
Abstract
Introduction:
Proximal humerus fractures (PHF) constitute the majority of the most common osteoporotic fractures. Bone density measurements can affect treatment methods and outcomes. This study was aimed to investigate the effect of osteoporosis values, measured from direct radiographs, on fracture type, surgical outcomes.
Methods:
248 patients over 50 years of age who presented to Mersin City Hospital between 2017 and 2020 with proximal humeral fractures were retrospectively evaluated. The age and gender of the patients and the fracture types were evaluated according to the AO classification system from the direct radiographs obtained at the time of admission were recorded. The Tingart cortical thickness and deltoid tuberosity index (DTI) measurements were used to assess osteoporosis status in all patients. Postoperative and follow-up radiographs of 45 patients, treated with fixed-angle proximal humeral locking plate, were evaluated for radiographic results and their correlations with osteoporosis measurements were examined.
Results:
According to the demographic characteristics of the patients, 171 patients were female and 77 patients were male (F/M: 3/1), and mean age was 69.2 ± 11.66 (50-95). Considering the bone quality parameters in all patients, the mean Tingart value was 5.8 ± 1.6 mm and the mean DTI was 1.43 ± 0.17, where there was a correlation between the Tingart value and DTI (r = 0.810 and p < 0.001). Although there was a statistically significant relationship between the osteoporosis parameters and age and gender (p < 0.001 and p = 0.023, respectively), main AO fracture types were not related to osteoporosis (p < 0.05). In the operated group (n = 48, 19%), 19 patients (42%) showed poor outcomes, which were not associated with age and osteoporosis parameters.
Conclusion:
This study was concluded that osteoporosis parameters differ between genders and age groups in patients with PHF, however osteoporosis is not the main factor affecting the fracture type and surgical outcomes.
Introduction
Proximal humerus fractures (PHF) account for 6% of all fractures and are the third most common type of osteoporotic fracture after those in the wrist and hip. 1,2 These fractures are associated with low bone mineral density (BMD) and increase in incidence after the age of 50 (3). Osteoporotic fractures range in incidence from 40–50% in women to 13–42% in men over a human lifetime. 3 PHF incidence increases in parallel with the increasing mean age of a country’s population. The improved general state of the elderly population’s health as a result of advancements in health practices has lead to a change in the epidemiology of fractures. This is set to result in an increase in the incidence of osteoporotic fractures in the elderly population and an increase in the related treatment costs. New approaches will therefore be necessary in the future when it comes to osteoporotic patients. 4,5
PHF are more commonly observed in older women following low-energy trauma, and exhibit a specific radiological pattern. They manifest with metaphyseal and tubercle fragmentation, impacted fragments, and inferior subluxation of the humeral head. This radiological pattern can be determined through the use of 2-dimensional plain radiographs. 4
In patients with PHF, the extent of osteoporosis can be determined from direct radiographs obtained to identify the fracture pattern, as well as BMD measurements. The relationship between cortical thickness and BMD was first demonstrated by Barnett and Nordin in metacarpal bones. 6 Tingart et al. showed that osteoporosis can be determined by measuring the cortical thickness of the humerus. 7 Moreover, Mather et al. demonstrated that the cortical thickness of the proximal humerus correlates with BMD measurements, which also correlate with proximal femur BMD measurements. 8 Similarly, Spross et al. described the deltoid tuberosity index (DTI) and mentioned that it was the simplest way of demonstrating the presence of osteoporosis in the proximal humerus. 9
This study will investigate the effect that the extent of osteoporosis had on fracture patterns and clinical outcomes in patients who presented to our hospital with PHF after low-energy trauma.
Methods
The study retrospectively evaluated 338 adult patients aged over 50 who were treated for PHF at Mersin City Training and Research Hospital between February 2017 and April 2020. Patients who had suffered PHF due to high-energy trauma (n = 42) were excluded from the study. The radiographs of the remaining 296 patients were evaluated. Patients who had PHF with diaphyseal extension (n = 4), those with pathological fractures (n = 7), patients with radiographed fractures that did not allow for radiographic measurement (n = 17), those who had concomitant PHF and ipsilateral humeral shaft fractures (n = 2), and patients who were followed up for less than 21 days (n = 18) were excluded from the study. The study therefore included 248 patients who received conservative and surgical treatment. Displacement of more than 5 mm between the fracture fragments, varus/valgus malalignment of more than 40 degrees, 3-part and 4-part PHF, and an inability to achieve closed reduction were accepted as surgical criteria. Of the 48 patients who received surgical treatment, 45 patients were treated with open reduction and internal fixation using a fixed-angle proximal humeral locking plate. Two patients underwent hemiarthroplasty and 1 patient underwent reverse shoulder replacement due to a head split fracture and non-reconstructable tuberosities with poor bone stock. These patients (n = 3) who were surgically treated with arthroplasty were not included in the outcomes. The patients’ data were accessed via the hospital’s electronic data system and the patient files were examined. The Constant scores of the osteosynthesis group were calculated by contacting the patients.
The patients’ demographic data (age and sex) were recorded. Proximal humerus bone quality was calculated radiologically using the method described by Tingart et al. and the DTI. 7,9 Patients with a Tingart measurement value below 6 and DTI value below 1.4 were considered osteoporotic. 8,9 The relationship between the demographic data and radiological bone quality parameters was determined. Fractures were classified as type 11A, 11B, and 11C according to the AO fracture classification system. The relationship between fracture types and bone quality parameters (Tingart and DTI) was then investigated.
Patients who underwent surgery and completed clinical follow-up were questioned about their outcomes in order to evaluate the relationship between poor radiological outcomes and Tingart and DTI measurements. Direct radiographs were evaluated in patients who underwent osteosynthesis with fixed-angle locking plates to mend a PHF. Patients who exhibited reduction loss, secondary fragment dislocation, displacement, greater tubercle dissociation, and valgus impaction were considered to have had poor radiological outcomes. Patients who exhibited union and no avascular necrosis were considered to have had good radiological outcomes. 10 Patients who received surgical treatment were assigned to either Group 1 (good radiological outcome) or Group 2 (poor radiological outcome). Patients treated with plate osteosynthesis were evaluated using the Constant Shoulder Score for around 18 months on average (8–34 months).
Statistical Analysis
The data were analyzed with SPSS 22 software compatible with Windows. Values were provided within a 95% confidence interval. Data were recorded as percentages, arithmetic means, and standard deviation values. The distribution of the evaluated values was in the normal range according to the Kolmogorov-Smirnov test. Spearman’s correlation analysis was used to evaluate the correlation of osteoporosis parameters. In the evaluation of correlation coefficients, r: 0–0.24 was considered a poor correlation, r: 0.25–0.49 a moderate correlation, r: 0.5–0.74 a strong correlation, and r: 0.75–1 a very strong correlation. The age and sex of all patients and the bone quality parameters of the group who underwent surgery were compared using the Mann–Whitney U test. The Kruskal–Wallis test was used to compare the subgroups created according to the AO classification system. The Mann–Whitney U test was used to compare good and poor outcomes in patients who underwent surgery. p < 0.05 was considered statistically significant.
Results
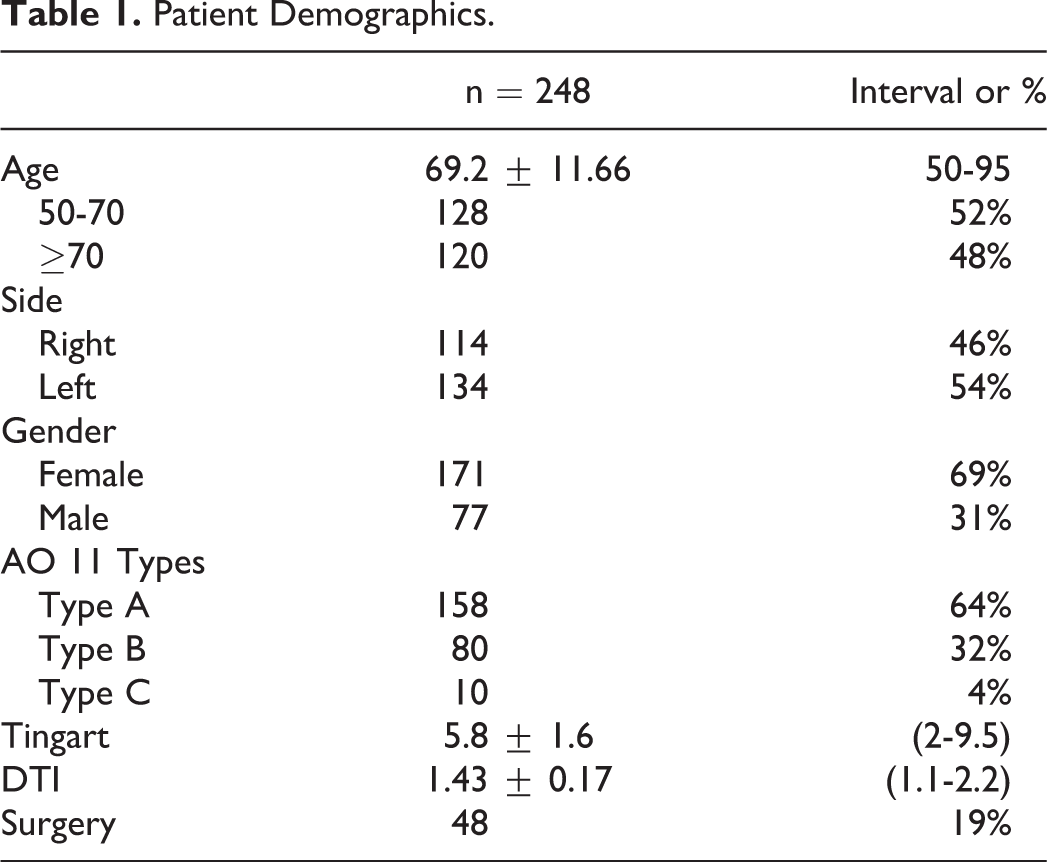
The mean age of the patients was 69.2 ± 11.66 (50–95), 171 patients were female and 77 were male (F/M: 3/1). The mean follow-up period was 4.8 months, with a minimum of 21 days and maximum of 2.8 years. The frequency of fractures according to age interval is presented in Figure 1. When evaluated according to the AO classification system, 64% of the fractures were type 11A, 32% were type 11B, and 4% were type 11C (Figure 2). The distribution of patient demographics is shown in Table 1 through frequency and percentage values.
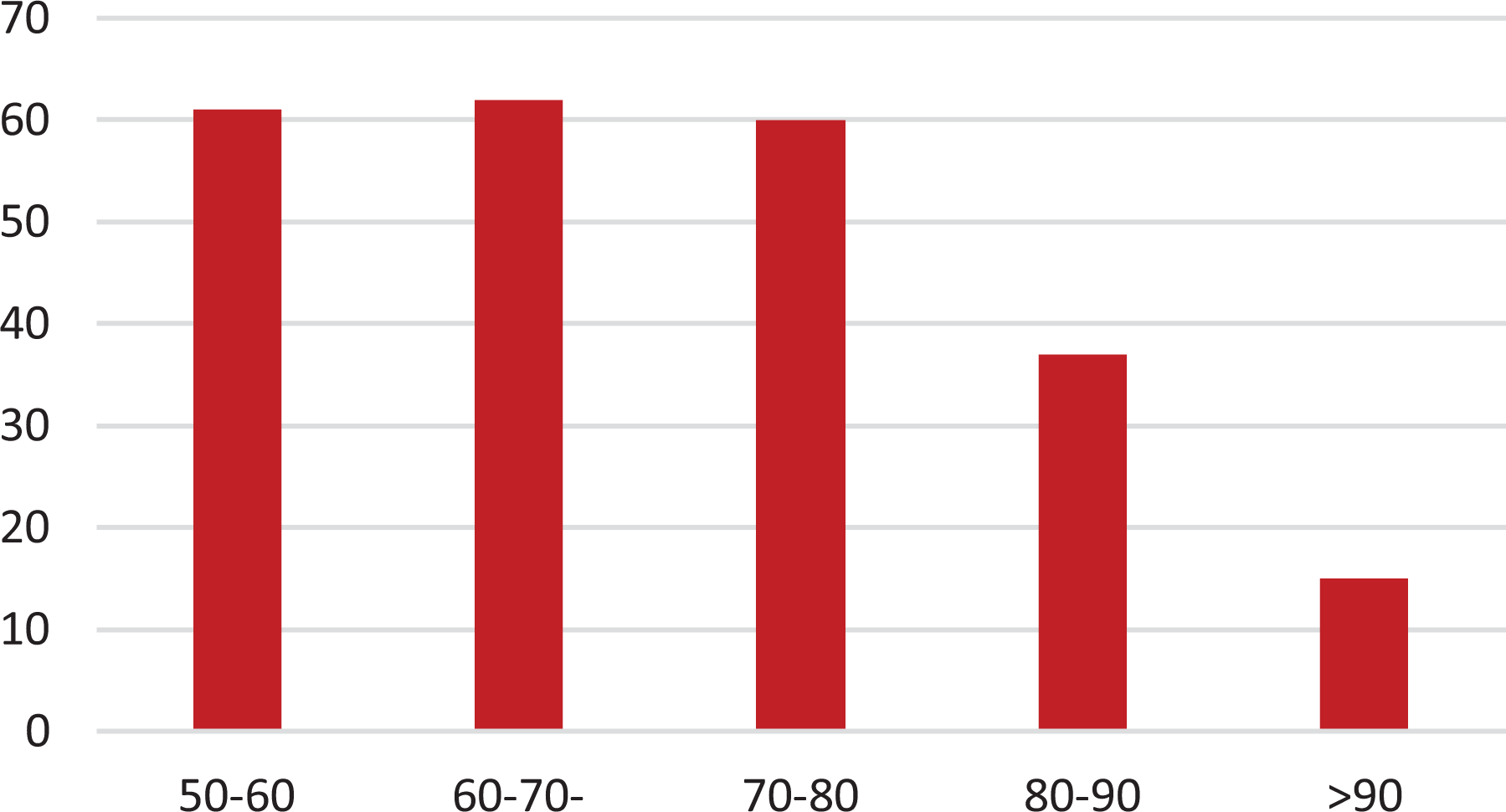
Incidence of fractures according to age interval.

AO classification location: 11 Types.
Patient Demographics.
When the osteoporosis evaluation parameters (Tingart and DTI) are considered in all patients, the mean Tingart value was 5.8 ± 1.6 mm while the mean DTI value was 1.43 ± 0.17. There was a correlation between Tingart and DTI values in all age groups (r = 0.810 and p < 0.001). The distribution of the Tingart and DTI values is presented in Figure 3.
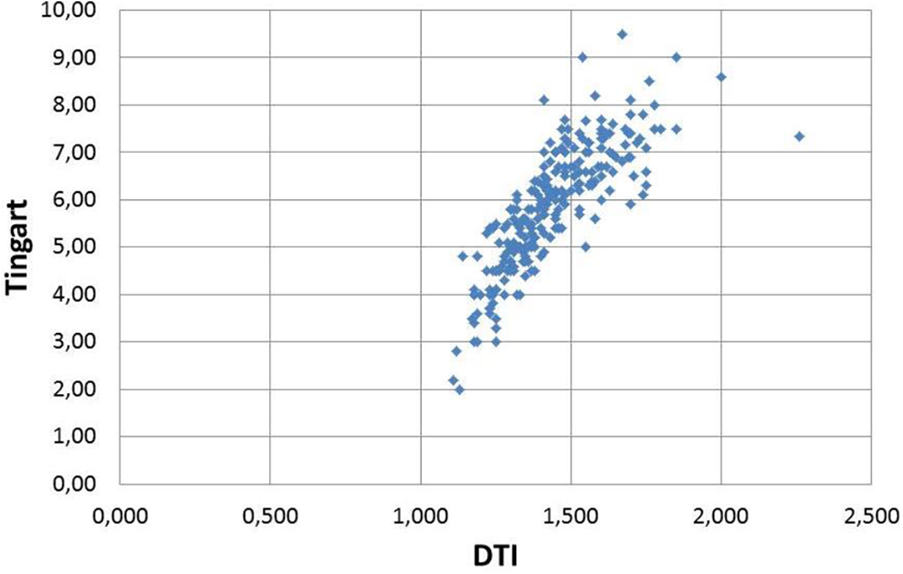
Distribution of the Tingart and DTI parameters.
There was a statistically significant difference between the sexes and age groups (ages 50–70 and over 70) in terms of their osteoporosis evaluation parameters (p < 0.001 and p = 0.023, respectively) (Table 2). However, no statistically significant difference was observed between the main AO fracture types in terms of the osteoporosis evaluation parameters (Table 3).
Comparison of Tingart and DTI Values With Age, Sex, and Use of Surgery.

Bone Quality Parameters According to the AO 11 Types.

Nineteen patients (42%) exhibited poor outcomes in the group that underwent plate osteosynthesis (n = 45). There was no statistically significant relationship between poor surgical outcomes and age and the osteoporosis evaluation parameters (Table 4).
Comparison of Poor and Good Radiological Outcomes in the Group That Underwent Surgery.

The Constant score of patients treated with plate osteosynthesis was 70.2 ± 15.4 (32–92). However, the Constant score for Group 1 was 76.8 ± 5.5 (66–92), while it was 57.2 ± 8.7 (36–72) for Group 2. There was a statistically significant difference between poor surgical outcomes and good surgical outcomes according to the Constant scores (p < 0.001).
Discussion
Osteoporosis can be defined as decreased bone quality and density, which leads to an increased risk of fracture. This reduction in bone quality results in a fragile bone structure, which can complicate surgical treatment. The decrease in bone mass and osteoporotic changes increases the risk of fractures in the vertebral bodies, distal radius, proximal femur, and proximal humerus, especially in the elderly population. 7
The most reliable methods used in clinical practice to evaluate osteoporosis in the femur, spine, and radius are dual energy X-ray absorptiometry and peripheral quantitative CT. 7 The presence of osteoporosis is a parameter that can change the treatment plan in patients who present to a hospital with PHF. Therefore, any method that can be easily used to test a patient’s bone quality could provide an advantage in clinical practice. Proximal femur and lumbar vertebral body measurements are routinely used in the diagnosis of osteoporosis in the clinical setting. However, these measurements may not accurately reflect the quality of upper extremity bones with different loading parameters. 11,12 Studies have been conducted to evaluate the presence of osteoporosis in the upper extremities, and it has been demonstrated that cortical thickness of the proximal humerus is associated with osteoporosis. 7 -9 In a study by Spross et al., it was shown that there was a correlation between the Tingart and DTI measurements and the BMD values of the proximal humerus as measured by peripheral quantitative CT. 9
In their study, Tingart et al. showed that the mean cortical thickness measurements were significantly different, especially in individuals over and under 70 years of age, and that these results correlated with the BMD measurements of the proximal humerus. 7 Similarly, our study also yielded significantly different results in patients aged 70 and over who had PHF. Measuring the mean cortical thickness may be useful in diagnosing osteoporosis and planning the treatment in patients with PHF, without the requirement for other methods. In Tingart’s study, there was no difference between the sexes in terms of cortical thickness measurements. However, our study showed a statistically significant difference between the sexes in patients over 50 who had PHF. This supports the literature, which says that the rate of osteoporotic humerus fractures is higher in women compared to men. 2
Conservative and surgical treatment methods can be used in the treatment of osteoporotic PHF. Among said surgical methods, fragment-specific fixation, the use of fixed-angle locking plates, antegrade nailing, and arthroplasty are the most commonly preferred. 10 There are studies showing that decreased bone quality may have a negative impact on the outcomes of PHF surgery. 13 -18 In a cadaveric study by Frankhauser et al., it was shown that low BMD values had a negative effect on stability in patients who underwent open reduction and internal fixation. 18 In another study by Krappinger et al., failed surgical fixation in patients with PHF was attributed to age, sex, BMD, insufficient medial cortical support, and anatomical reduction. Insufficient anatomical reduction was found to be the leading cause of failure. The BMD of the proximal humerus region was also found to be associated with surgical failure. 16 On the other hand, the rate of mechanical failure was 35% in patients who underwent surgery for PHF in Kralinger et al.’s study. However, the study did not demonstrate a relationship between failure and osteoporosis, and the causes of failure were reported to be insufficient anatomical reduction and medial cortical support, age, and sex. 10
In a study comparing the results of conservative treatment with the use of proximal fixed-angle locking plates in 3- and 4-part PHF, the surgical complication rate was found to be 56%. 19 Similarly, a meta-analysis by Li et al. was unable to demonstrate the superiority of open reduction and internal fixation over conservative treatment in 3- and 4-part PHF. 20 In our study, 45 patients who were treated with fixed-angle locking plates for PHF were evaluated in terms of the effect that osteoporosis had on their radiographic results. In the group that underwent surgery, 42% of the patients exhibited poor outcomes. However, there was no difference between those who had poor and good radiological outcomes in terms of their osteoporosis evaluation parameters. There was a correlation between the radiological outcomes and Constant scores of patients who underwent plate osteosynthesis. The poor outcomes mentioned may result from the complexity of fracture patterns, the surgical technique, and non-compliance with follow-up in patients who were treated with plates.
Unlike other studies in the literature, in the present study low-energy PHF in patients aged over 50 were classified according to the AO classification system. It was observed that most of the fractures were AO type 11A and 11B (63.7% and 32.2%, respectively), and that complex intra-articular fractures (AO Type 11C) were rarely associated with low-energy traumas. However, it was concluded that osteoporosis evaluation parameters did not have an effect on the type of fracture identified according to the AO classification system.
The weakness of this study is that the clinical outcomes between patients with PHF who received conservative treatment and those who underwent surgery could not be compared. Similarly, inclusion of the clinical outcomes would enhance the reliability of the study. Checking the intra-observer and inter-observer reliability for cortical thickness measurements taken from direct radiographs would also enhance the reliability of measurements.
Conclusion
In this study, it was concluded that osteoporosis parameters vary between the sexes and age groups in patients over 50 who have low-energy PHF, but that osteoporosis is not the main factor affecting fracture type and surgical outcomes. This study also showed the presence of a strong correlation between Tingart cortical thickness measurements and DTI values, which is consistent with the literature.
Footnotes
Abbreviations
Proximal humerus fractures: PHF
Bone mineral density: BMD
Deltoid tuberosity index: DTI
Computer tomography: CT
Authors’ Note
All authors contributed to the work and accepted the final version. AT collected, analyzed and interpreted data, and wrote the manuscript. AG and KU supervised in data analysis and interpretation, and contributed with preparing the finalized manuscript. YUY designed the study, contributed with disease-specific knowledge and data collection, and revised the manuscript. The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. Our study was ethically approved by the Our Hospital Local Ethical Committee. The study was conducted in accordance with the principles of the Declaration of Helsinki. All participants signed informed consent, except in the 5 case where a participant was indicated by their doctor to have impaired ability to consent, in which cases a proxy signed on their behalf.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.