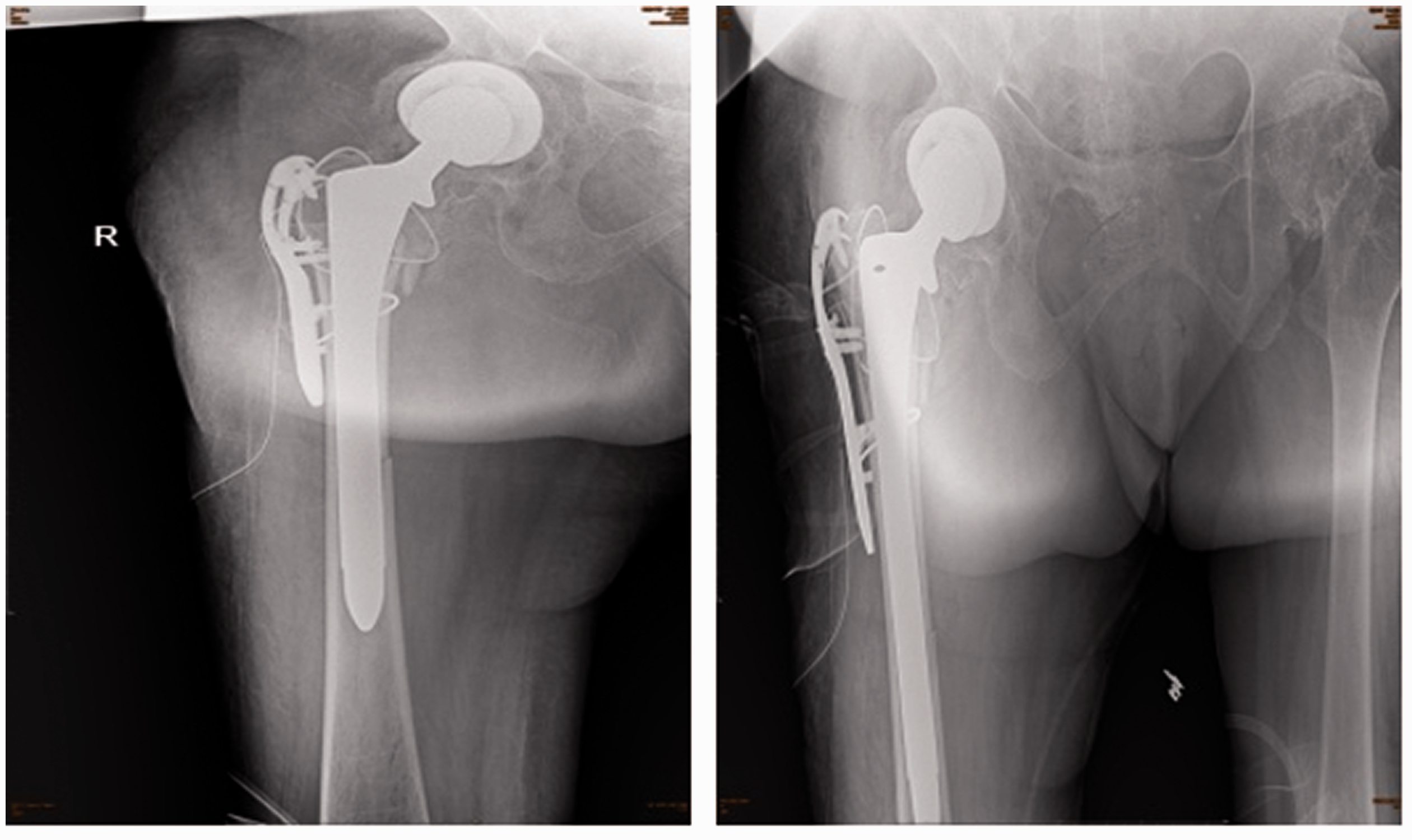
Post-operative X-radiographs of the patient, showing the results of right total hip arthroplasty and internal fixation of the right proximal femoral shaft fracture.
The surgery lasted for 4 hours and 30 minutes and the temperature of the patient was monitored throughout using an infrared frontal thermometer. Totals of 2000 mL Ringer’s solution and 600 mL autologous blood, as well as two transfusions of erythrocyte suspension, were performed during the surgery. The volumes of blood lost and urine passed were 1300 mL and 850 mL, respectively. The results of arterial blood gas analysis are shown in Table 1. The patient was resuscitated smoothly, and received low-flow oxygen through a nasal catheter (2 mL/minute) after returning to the ward. The duration of analgesia yielded by the ultrasound-guided interscalene brachial plexus block was approximately 7 hours, and that yielded by the ultrasound-guided “hourglass-pattern” fascia iliaca block was approximately 9.5 hours.
Postoperatively, the patient regained consciousness, had stable vital signs, and had no memory of the process of endotracheal intubation. No remedial analgesics were used, and no nausea, vomiting, or other adverse reactions associated with the low-dose opioids or other analgesics used during the perioperative period developed. The patient was quite satisfied with her anesthesia. Blood gas analysis was performed 10 hours following the surgery, the results of which were satisfactory (Table 1). The patient’s visual analog scale pain scores at rest and during activity 2 hours, 12 hours, and 24 hours after the surgery were all <4 points. In addition, she was able to flex and extend her ankle joint and quadriceps femoris soon after the surgery.
Discussion
OI is also called “brittle bone disease” because fractures can occur following slight or no trauma. A previous survey showed that OI affects approximately 6 to 7 people per 100,000 and is present in approximately 1 in 20,000 births. 7 The disorder is caused by a defect in type I collagen synthesis, secondary to a gene mutation. Type I collagen is the principal type in bone, skin, sclera, dentine, and other tissues; therefore, lesions in these locations are more obvious. 2 Patients with OSAS often show cognitive dysfunction and cardiovascular disease. In addition, because of abnormalities of pharyngeal anatomy, upper airway dilation, and ventilatory control, recurrent pharyngeal collapse and even apnea occur during sleep.8,9 Therefore, the perioperative management of anesthesia in patients with these conditions is very challenging.
The literature regarding OI consists mostly of case reports and there is a lack of randomized controlled trials. Therefore, there is little evidence in the literature regarding the potential risks associated with the use of regional and neuraxial techniques in patients with OI. 10 The present patient had both a humeral fracture and an intertrochanteric fracture, which would have been associated with larger internal hemorrhage than a single fracture. Furthermore, because of poor platelet function and the pathological characteristics of the osteoporosis and bone fragility of the patient, the surgery was expected to be challenging and of long duration. Under these circumstances, it is necessary to predict blood loss in a timely fashion and institute appropriate blood transfusion and circulatory management strategies. The circulatory management strategy should then be adjusted according to blood loss and the changes in hemodynamics. Yap et al. 11 showed that the choice of anesthetic protocol affects the prognosis and rehabilitation of patients. They compared the effects of volatile anesthesia and propofol-based total intravenous anesthesia on cancer outcomes and showed that the latter was associated with superior overall survival.
The intravenous administration of general anesthesia minimizes the use of drugs that require renal metabolism. In the present case, an ultrasound-guided left intermuscular sulcus brachial plexus block and an “hourglass-pattern” fascia iliaca block were used, which effectively blocked the brachial plexus, lateral femoral cutaneous nerve, and obturator nerve.12,13 The “hourglass-pattern” fascia iliaca block is an effective means of analgesia in patients undergoing hip surgery. In addition, the use of a combination of general anesthesia and nerve blocks not only reduces the amount of intravenous drugs used, but also reduces the patient’s stay in the post-anesthesia care unit. 14 It can provide satisfactory postoperative analgesia, with few adverse effects, help ensure that early rehabilitation exercise is possible, and hence contribute to the rapid recovery of patients. 15 It has previously been reported that patients with deficient osteogenesis often have airways that are difficult to access, and therefore guidance for difficult airway management should be followed. 16 The slow, conscious, fiberoptic bronchoscope-guided endotracheal intubation method used in this case is relatively safe. 17
OI is a serious disease that is associated with multiple complications. It is necessary to determine how severe the disease is, undertake a full preoperative evaluation, and develop an appropriate individualized anesthesia management plan for patients who require surgery. The recognition of risk factors in advance and the optimization of the preoperative health status of patients with OI helps ensure the safety and smoothness of the anesthesia. On the basis of our findings with the present patient, we suggest that when patients with OI require surgical treatment, the use of slow, conscious endotracheal intubation, an ultrasound-guided bilateral superior laryngeal nerve block, and cricothyroid membrane puncture can significantly relieve their intubation response. In addition, the use of general anesthesia in combination with a nerve block is suitable for patients with OI. This approach not only reduces the amount of opioid that must be administered, but also improves perioperative analgesia.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211028420 - Supplemental material for Management of anesthesia in a patient with osteogenesis imperfecta and multiple fractures: a case report and review of the literature
Supplemental material, sj-pdf-1-imr-10.1177_03000605211028420 for Management of anesthesia in a patient with osteogenesis imperfecta and multiple fractures: a case report and review of the literature by Huiyue Wang, Xiao Huang, Anshi Wu and Qianyu Li in Journal of International Medical Research
Footnotes
Author contributions
Conceptualization: QL, HW, XH, and AW.
Data curation: QL, HW, and XH.
Investigation: HW, and XH.
Writing-original draft: HW and XH.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Baoding First Central Hospital. The written informed consent of the patient was obtained for publication.
Funding
This study was supported by a Baoding Science and Technology Planning Project (no. 1951ZF066), Baoding, Hebei, China.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.