
Abstract
Introduction
Compared to other patients, Parkinson disease (PD) patients may experience suboptimal outcomes after hip fracture. The purpose of this study was to describe and compare characteristics and outcomes of hip fracture patients with PD to those without PD.
Methods
This retrospective cohort study included all patients admitted for hip fracture within a large healthcare system between July 1, 2017 and June 30, 2019. Demographics, injury characteristics, Charlson Comorbidity Index (CCI), treatment characteristics, and outcomes including complications, readmissions, and mortality were extracted. Patients with PD were compared to those without PD. Chi-square tests, two-sample t-tests, and Fisher exact tests were conducted to identify group differences.
Results
A total of 1239 patients were included (4.0% PD and 96.0% non-PD). PD patients were mostly male (59.2%) compared to mostly female non-PD patients 69.4%, P < .001). PD patients on average had a higher CCI (2.3 vs 1.7, P = .040) and more frequently had dementia (42.9% vs 26.7%, P = .013). No PD patients were discharged home without additional assistance compared to 8.1% of patients without PD. More PD patients were discharged to a skilled nursing facility (SNF) than non-PD patients (65.3% vs 48.2%, P = .021). Only 22.4% of PD patients were previously prescribed osteoporosis medication, and only 16.3% were referred for osteoporosis follow-up after fracture. In-house complications, readmissions, and mortality up to 1 year were comparable between groups (P>.191).
Conclusions
Outcomes between PD patients and non-PD patients were mostly equivalent, but more PD patients required discharge to a higher-level care environment compared to non-PD patients. Although PD seems to be a risk factor for hip fracture regardless of age and sex, most patients had not undergone proper screening or preventative treatment for osteoporosis. These results emphasize the need for early bone health evaluation, multidisciplinary collaboration, and care coordination in preventing and treating hip fractures in PD.
Keywords
Introduction
Parkinson disease (PD) patients are susceptible to recurrent falls1-3 and subsequent hip fractures.1,2,4-8 They exhibit a 3-fold risk of falls compared to the general population, 3 with more than 50% sustaining repeated falls.1,2 Of those that fall, approximately 1/3 sustain 1 or more fractures, with 28-50% of such fractures involving the hip.1,2 PD patients have been found to carry 2-3 times the risk of hip fracture compared to the general population,4-6 with 27% of patients experiencing hip fracture within 10 years of diagnosis. 8 In addition, PD has been found to be associated with lower bone mineral density (BMD)3,9 and higher risk of vitamin D deficiency and osteoporosis, 10 increasing the likelihood of subsequent hip fracture.
Despite the well-known susceptibility of PD patients to falls and hip fractures, a recent literature review uncovered gaps in orthopaedic care of PD patients. 11 Kim et al 12 found in a study of 400 patients that, compared to age-matched and sex-matched non-PD controls, PD patients exhibited a higher prevalence of orthopaedic complaints as well as a lower rate of pharmacologic treatment. 12 Multiple studies have reported worse outcomes for hip fracture among PD patients,13-16 with 1 recent retrospective study of 9225 patients by Coomber et al 13 demonstrating that PD patients exhibit longer hospitalization, higher rate of institutionalization, worse mobility, and higher 1-year mortality than non-PD patients. 13 Although hip fracture risk mitigation algorithms have been developed for PD patients, few recommendations and preventative measures are regularly enacted.17-19
The purpose of this study was to describe and compare hip fracture patients with and without PD within our organization in order to identify opportunities to optimize care. We specifically aimed to identify differences in demographics, comorbidities, injury characteristics, treatment characteristics, and outcomes between these groups.
Methods
This descriptive retrospective cohort study identified all patients in our healthcare system who sustained a hip fracture between July 1, 2017 and June 30, 2019. This was done using a hip fracture registry that tracks all hip fracture-related hospitalizations in 6 hospitals within a large healthcare system. We then performed chart reviews of all admissions with a primary diagnosis of hip fracture. Admissions without an acute fracture of either the femoral neck, intertrochanteric region, or subtrochanteric region were excluded. Fractures of the pelvic ring, acetabulum, greater trochanter, or lesser trochanter, as well as periprosthetic fractures, were also excluded. For patients with more than 1 admissions for the primary diagnosis of hip fracture during the observation period only the earliest admission was included.
Variables of interest extracted from the hip fracture registry included age, gender, body mass index (BMI), Charlson Comorbidity Index (CCI) total score,20-22 diagnosis of osteoporosis (yes or no), use of osteoporosis medication (yes or no), emergency department (ED) length of stay (LOS), hospital LOS, discharge disposition (categorized as “Higher Level Care”, “Home”, “Hospice”, “Expired”, and “Other”), post-discharge osteoporosis care referral (yes vs no), treatment modality (operative vs non-operative), associated surgical CPT codes, and admit to death time (for in-hospital mortality). Regarding discharge disposition, we classified as “Higher Level Care” any discharge destination that referred to an environment with increased supervision and resources to provide more comprehensive patient care for acute and/or complex issues (eg skilled nursing facilities [SNFs], transitional care units [TCUs], long-term care hospitals [LTCs], dedicated home health care, etc.). “Home” referred to discharge to a home without any additional care other than standard of care provided for any hip fracture patient in our healthcare system. “Hospice” referred to any destination where the patient would receive hospice care. “Other” included miscellaneous destinations or dispositions whose care level could not be determined (eg transfers to another hospital, transfers to incarceration status).
Outcomes obtained from the registry included in-hospital mortality, 30-day mortality, 90-day mortality, 1-year mortality, 30-day readmission, 90-day readmission, development of complication (yes vs no), and ICD-10 code of first recorded complication. The electronic medical record (EMR) was abstracted to corroborate hip fracture registry data. Diagnosis of PD was extracted from the EMR using ICD-10 codes G20 and G31.8. Diagnosis of PD at the time of admission, as well as absence of same was confirmed in these patients via chart review by the senior neurologist.
Two groups were analyzed based on diagnosis of PD: patients with PD vs patients without PD. Statistical analysis was done using SYSTAT 13 (SYSTAT Software Inc, San Jose, CA) and Microsoft Excel. Data was summarized and presented via descriptive statistics. Categorical and binary variables were presented as counts and percentages, while continuous data were presented with averages, standard deviations, and 95% confidence intervals. Differences between the groups were identified using either chi-square tests for categorical and binary variables or two-sample t-tests for continuous variables. A P-value of .05 or less was considered to be statistically significant.
Results
We identified 1529 encounters in the hip fracture registry, of which 1239 were eligible for study inclusion (Figure 1). The cohort was mostly female (N = 846, 68.3%) with an average age of 80.3 ± 11.1. Average BMI and CCI were 25.1 ± 5.5 and 1.8 ± 1.8, respectively. A total of 49 patients had a diagnosis of PD (4.0%). Inclusion/exclusion for encounters in the institutional hip fracture registry.
Demographic and Injury Characteristics of Hip Fracture Patients with and without Parkinson (N = 1239).
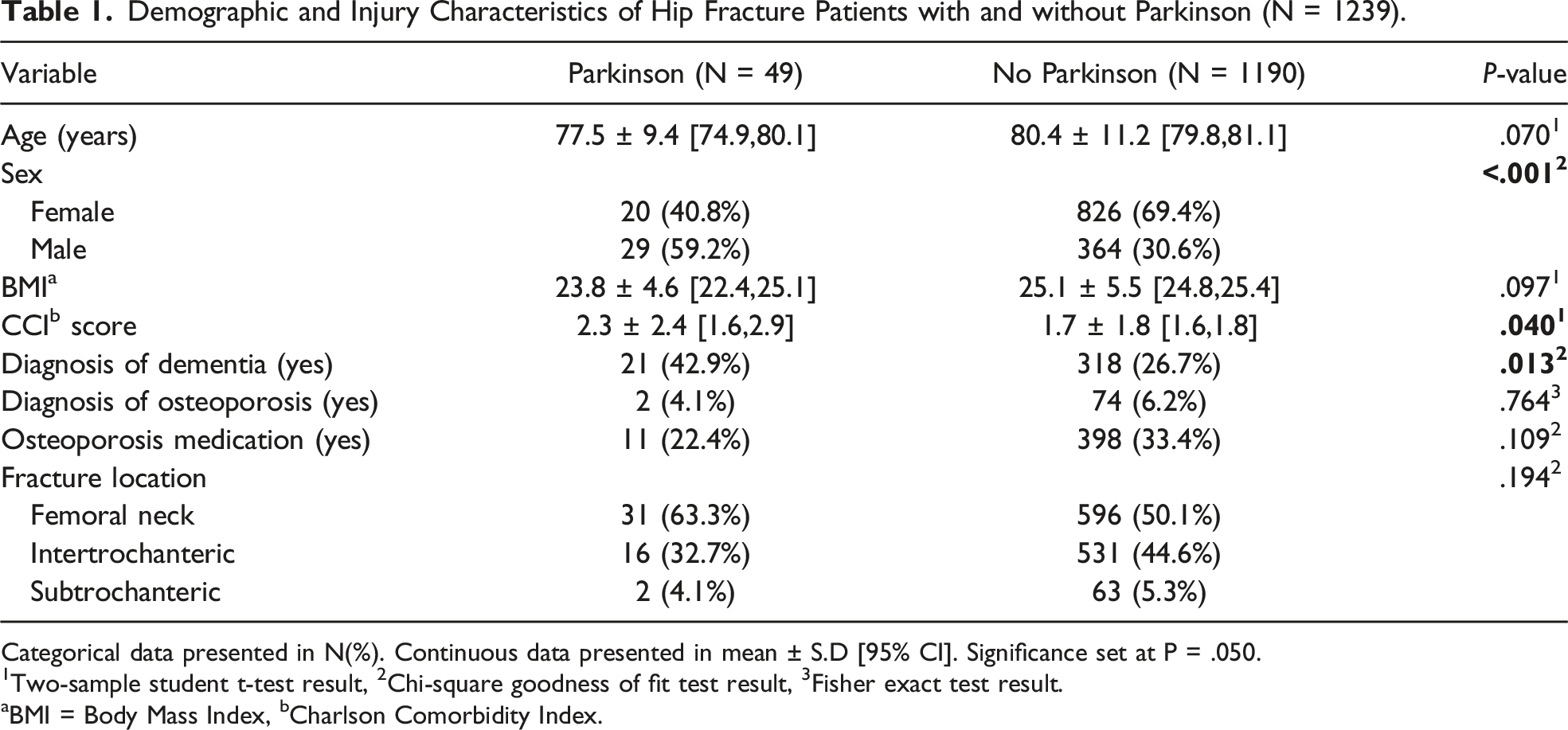
Categorical data presented in N(%). Continuous data presented in mean ± S.D [95% CI]. Significance set at P = .050.
1Two-sample student t-test result, 2Chi-square goodness of fit test result, 3Fisher exact test result.
aBMI = Body Mass Index, bCharlson Comorbidity Index.
Care Pathway for Hip Fracture Patients with and without Parkinson (N = 1239).

Categorical data presented in N(%). Continuous data presented in mean ± S.D [95% CI]. Significance set at P = .050.
1Two-sample student t-test result, 2Chi-square goodness of fit test result, 3Fisher exact test result.
aED = Emergency Department; bLOS = Length Of Stay; cSHS = Sliding Hip Screw; dIMN = Intramedullary Nail; eHigher Level Care = includes skilled nursing facility (SNF), transitional care unit (TCU), long-term care facility (LTC), dedicated home health care, among other services.
One-Year Outcomes for Hip Fracture Patients with and without Parkinson (N = 1239).

Categorical data presented in N(%). Significance set at P = .050.
1Chi-square goodness of fit test result, 2Fisher exact test result.
Discussion
We aimed to describe the PD hip fracture population and compare it to the non-PD cohort within our organization in order to identify opportunities to improve patient care. We found that the PD cohort was predominantly male, had a higher average CCI, and had a higher prevalence of dementia compared to the non-PD group. The PD cohort was also more likely to be discharged to a higher level care facility. The 2 groups demonstrated no significant differences in complications, readmissions, or mortality up to 1 year post-injury. Of note, just 4.1% of PD patients had a prior diagnosis of osteoporosis, and only 22.4% had a prior prescription for an osteoporosis medication. Only 16.3% of PD patients received appropriate bone health referral after discharge.
The baseline demographic differences observed between the groups are consistent with prior knowledge. While it is well known that female sex and older age are associated with increased risk of developing osteoporosis and sustaining fragility fractures,23-25 it is also known that the prevalence and incidence of PD in males is 1.5-2 times higher than in females. 26 This explains the higher proportion of males seen in the PD group (59.2% vs 30.6%). Prior studies have also revealed the fact that patients with PD are more at-risk of developing dementia, 27 which would explain the higher prevalence of dementia within the PD group (42.9% vs 26.7%). Because a diagnosis of dementia is included in CCI scoring (1 point), 20 the slightly higher average CCI in the PD group, which was within a one-point difference of the average CCI for non-PD patients (2.3 vs 1.7), could potentially be a result of the higher prevalence of dementia observed in the group. The PD group also trended slightly younger than the non-PD group (77.5 vs 80.4, P = .070). Although we did not evaluate the effect of these variables on hip fracture risk or outcomes, it is important to note that a diagnosis of PD in and of itself serves as a risk factor for hip fracture.1,2,4-8
PD is additionally associated with lower BMD, risk of vitamin D deficiency, and osteoporosis.3,9,10 The prevalence of osteopenia and osteoporosis in all PD patients, including those without a hip fracture, has been found to be 41.4% and 11.8%, respectively. 28 However, in our study, we found that only 4.1% of PD hip fracture patients had a known diagnosis of osteoporosis. Although there are no established osteoporosis screening guidelines for patients with PD, 36.2% of PD patients without a prior diagnosis were women aged 65 or older. PD patients who did not receive a diagnosis of osteoporosis had an average age of 78.1 ± 9.5. Additionally, only 22.4% of PD patients had record of prescribed osteoporosis medications. If we were to consider this number a more accurate indicator of osteoporosis diagnosis in this population, it would still be suspiciously low considering the fact that it refers exclusively to PD patients with hip fractures rather than all PD patients. While we were unable to ascertain whether these patients received screening, these numbers strongly suggest under-screening in this population. It is also important to note that only 16.3% of PD patients received a referral for bone health evaluation and/or follow-up after sustaining a low-energy hip fracture. These results highlight the opportunity to improve osteoporosis care coordination and bone health screening for patients with PD. Of note, these observations were not statistically different compared to non-PD hip fracture patients (all P>.109, Tables 1 and 2), perhaps indicating an opportunity to optimize care for all hip fracture patients.
Prior studies have evaluated healthcare utilization for PD hip fracture patients compared to non-PD patients. Idjadi et al 29 found in a review of 920 patients (3.4% with PD) that PD patients experienced longer hospital LOS and higher likelihood to be discharged to a SNF compared to non-PD patients. 29 Walker et al 14 similarly reported longer LOS average of 38.9 days compared to non-PD patients in an analysis of 1362 patients (2.1% with PD), despite finding no significant difference in discharge disposition between PD and non-PD patients. 14 Bliemel et al. also reported longer LOS at an average of 17 days for PD patients (4.7% of a total of 402 patients). 15 Most recently, Coomber et al 13 evaluated 9225 patients (4.9% with PD) over a 29-year period and found that PD patients experienced longer LOS (average of 20 days) and a higher likelihood of discharging to an institution. 13 Our study looked at 1239 patients (4.0% with PD) and similarly found that PD patients tend to be discharged to higher level care institutions compared to non-PD patients. However, in contrast to prior studies, we found no difference in hospital LOS between PD and non-PD hip fracture patients, with an average LOS of 5.1 ± 2.6 days for PD patients compared to prior studies. Our relatively short LOS compared to prior studies is likely due to a combination of our relatively recent study period (2017-2019), our practice differences compared to other healthcare systems and/or countries, and our employment of a hip fracture multidisciplinary care pathway.
Hip fracture outcomes in PD patients when compared to other patients are still not well understood. Idjadi et al 29 found that complications, mortality, and recovery of ambulation were equivalent at 1 year between PD and non-PD hip fracture patients. 29 Bliemel et al. found that in-hospital mortality was comparable between PD and non-PD hip fracture patients. 15 Fontalis et al. also identified similar 1-year mortality between these groups in a review of patients that underwent total hip arthroplasty (THA) for hip fracture. 16 In contrast, the more recent and higher power study by Coomber et al 13 demonstrated that hip fracture outcomes tend to be worse for PD patients compared to non-PD patients, reporting higher 1-year mortality as well as worse cognitive decline and post-operative mobility. 13 Walker et al 14 reported a higher reoperation rate for PD patients, likely reflecting higher readmissions and complication rates. 14 Bliemel et al. and Fontalis et al. also indicated higher likelihood of complication for PD patients.15,16 Although we were unable to evaluate functional outcomes for our cohort, our study found that outcomes other than discharge disposition, including complication rates, readmissions, and mortality were comparable between PD patients and non-PD patients up to a year after injury.
It is important to note that complications, readmissions, and mortality are not the only outcomes that can inform care optimization and treatment success. Functional outcomes and patient-reported measures have also been used to evaluate care in PD patients. 13 Hip fracture patients, particularly older and frailer patients, may also have care goals that may differ from traditional goals of treatment. 30 This has led to a notable shift in our healthcare system to focus more on patient-specific goals, manifesting in ways such as higher rates of non-operative treatment in our system (Table 2). A recent study of institutionalized patients similarly demonstrated that, while mortality still remained high, non-operative treatment of hip fractures produced high patient and healthcare proxy satisfaction. 31 Evaluating these alternative outcome measures in PD patients may help inform providers as they work towards defining optimal hip fracture care for these patients.
Best practices for the preventative and post-injury hip fracture care of PD patients are still relatively undetermined and under development.32,33 There has been a call to enhance multidisciplinary care to improve outcomes among these patients. 33 In fact, 1 study found that, despite the fact that just 58% of the included PD patients received care from a neurologist, neurologist involvement was associated with lower likelihood of SNF placement, hip fracture, and mortality. 34 Although 1-year outcomes between PD and non-PD patients were equivalent in our study, we identified some differences in baseline characteristics and in the care process that could help inform best practices. The importance of bone health management in PD patients is well-established, 32 yet our findings suggest that this was not a pre-operative or post-operative priority in our PD patients. Regarding peri- and post-injury care, the only significant difference between the groups in our study was discharge disposition. Outcomes depend on a wide range of factors, and the role of discharge disposition cannot be ignored. Although it was not determined, as it was outside the scope of this study, it is possible that discharge to higher care level facilities with higher degrees of multidisciplinary care can help PD hip fracture patients achieve non-inferior outcomes compared to patients without PD. Considering the high resource utilization and subsequent economic burden this may entail, it may be worthwhile to focus future efforts on optimizing and/or incentivizing discharge and care coordination for these patients to higher level care facilities such as TCUs and SNFs. Finally, considering our equivalent outcomes in the context of shorter hospital LOS compared to prior literature, aiming for early mobilization and discharge to shorten hospital LOS may also improve care for PD patients. Considering the variability in available levels of care and/or resources among different healthcare systems, which may explain the discrepancy in LOS between our study and prior studies, we interpret our results and propose this idea with caution.
The retrospective nature of our study introduces inherent limitations such as the inability to detect causation among associations. Despite our large sample size, only 49 (4.0%) of these patients had a diagnosis of PD, limiting our results and conclusions. This may be aided if studied with higher power, more even distribution between the groups, and methods such as propensity matching to mitigate the effects of confounders, which we were not able to do. We were also unable to examine pre-injury living status and environment for all patients, which may influence the way we interpret our discharge disposition results. This study used a registry that can lend itself to inaccuracies based on user error in coding. For example, our relatively high rate of non-operative treatment (19.5% overall), though possible, may be falsely inflated due to this limitation. We also determined discharge disposition based on the available codes and were unable to describe post-injury discharge environment in granular fashion. Therefore, we recognize that our definition of a “higher level care environment” is somewhat arbitrary. Similarly, the use of a registry made it difficult to determine specific information regarding our bone health variables such as timing of bone health referral, type of osteoporosis medication, diagnosis of osteopenia vs osteoporosis, etc. Finally, the study was conducted in 1 healthcare system in a single metropolitan area, thus impacting the generalizability of our results.
Conclusions
Although hip fracture outcomes between PD and non-PD patients were similar, differences between the groups were identified. These differences could inform best practices for prevention and treatment of hip fractures in PD patients. Future efforts should focus on optimizing and facilitating bone health screening and follow-up, as well as post-injury care coordination and multidisciplinary involvement, for PD patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Lisa K. Schroder MBA is a paid consultant for Exactech, Inc. and Synthes. Julie A. Switzer MD is a committee member for the American Academy of Orthopaedic Surgeons (AAOS), the American Orthopaedic Associations (AOA), and the International Geriatric Fracture Society (IGFS). She is also on the editorial board of Geriatric Orthopaedic Surgery & Rehabilitation. All other authors reported no disclosures or conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.