
Abstract
Introduction
It is appealing to accurately predict postoperative delirium (POD) before surgeries. In this study, it was hypothesized that a novel electroencephalogram-derived index, the delirium index (DELi), could extract latent information regarding the predisposing factors of POD preoperatively. This study was aimed at developing a concise model that incorporated this DELi score to predict the early POD of elderly patients after hip surgeries.
Materials and Methods
Elderly patients scheduled for elective hip fracture surgeries were prospectively enrolled in a tertiary care hospital from November 2020 to June 2022. DELi scores and patient characteristics (age, sex, types of fracture and surgery, the time interval between fracture and surgery, cognitive function assessed using the Montreal Cognitive Assessment (MoCA), and frailty status assessed using the FRAIL scale) were collected preoperatively as candidate predictors. POD diagnosed using the confusion assessment method (CAM) was the outcome. Least absolute shrinkage and selection operator (LASSO) regression analysis was used to select predictors. Then, these predictors were entered into a backward logistical regression analysis to develop a prediction model. Discrimination, calibration and clinical utility were validated using the bootstrapping method.
Results
All data (144 qualified patients of 170) were used for development. POD was observed in 71 patients (49.3%). Preoperative DELi scores predicted early POD (the area under the curve (AUC) = .786, 95% confidence interval (CI): .712, .860, in internal validation). A nomogram with MoCA, FRAIL scale and DELi score was constructed with excellent discrimination (AUC = .920, 95% CI: .876, .963, in internal validation), accredited calibration (P = .733, Hosmer‒Lemeshow test), and a wide range of threshold probabilities (5% to 95%).
Conclusions
Preoperative DELi scores predicted the early POD of elderly patients after hip surgeries. A concise prediction model was developed and demonstrated excellent discrimination.
Keywords
Key Messages
The accurate prediction of POD before surgeries is the premise of adopting an integrated perioperative strategy for delirium risk reduction from preoperative stages.
The preoperative DELi, a novel electroencephalogram-derived index based on a wavelet algorithm, predicted early POD in elderly patients after hip surgeries.
A concise model with excellent discrimination (AUC >.9) and a wide range of threshold probabilities (5% to 95%) of yielding more net benefits was developed for predicting the early POD of elderly patients after hip surgeries.
Introduction
As the most frequent postoperative complication in old patients,1–4 postoperative delirium (POD) may cause prolonged hospital stays, dementia, and increased morbidity and mortality. 5 Preventing POD in the elderly is of high priority. Currently, risk evaluation and perioperative risk reduction are the most effective ways of managing POD. 6 An accurate and timely prediction model is the premise of implementing prevention measures early. However, an extensive list of POD risk factors distracts doctors and it is challenging to complete complex neuropsychological evaluation in routine practice. Moreover, variables during and after surgeries are generally included in present POD prediction models.7,8 That impedes the implementation of delirium risk reduction interventions from the preoperative stages. A concise model using only data available before surgeries is more rational and pragmatic. 9
Electroencephalography (EEG) has been used to assess delirium for decades. 10 Intra-operative frontal α-band power was demonstrated to be associated with POD in cardiac surgeries. 11 Recently, the entire frequency band EEG was analyzed by developing a wavelet analysis method.12,13 Based on this wavelet algorithm, a series of specific changes in EEG were identified when delirium occurred. These dynamic variations of EEG parameters attributable to delirium were integrated into a real-time index named the delirium index (DELi ranging from 0-100 and positively associated with the probability of delirium). This novel DELi score could be easily attained via a wavelet algorithm multifunction monitor (Beijing Easymonitor Technology Co., Ltd., Beijing, China) and was considered to be related to delirium-associated cognitive status. 14
Preoperative cognitive status is the leading predisposing factor for POD. 11 A preoperative DELi score is plausible to measure baseline cognitive status and identify brain vulnerability to delirium. The identification of patients at high risk of POD before surgeries is conducive to adopting an integrated perioperative strategy for preventing POD from the very beginning. This DELi score was used for developing a concise model to preoperatively predict POD in elderly patients.
Materials and Methods
Study Design
This prognostic study was conducted to develop a multivariable model to predict the early POD of elderly patients after hip surgeries. A prospective longitudinal cohort was designed to consecutively enroll elderly patients in a tertiary care hospital from November 2020 to June 2022. The follow-up of all participants continued until postoperative day 2.
Registered at the China Clinical Trials Registry Platform (ChiCTR2200060389), this study gained the approval of the Institutional Review Board of Beijing Jishuitan Hospital (approval number (No.): 202102-11). The written informed consent of all participants (or their statutory guardians when they were incapacitated to consent) was obtained. This manuscript followed the transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD) statements.
Participants
Elderly patients (≥65 years old) scheduled for elective hip fracture surgeries were screened at Beijing Jishuitan Hospital, Beijing, China. Only those scheduled for the first procedure on the day were eligible to attenuate the potential bias caused by circadian rhythms. 15 The exclusion criteria were as follows: (a) Elderly patients refused to participate; (b) Scheduled surgeries were changed; (c) Cognitive function could not be assessed; (d) Elderly patients had a history of long-term opioid use or alcohol abuse; and (e) EEG data were unavailable. According to the instructions of the center, patients with the poor physical condition were not permitted to accept elective hip fracture surgeries. Thus, patients with the American Society of Anesthesiologists (ASA) physical status IV or V were not allowed to participate.
Patients underwent total hip arthroplasty (THA), hemiarthroplasty, cannulated screw fixation or proximal femoral nail anti-rotation (PFNA) surgeries according to fracture types and surgeons’ decisions. Before operations, all patients received routine spinal anesthesia and ultrasound-guided fascia iliaca compartment block analgesia. Routine patient-controlled intravenous analgesia was used for all the participants.
Outcome
Delirium was identified using the confusion assessment method (CAM).3,16 A trained geriatrician blind to patients’ perioperative characteristics conducted delirium assessments twice daily (08:00 and 20:00) on postoperative days 1 and 2. Early POD was diagnosed upon the identification of delirium during any of the assessments.
Predictors
DELi scores were collected by the use of wavelet algorithm multifunction monitors before anesthesia in operation rooms (see Supplemental Figure 1). They were consecutively recorded every 2 min for 20 min. Then, the median of these records was calculated as the final score. Patients stayed awake and calm without any procedures performed or drugs used until the collection of DELi scores was completed. The supplemental document details the rationale and course of calculating DELi scores.
In addition to DELi scores, patients’ clinical and demographic characteristics were collected preoperatively. These characteristics included age, sex, types of fracture and surgery, time interval between fracture and surgery, frailty status and cognitive function. The Montreal Cognitive Assessment (MoCA ranging between 0 and 30 points, where ≥26 indicates cognitive impairments) 17 was used to assess cognitive function. The FRAIL scale (0 to 5 points, where 0 indicates robust status and ≥3 indicates frail status) 18 was used to assess frailty status.
Sample Size
According to the pretest, DELi scores exhibited a sensitivity and specificity of 79% and 80% respectively in the discrimination of POD, and the incidence of POD was approximately 50%. The sample size needed was 128 when a prevalence, sample sensitivity and specificity of 50%, 79% and 80% were assumed to be for a two-sided 95% sensitivity confidence interval (CI) with a maximum width of .20, and 124 when those were assumed to be for a two-sided 95% specificity CI with equal width. With a dropout rate of 11%, 144 patients were required to verify the discrimination of POD.
Statistical Analysis
Multiple imputations were arranged for missing data. Continuous and categorical data were represented by the mean with standard deviation (SD) or median with interquartile range (IQR) and number with proportion, respectively. Least absolute shrinkage and selection operator (LASSO) regression analysis was used for obtaining a subset of predictors and running K cross-validation five times to regularize the observed items. Candidate predictors were selected using the “lambda. 1 standard error” criterion and entered a backward logistical regression analysis to develop a nomogram prediction model for predicting POD. Receiver operating characteristic (ROC) curve analysis was utilized, and the area under the curve (AUC) was calculated to determine the discrimination of the model. Internal validation was performed using the bootstrapping method (resampling = 1000). Comparisons between models were made with net reclassification improvement (NRI, cutoff = .5) and integrated discrimination improvement (IDI) indexes. R software (version 4.2.0; R Foundation for Statistical Computing, Vienna, Austria; https://www.R-project.org) was used to conduct statistical analysis, and P < .05 was considered to show statistical significance.
Results
Clinical Characteristics
In this study, 144 of 170 participants who were approached were qualified for the analysis (Figure 1). The clinical and demographic characteristics of these patients (median age [IQR], 78 [71, 85] years old; 55 (38.2%) males) are presented in Table 1. The POD of all 144 participants was assessed successfully. Early POD was observed in 71 patients (49.3%). No data were missing. No significant discomfort caused by the acquisition of DELi scores was reported by the patients. There were no severe postoperative complications in both groups. No significant difference was observed in the length of hospital stay between the participants with and without POD (5 [4,6] vs 5 [4, 5], P = .054). Flow of patients through the study. Patients’ Baseline Demographic and Clinical Characteristics. Abbreviations: POD, postoperative delirium; PFNA, proximal femoral nail anti-rotation; THA, total hip arthroplasty; MoCA, Montreal cognitive assessment; DELi, delirium index; IQR, interquartile range. Data were shown as n (%) or median [IQR].

Prediction of Early POD by DELi Scores
DELi scores per se could moderately predict early POD. The AUC of DELi scores for the prediction of early POD was .791 (95% CI: .714, .867) in the training set and .786 (95% CI: .712, .860) in the internal validation set using the bootstrap method (resampling = 1,000, see Supplemental Table 1 and Supplemental Figure 2).
Development of an Early POD-Predicting Nomogram
Data from all the participants were used to develop the model. Based on the one standard error criterion in the LASSO regression model, three potential predictors including MoCA, FRAIL scale and DELi score were chosen (Figure 2). All three candidates entered the final logistic regression model and developed a composite score for predicting early POD (Supplemental Table 1). The construction of a nomogram provided a handy tool for predicting the probability of POD (Figure 3). Selection of predictors using LASSO regression analysis with 5-fold cross-validation. (A) A coefficient profile plot was drawn against the log (lambda) sequence. (B) The parameter (lambda) selection of deviance in the LASSO regression was tuned based on minimum and 1-SE criteria (left and right dotted lines, respectively). In this study, the selection of predictors followed the 1-SE criterion, where three nonzero coefficients were chosen. LASSO represents the least absolute shrinkage and selection operator; SE represents standard error. Nomogram for predicting the probability of POD in elderly patients after orthopedic surgeries. The total points of the nomogram ranged from 0 to 268. MoCA represents Montreal Cognitive Assessment.

Performance Assessment of the Early POD-Predicting Nomogram
The AUC of this nomogram for the prediction of early POD was .922 (95% CI: .878, .965, see Figure 4(a)), and the internal validation by use of the bootstrap method (resampling = 1000) was .920 (95% CI: .876, .963, see Figure 4(b)). The accredited calibration was confirmed using the Hosmer‒Lemeshow test (P = .733, see Figure 5(a)). Based on the cutoff of .481 (the largest Youden index of the nomogram), the nomogram had a sensitivity and specificity of .859 (95% CI: .778, .940) and .877 (95% CI: .801, .952), respectively, in predicting early POD, with a positive and negative prediction value of .871 (95% CI: .793, .950) and .865 (95% CI: .787, .943), respectively (Supplemental Table 2). Discrimination of the composite-score nomogram for the prediction of POD in elderly patients after orthopedic surgeries. ROC curve of the nomogram in training (a) and internal validation sets (b) using the bootstrap method (resampling = 1000). Vertical solid lines indicate 95% CI. Calibration curve and DCA of the composite-score nomogram for predicting the POD of elderly patients after orthopedic surgeries. (a) Calibration curve in training (apparent) and internal validation sets (bias-corrected) by use of the bootstrap method (resampling = 1000). X- and y-axis represent nomogram-predicted and actual observed probabilities, respectively. The calibration curve demonstrates the degree of agreement between predicted and observed probabilities. (b) DCA for the nomogram in the internal validation set using the bootstrap method (resampling = 1000). The x-axis shows threshold probability, namely the minimum probability of warranting further intervention. The y-axis stands for net benefits calculated across different threshold probabilities. Horizontal solid black and gray lines represent the assumption that no and all patients had POD, respectively. The solid red line denotes the nomogram. The decision curve demonstrates that the application of this nomogram added a net benefit when threshold probability ranged from 5% to 95% compared with when either the treat-all or -none strategy was employed.
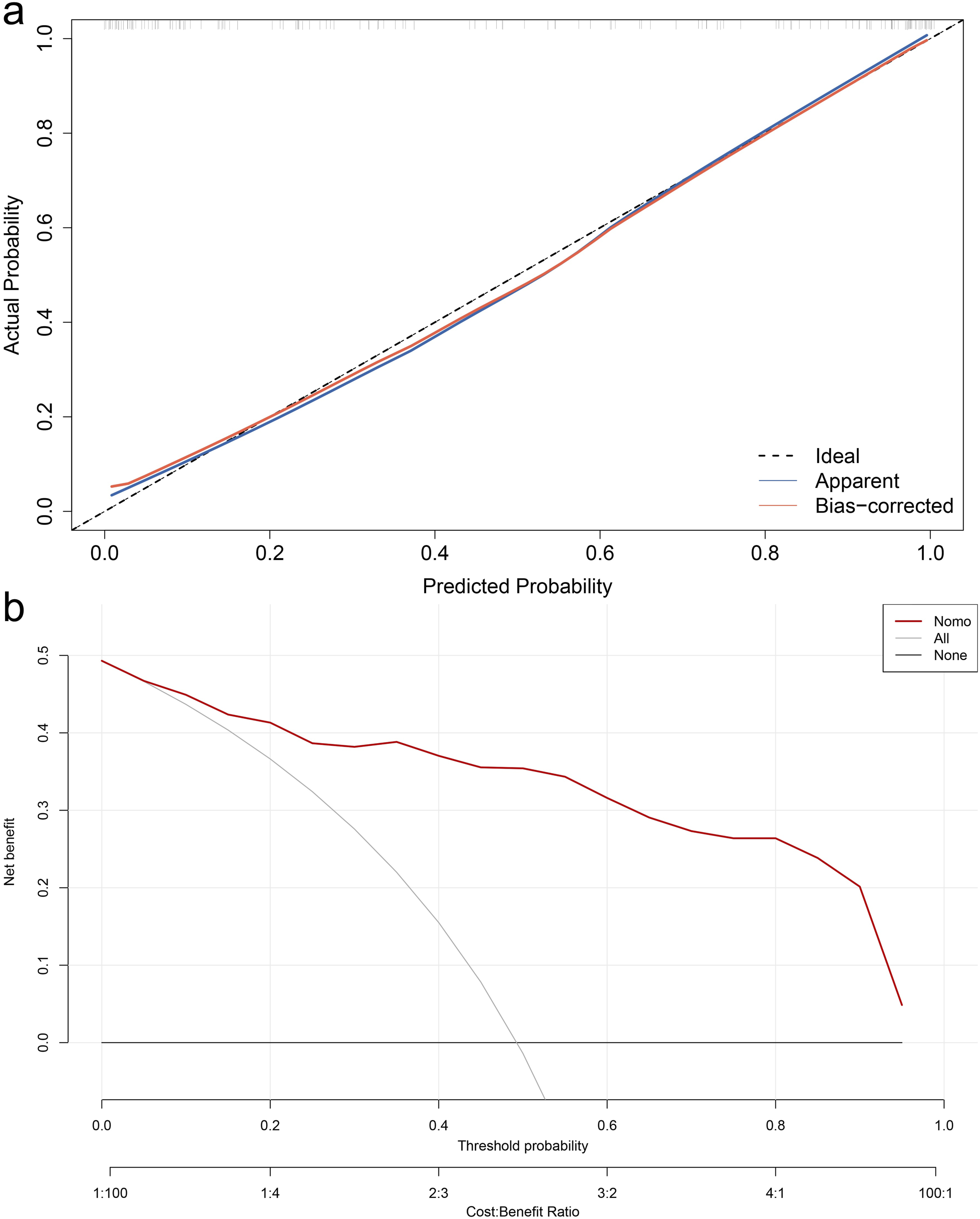
Decision curve analysis (DCA) was conducted using the bootstrap method (resampling = 1000), with the aim of assessing the clinical usefulness of this nomogram. It can be seen from the decision curve that using this nomogram for predicting POD would be more precise when the threshold probability was between 5% and 95% (Figure 5(b)). Within this scope, more net benefits were yielded when this nomogram was used to decide compared with when either the treat-all or -none scheme was used.
Cutoff of DELi Scores
Based on the cutoff of 39.5 (the largest Youden index of DELi scores for predicting POD), the DELi score was converted to binary data. A new model was constructed with this binary DELi score that replaced the original continuous DELi score for sensitivity analysis. This new model also indicated excellent discrimination (AUC = .914 (95% CI: .869, .960) in the training set and .912 (95% CI: .865, .958) in the internal validation set using the bootstrap method (resampling = 1000), see Supplemental Figure 3). No significant difference was observed in discrimination between original and new models (NRI = −8.2% (95% CI: −17.5%, −1.0%), P = .081; IDI = −2.2% (95% CI: −5.7%, −1.2%), P = .196).
Discussion
A novel EEG-derived delirium-associated index and DELi scores were introduced. It was demonstrated that preoperative DELi scores predicted the risk of early POD in old patients who underwent hip fracture repair surgeries. In this study, DELi scores per se demonstrated comparable or even better discrimination in the prediction of POD (AUC = .791) than previous models.7,8,19–21 A concise model with only three predictors incorporated this DELi score and was developed from a prospective longitudinal cohort and demonstrated excellent discrimination (AUC >.9) for predicting early POD in this population. This impressive discrimination indicated that the strong precipitating factor, hip surgeries, could easily precipitate this susceptible population into POD when the condition of predisposing factors was worse enough. Notably, the wide range of threshold probabilities (5% to 95%) highlighted its value as a useful tool for the governance of clinical decision-making.
To our best knowledge, it’s the first time to use this novel index, DELi score, for predicting early POD. Therefore, this study should be considered as a pilot study to assess the feasibility of this EEG-derived index. The inspiring results encourage further studies based on larger cohorts of the same population which may not only include more participants but also consider longer follow-up and more complex clinical scenarios.
POD can occur immediately after the recovery from anesthesia and up to five postoperative days in the hospital or until discharge.6,22 However, elderly patients with hip fractures are generally discharged on postoperative days 2 to 4 (the length of hospital stay is 4 to 6 days) as per the enhanced recovery after the surgery protocol of local health centers. To be consistent in follow-up time, POD was only tested on postoperative days 1 and 2 in all the patients. Therefore, this study reported that early POD had an incidence of 49.3%, which may optimistically estimate the incidence of POD.
It has been demonstrated that copious predisposing and precipitating risk factors are linked to POD, such as advanced age, benzodiazepines, opioids, hypotension, increased comorbid disease, preoperative cognitive impairment, massive intraoperative blood loss and poor pain control.23–25 Several POD prediction models have been developed.7,8,19–21 Unfortunately, the discrimination for predicting POD is only proved to be poor or acceptable despite the complex and numerous predictors included in these models (AUC ranging from .638 to .814). Furthermore, models commonly incorporate intraoperative and postoperative variables, such as blood transfusion, intraoperative vasopressor use, duration of surgery and anesthesia and postoperative intensive care.7,8,20 Nevertheless, an ideal POD prevention strategy should be implemented from the perioperative stages, and prediction after surgeries undoubtedly delays the intervention and attenuates effects. An accurate and concise POD prediction model using only data available before surgeries is needed to tackle the intractable issue of timely intervention.
More intricate questionnaires and prudent scrutiny may lead to a better prediction, but deviate from clinical practices. Models with a number of predictors also run a risk of overfitting, especially when predictors may be significantly associated. 26 It is plausible that a variable is conducive to developing a concise prediction model if directly measures brain status and extracts relevant attributes from various interactional preoperative risk factors.
EEG has been used in delirium studies for decades. 10 Parameters of EEG were shown to be associated with preoperative cognitive status, the leading predictive factor for POD. 11 The development of the DELi score was based on the entire frequency band-EEG wavelet algorithm.12,13 In the presence of delirium, repeatable and regular changes were extracted from brain waves as the characteristic indicators of delirium. 14 The DELi score incorporated these dynamic variations of EEG parameters attributable to delirium based on a wavelet algorithm,12,13 and was thus related to the cognitive status of delirium. 14 It was hypothesized that preoperative DELi scores could extract latent information regarding the predisposing factors of delirium and predict POD. Therefore, preoperative DELi scores might replace copious factors regarding susceptibility to POD and thus preclude a multitude of complex questionnaire surveys that were vital in previous models.7,8,19–21 For instance, age, a common predictor, was not included in this model since brain vulnerability was already assessed by DELi scores. Similarly, a previous study demonstrated that the assessment of EEG-derived baseline cognitive status was more important than chronological age for predicting POD. 11
Previous models used the binary variables of cognitive function (the presence or absence of cognitive impairment). However, it is shown that the risk of delirium is strongly linearly related to all levels of cognitive function though patients are regarded as unimpaired through formal testing. Thus, continuous scores assessing frailty status and cognitive function were used in the model of this study.
A notable strength of the model is a wide range of threshold probabilities (5% to 95%). Within this range, more net benefits were yielded when this model was used to make a decision. POD may be anticipated by an experienced clinician. However, the risk of delirium is probably more ambiguous when the risk is moderate or the clinician is less experienced. Hence, the wide range of threshold probabilities promised clinical utility and bolstered the value of this model.
It should be noted that this model was developed in elderly patients undergoing hip fracture surgeries for early POD. It is recommended that delirium prediction models be focused on specific populations. 9 As a result, the nomogram may not be extrapolated to other populations. More importantly, however, a novel index with which a concise and excellent model using a few preoperative measurements could be developed was introduced. Sensitivity analysis also demonstrated that the discrimination of the model was not altered by substituting the continuous DELi score with binary DELi classification. This indicated that DELi scores or their binary classification could be used as a robust predictor per se or contribute to a model when POD was predicted. However, studies should generalize these results to a new population and bolster extensive external validation.
Limitations
This study is single-center with a small sample. However, the sample size met the requirements of the statistical hypothesis. Furthermore, all data were used for model development, and only internal validation was conducted in this study. This might lead to overly optimistic model performance. Further studies are still needed. In addition, only data on postoperative days 1 and 2 were collected, which precluded the resolution of long-term outcomes. Moreover, it should be mentioned that the sample size was calculated for predicting POD. Thus, the difference in the duration of hospital stays between the patients with and without POD was not identified due to insufficient power.
Conclusions
A novel EEG-derived index was introduced in this study. Preoperative DELi scores predicted the early POD of elderly patients undergoing hip fracture repair surgeries. A POD prediction model with excellent discrimination that incorporated the DELi score, MoCA and FRAIL scale was developed in this population.
Supplemental Material
Supplemental Material - A Novel Preoperative Electroencephalogram-Derived Index to Predict Early Postoperative Delirium in Elderly Patients After Hip Fracture Surgeries: Development of a Prediction Model
Supplemental Material for A Novel Preoperative Electroencephalogram-Derived Index to Predict Early Postoperative Delirium in Elderly Patients After Hip Fracture Surgeries: Development of a Prediction Model by Ayixia Nawan, Geng Wang, Congcong Zhao, Wenchao Zhang, Bailin Jiang, and Yi Feng in Geriatric Orthopaedic Surgery & Rehabilitation.
Footnotes
Acknowledgments
The authors thanked all the anesthesiologists who cared for the patients.
Author Contributions
Ayixia Nawan: This author helped to generate, collect, analyze and interpret data, and conceive and write the manuscript. Geng Wang: This author helped to generate and collect data, and write the manuscript. Wenchao Zhang: This author helped to generate and collect data, and conceive and write the manuscript. Congcong Zhao: This author helped to generate and collect data. Bailin Jiang: This author helped to analyze and interpret data, conceive and write the manuscript, and finally approve the version to be published. Yi Feng: This author helped to analyze and interpret data, and conceive and design the manuscript. All authors agreed to be responsible for all aspects of this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key Research and Development Program of China under grant No. 2018YFC2001905, Bethune Charitable Foundation (BCF) under grant No. SX2022-005 and Beijing Municipal Administration of Hospitals Incubating Program under grant No. PY202101.
Ethical Statement
Clinical Trial No. and Registry Uniform Resource Locator
The methodology of data collection was registered before the enrollment of patients at the China Clinical Trials Registry Platform (ChiCTR2200060389).
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, B Jiang, upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.