
Abstract
Purpose
To investigate the effects of age on the clinical, functional, and radiographic outcomes of patients with proximal humerus fractures treated operatively with locking plates.
Methods
Between February 2003 and July 2012, all patients who sustained a proximal humerus fracture who presented to our institution were enrolled into a database. Patients were followed up at 1, 6, 12, 26, and 52 weeks postoperatively with physical examination and radiographs. Validated functional outcomes scores were collected at 6 and 12 months. Complications were recorded as they occurred. Statistical analysis was conducted to assess for functional, physical, or radiographic differences between patients age younger than 65 and patients age 65 or older.
Results
Of the 147 consecutive patients treated operatively for a proximal humerus fracture, 115 (78%) patients with an average follow-up of 16 months met the inclusion criteria for this study. The young cohort (patients < 65) included 70 patients with an average age of 53, whereas the elderly cohort (patients ≥ 65) included 45 patients with an average age of 73. The older cohort had significantly more women (P = .04), but there was no statistical difference in fracture type between the age groups. There were no differences in the radiographic measures of screw penetration, humeral head height, and neck-shaft angle between the age groups. There were no differences in physical examination scores between the age groups. There were no significant differences in functional outcomes or complication rates between the age groups.
Conclusion
Treating proximal humerus fractures operatively with locked plates can overcome the challenges of poor bone quality that often occur with increasing age. Age should not play a significant role in the decision-making process for treating proximal humerus fractures that would otherwise be indicated for surgical fixation.
Introduction
As the number of elderly persons in the United States increases so will the incidence of osteoporotic fractures among this population. 1 According to the department of Health and Human Services, there are an estimated 1.5 million osteoporotic fractures per year. 2
The proximal humerus has been traditionally considered an anatomic area prone to osteoporotic fracture following low-energy trauma in the elderly patient, and as the population continues to age, there will likely be an increase in the incidence of these fractures. 3 Operative fixation of these fractures has been historically challenging due to poor bone quality that can lead to inadequate screw purchase and to the failure of internal fixation constructs. In addition, the concern for the development of osteonecrosis and the need for subsequent surgical intervention have lead some to advocate for arthroplasty in this patient set. The advent of locking plate technology offers an innovation beyond conventional compression plating in the fixation of osteoporotic bone: the plate acts as a fixed-angled construct and converts shear stress to compressive stress at the screw–bone interface. 4
To date, there have been no studies that have compared the functional outcomes of surgically treated proximal humerus fractures in older versus younger cohorts using standard modern fixation techniques. The purpose of this study was to compare the functional outcomes of proximal humerus fractures treated with a locking plate implant and a standard surgical technique in patients younger than 65 years to those 65 years and older.
Materials and Methods
This is an institutional review board approved study of patients who sustained a proximal humerus fracture and were treated with open reduction and internal fixation with a locking plate. Between February 2003 and December 2012, patients who presented to our academic medical center with displaced proximal humerus fractures treated with open reduction internal fixation were enrolled into a prospective database. This database included initial injury films retrospectively acquired from the medical record, demographic information collected from the patient at time of enrollment, and prospectively collected radiographic, physical examination, and functional data collected at all follow-up intervals. Fractures were classified by the Neer classification and the Orthopedic Trauma Association’s (OTA) Compendium classification. 5,6 Indications for surgical intervention were made by the treating surgeon and based upon a number of factors including radiographic imaging, physical examination, and level of function. Patients were included in the study if they were older than 18 years of age and had an acute fracture of nonpathologic origin.
Following study enrollment, a trained interviewer obtained baseline information that included patient demographics such as age, gender, date of fracture, and type of fracture. Operative data including patient position, length of surgery, blood loss, number of screws utilized, and intraoperative complication were extracted from the hospital record following the procedure. Patients were followed up at regular time intervals by their surgeon of record. Functional status was recorded by a trained interviewers at 3-, 6-, and 12-month follow-up intervals using the Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire. 7 The DASH is a 30-item validated outcome questionnaire that measures upper extremity disability on the basis of physical function and symptoms. Interviewers were trained to administer surveys by the principal investigator of this study. Interviewers were not aware that the information garnered from the surveys would be used to compare patients on the basis of age.
All surgeries were performed under the supervision of 1 of 5 fellowship trained shoulder or trauma surgeons. The patient was place in the beach chair position, and open reduction and internal fixation of the fractures were performed through a deltopectoral approach. Nonabsorbable sutures placed through the rotator cuff tendons adjacent to the displaced tuberosity fragments (if present) were used to indirectly mobilize the fracture fragments. The humeral head was elevated and reduced through a lateral cortical window, followed by filling of the void with either cancellous chips or calcium phosphate cement at the discretion of the treating surgeon. After reduction in the head and tuberosities, the locking plate was applied just lateral to the bicipital groove on the humeral shaft.
Proximal locking screws were placed in a unicortical fashion with the aid of an external guide into the humeral head and confirmed with intraoperative fluoroscopy. Screw placement was verified with anterior–posterior (AP; internal and external rotation) views and axillary views to ensure that the screws were not intra-articular. The distal portion of the plate was then fixed to the distal humeral shaft with a combination of locked and nonlocked bicortical screws. Finally, to further secure the fixation construct, the nonabsorbable braided sutures were tied down to the plate following plate and screw placement.
The postoperative physical therapy protocol was standardized as follows: isometric deltoid, bicep, and triceps strengthening were begun immediately on the first postoperative day along with active range of motion of the elbow, wrist, and hand. Patients were placed in a sling and were encouraged to start early passive range of motion (PROM) exercises of the shoulder. The PROM exercises were continued for the first 4 to 6 weeks postoperatively until radiographic evidence of fracture healing. Patients then began active range of motion exercises in a formal physiotherapy program.
Patients were then seen for follow-up examination at a minimum of 1, 6, 12, 26, and 52 weeks postoperatively. All patients were examined by their treating surgeon and an independent researcher to determine the active range of motion, level of pain, and discomfort, functional status, and evaluation for the development of a complication. Patients also underwent standard shoulder trauma radiographs: AP, scapular Y, and axillary views to evaluate their fractures. These radiographs were obtained preoperatively, intraoperatively, and at follow-up visits (1, 6, 12, 26, and 52 weeks) to evaluate for fracture healing, hardware position, anatomic alignment, and to identify evidence of postoperative osteonecrosis.
Trained research personnel analyzed all radiographs including neck-shaft angle, length of the implant, average screw distance from the articular surface, and humeral head height. The neck-shaft angle was based on the description by Agudelo et al, in which a line was drawn from the superior border to inferior border of the articular surface. 8 A second line was then drawn perpendicular to the first and through the center of the humeral head. The angle created by this line and the line bisecting the humeral shaft were measured as the neck-shaft angle. Length of the implant was measured as the vertical distance from the most proximal to the distal edge of the plate. Radiographic magnification was standardized for each measurement based on the ratio of the measured implant length to the standard implant length. Two types of implants were utilized during the course of this study, one (Synthes, Paoli PA) measuring 90 mm in length was used in all patients prior to January 2010 and another (Exactech, Gainsville, Florida) measuring 80 mm in length was used in all patients beginning in January 2010. Both implants used exclusively fully threaded locking screws. Humeral head height was based on the description by Gardner et al and was determined by drawing a vertical line along the shaft of the plate and then drawing 2 lines perpendicular to it, one at the superior aspect of the humeral head and the other at the top edge of the plate. 9 The distance between these 2 perpendicular lines was measured as the humeral head height. On AP radiographs, the screw tip measured to be nearest to the glenohumeral joint along the screw’s axis was used to determine the screw tip to articular surface distance and was deemed the reference screw for subsequent radiographic measurements. The same reference screw tip to articular surface distance was measured at each follow-up visit to assess for humeral head settling or collapse. Patients with screws penetrating the articular surface were assigned a screw distance of zero.
Statistical Analysis
Differences in demographic characteristics were assessed between patients younger than 65 years old to those 65 years and older with use of Fischer exact test or chi-square test for categorical variables and the Mann-Whitney U test for continuous variables, none of which were normally distributed. A P value of <.05 was considered significant.
Patients
Of the 147 consecutive patients treated for a proximal humerus fracture with operative fixation at our institution, 115 patients (37 men, 78 women; 78%) with an average 16-month follow-up met the inclusion criteria and were included in the study (Table 1). Twenty-nine patients were excluded because they had less than 6 months of follow-up. The excluded patients had similar mean DASH scores at 3 months to those included in the study (31 vs 33). In 115 adult patients, 115 acute fractures were identified; 70 patients were aged less than65 and 45 patients were aged 65 or older. The average age in the less than 65 group was 53, and the average age in the 65 and older group was 73. Based on the Neer system, there were 25 (22%) 2-part fractures, 68 (59%) 3-part fractures, and 22 (19%) 4-part fractures. Significantly more women were found in the older cohort than younger cohort. There were 42 females and 28 males were in the younger cohort, while 36 women and 9 males were in the older cohort (P = .04).
Demographic Data of Age Cohorts.a

a P values denote statistical differences between the age cohorts.
Results
Patients under the age of 65 had an average active forward elevation of 137.4°, while patients 65 and older had an average active forward elevation of 125.9° (Table 2). Patients younger than the age of 65 had an average passive forward elevation of 148.9°, while patients aged 65 and older had an average passive forward elevation of 140.9°. Active and passive forward elevations were not significantly less in the older cohort than in the younger cohort (P = .09, P = .08, respectively). In addition, patients under the age of 65 had an average external rotation of 46.9°, while aged patients 65 and older had an average forward elevation of 41.9°; external rotation was not significantly less in the older cohort than in the younger cohort (P = .15). There was no difference in complication rate (P = .83), OTA fracture type (P = .98), or number of screws inserted in the humeral head (P = .45). Patients aged 65 and older had fewer Neer 4-part fractures than patients younger than age 65 (Table 1). The DASH scores between age groups showed lower function in patients aged 65 or older, but the difference between the groups was not significant (P = .07).
Radiographic assessment demonstrated that all the fractures united by 3 months after surgery. Of the radiographic parameters analyzed (neck-shaft angle, screw distance, and humeral height), no parameter was found to be different (Table 2). Patients under the age of 65 had an average neck-shaft angle of 132.5°, while patients aged 65 and older had an average neck-shaft angle of 129.3° (P = .66). Patients under the age of 65 had an average screw distance of 3.8 mm, while patients aged 65 and older had an average neck-shaft angle of 3.1 mm (P = .10). Patients under the age of 65 had an average humeral head height of 14.1 mm, while patients aged 65 and older had an average humeral head height of 13.4 mm (P = .60).
Outcome Measurements and Results.a
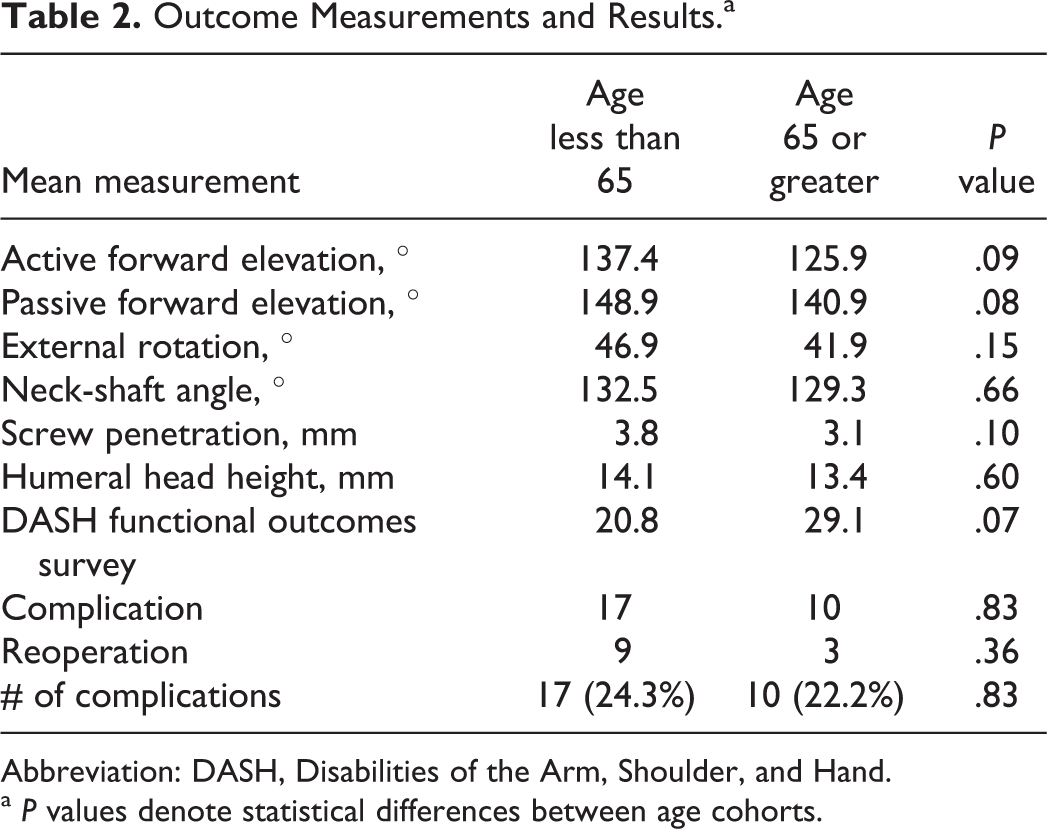
Abbreviation: DASH, Disabilities of the Arm, Shoulder, and Hand.
a P values denote statistical differences between age cohorts.
Discussion
The management of displaced proximal humerus fracture can be challenging, especially in the elderly patient due to issues with poor bone quality. Locking plates have gained popularity in operative treatment of these fractures, but it is not clear whether this device results in better outcomes. The purpose of our study was to determine whether there are differences in functional and radiographic outcomes between elderly and younger patients treated with locked plating.
Poor bone quality in elderly patients has often been cited as a factor that makes the operative treatment of proximal humerus fractures in this cohort difficult. Decreased bone density can result in poor screw purchase and failure of the internal fixation construct. Barvencik et al has used histomorphometric analysis to examine the microarchitecture of the proximal humeri of cadaveric specimens and found that women older than 60 years have a significant loss of bone mass in the medial and lateral regions of the humeral head compared to women younger than 40 years of age.
These observations are important, because it suggests that the relatively decreased bone mass in the lateral region of the humeral head represents a structural weakness that might explain the high incidence of avulsion fractures of the greater tuberosity. His group also found that the most superior and medial region of the humeral head had the highest bone mass. This finding correlates with pullout studies by Liew et al which determined that screw fixation was strongest in this area, subchondrally in the center of the humeral head perpendicular to the anatomic neck. 10,11
In our review of the literature, we found few studies that examined the functional results of elderly patients treated with locked plating for displaced proximal humerus fractures. Some investigators have found that locked plating can be advantageous for osteoporotic bone. Siwach examined 25 patients with osteoporosis with a mean age of 62 treated with locked plating. He found that 92% of the patients in this series had good to excellent outcomes. However, those with grade IV osteoporosis had the highest average Constant-Murley scores. 12 Another recent series by Shi et al studied the management of proximal humeral fractures in elderly patients with uni- or polyaxial locking osteosynthesis systems. In this series of 76 patients with a mean age of 68.8 years, the authors found that satisfactory outcomes were achieved in 73.7% and 75.0% of the patients, respectively. 13
Olerud et al randomized elderly patients with 3-part proximal humerus fractures to internal fixation with a locked plate or nonoperative treatment. They found that locked plating resulted in better function and quality of life compared to nonoperative treatment. They also found, however, that operative treatment is not without complications. In their series of 60 patients with a mean age of 73.9 years, 13% of the patients had a severe complication requiring a major reoperation, and 17% had a minor secondary surgical intervention.
Our study shows that there is no significant functional difference in terms of DASH scores between younger and older age groups (younger than 65 vs 65 and older). Although our older cohort trended toward worse functional outcomes, we believe this trend was primarily due to preinjury functional status in the elderly cohort rather than injury-associated limitations. Although range of motion was found to be marginally superior in the younger group in terms of forward elevation and external rotation, it was not significantly different between the groups. We also found that radiographic outcome measures of neck-shaft angle, humeral height, and screw distance were similar between the groups. This suggests that poor bone quality may not considerably impact the efficacy of locked plates. Limitations of this study include the lack of a nonoperative comparison group and a moderate sample size, which limited our ability to stratify outcomes by decades. Patients 65 and older had fewer Neer 4-part fractures than younger patients, which may have lessened the complication rate in the older cohort in comparison to the younger cohort. The determination of age cutoff in this study may also be considered a limitation. This cutoff was chosen, because age 65 is commonly considered the age at which an individual is designated as a “senior citizen.” However, this cutoff seems reasonable in line with the available literature on proximal humerus fractures in the elderly patient. Finally, a further limitation of this study was the fact that indication for surgical treatment and the use of a locking plate was at the discretion of the treating surgeon. We did not include patients that underwent arthroplasty or other forms of fixation in our analysis. 14 Despite these limitations, our study shows that elderly patients with proximal humerus fractures have functional and radiographic outcomes that are comparable to their younger counterparts. These findings suggest that treating proximal humerus fractures operatively with locked plates can overcome the challenges of poor bone quality that often occurs with increasing age. Age alone should not play a significant role in the decision-making process for treating proximal humerus fractures that would otherwise be indicated for surgical fixation. Many older adults continue to live dynamic lives well past the age of retirement and should be treated based on their overall health and activity level rather than their age or bone quality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.