
Abstract
The Honda Walking Assist® (HWA) is a light and easy wearable robot device for gait training, which assists patients’ hip flexion and extension movements to guide hip joint movements during gait. However, the safety and feasibility of gait training with HWA after total knee arthroplasty (TKA) remains unclear. Thus, we aimed to evaluate the safety and feasibility of this gait training intervention using HWA for a patient who underwent TKA. The patient was a 76-year-old female who underwent a left TKA. Gait training using HWA was conducted for 18 sessions in total, from 1 to 5 weeks after TKA. To verify the recovery process after TKA surgery, knee function parameters and walking ability were measured at pre-TKA and 1, 2, 4, and 8 weeks after TKA. The gait patterns at self-selected walking speed (SWS) without HWA at pre- and 5 weeks after TKA were measured by using 3-dimensional (3D) gait analysis. The patient completed a total of 18 gait training interventions with HWA without any adverse complications such as knee pain and skin injury. The postoperative knee extension range of motion (ROM), knee extension torque, SWS, and maximum walking speed were remarkably improved. Regarding gait kinematic parameters, though this patient had a characteristic gait pattern with decreased knee ROM (called stiff knee gait) preoperatively, the knee flexion angle at 5 weeks after TKA showed knee flexion movement at loading response phase (LR; called double knee action), increased knee ROM during gait, and increased knee flexion angle at swing phase. In this case, the gait training using HWA was safe and feasible, and could be effective for the early improvement of gait ability, hip function, and gait pattern after TKA.
Background
Total knee arthroplasty (TKA) is a widely accepted surgical treatment for severe osteoarthritis (OA). 1,2 Although TKA can lead to decreased pain, increased knee range of motion (ROM), and eventually, improved physical function and quality of life (QOL), 3 physical function (e.g., quadriceps and hamstring strength, and knee ROM) decreases immediately after TKA. 4,5 A stiff knee gait (SKG), in which there is reduced knee flexion during walking, 6,7 increases energy cost and decreases walking speed. 8 It has previously been revealed that there is a temporary postoperative decrease in walking ability, including walking speed, followed by a recovery time of several months to 1 year. 9 -11 Individuals with a notable improvement of knee gait biomechanical outcomes and walking speed have reported an improved knee-related QOL 12 ; therefore, rapid postoperative improvement of TKA patients’ walking ability is desirable.
Robot-assisted training (RAT) has been in development since the early 2000s. Several reports have demonstrated improved walking ability through the application of RAT in patients with medical conditions affecting the central nervous system, such as stroke, 13 spinal cord injury, 14 and cerebral palsy. 15 However, there are few reports demonstrating the effect of RAT in postoperative rehabilitation after TKA. 16,17 The Honda Walking Assist® (HWA; Honda Motor Co., Ltd., Tokyo, Japan) is a wearable robotic device that assists with gait training. It has a simple mechanism and is lightweight and easy to wear (Figure 1A). Actuators placed at the hip joint assist with hip flexion and extension to guide left-right symmetry and hip joint movement during walking. 18 Angular and torque sensors placed at the hip joint monitor hip joint angle, and the “assist torque” assists hip joints based on an algorithm for regulating and correcting gait. Using the HWA for gait training, we have previously reported improved lower limb kinematic parameters during walking, as well as early improvement of walking ability after surgical operation in a patient who underwent total hip arthroplasty (THA). 19 As SKG is affected by hip and knee flexion velocity at the early swing phase 20,21 (Figure 1B), we hypothesized that effective walking exercises with improved knee biomechanics may be possible with hip assistance using HWA gait training.
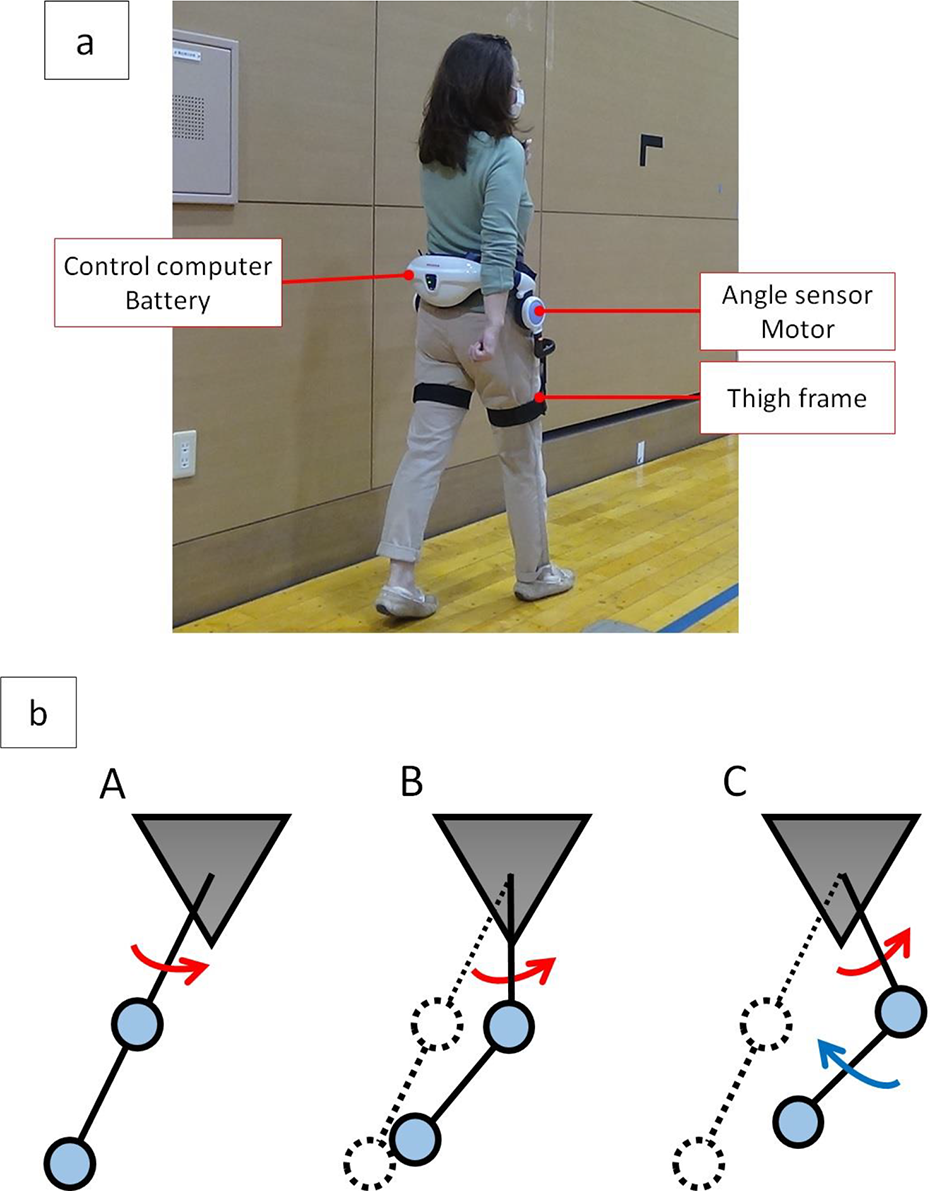
A, The Honda Walking Assist® device. b: The mechanism of knee flexion during the swing phase due to hip assistance using the Honda Walking Assist® device (HWA). HWA assistance has the effect of lifting the thigh (red arrow) during the swing phase (B and C), thereby promoting knee flexion (blue arrow).
In this study, we aimed to examine the safety of a robotic training intervention and to evaluate the effect of HWA training on knee function, walking ability, and gait kinematics during walking on a patient who underwent TKA.
Case Presentation
The patient was a 76-year-old female who underwent left TKA. She started experiencing pain in both knees approximately 20 years before TKA and managed its progression with pain medication. However, her knee pain gradually intensified and interfered with activities of daily living (ADL). For this reason, she underwent right TKA 4 months prior to left TKA. After right TKA, she could walk outdoors without using a cane, but she had difficulty walking for long distances (approximately 500 m) and climbing stairs because of pain in her left knee. Therefore, she was hospitalized to undergo left TKA.
The surgical procedure was similar to that described in our previous report. 17 Under general anesthesia, we made a midline skin incision and reached the joint using a medial parapatellar approach. The patella was not replaced, and the posterior cruciate ligament was retained. We used the Persona® (Zimmer Biomet, Warsaw, IN, USA) implant for the femoral component and the NexGen® Trabecular Metal™ Monoblock Tibia (Zimmer Biomet) implant for the tibial component.
The ethics committee of Ibaraki Prefectural University of Health Sciences approved the study (no. e204). We explained the purpose of the study to the patient using verbal and written forms, and her written consent was obtained.
Intervention
The patient underwent gait training using the HWA from 1 to 5 weeks after TKA. There were four to five 20-min sessions (excluding resting time) per week, in the hospital, for 18 sessions in total. The patient also undertook conventional rehabilitation during the intervention period, such as ROM exercise, stretching, muscle strengthening, balance training, ADL training (toileting, bathing, bedside tasks, etc.), gait training, and stair climbing training. Each HWA training session was integrated with walking exercises during physical therapy sessions. The patient was closely monitored during the HWA sessions to verify the safety of the intervention, and any adverse events, such as aggravation of knee pain or skin problems (redness or abrasion due to contact with the equipment), were noted.
Measurements
Table 1 summarizes the items and timing of measurements related to knee function, walking ability, and gait analysis.
Measurement Items and Timing.

Measurements related to knee function included: ROM in terms of knee flexion and extension during passive and active movement of the operated knee; knee extension and flexion torque (representing quadriceps and hamstring strength); and Western Ontario and McMaster Universities Osteoarthritis Index subscales of pain (WOMAC-p) and physical function (WOMAC-f) scores, modified for the Japanese context. 22 Isometric knee torque was measured using the Biodex System 4 dynamometer (Biodex Medical Systems, Inc., NY, USA), with the knee fixed in 60° of flexion. Each torque was measured 3 times for 5 s at a time, and the peak torque value was divided by body weight for further analysis.
Measurements related to walking ability included self-selected walking speed (SWS), maximum walking speed (MWS), mean step length at SWS and at MWS, and cadence at SWS and at MWS. SWS and MWS tests were carried out without the HWA, on a walking path with 3 m of extra path before and after the 10-m measurement section. To calculate step length and cadence, steps were counted during these tests.
Most of the measurements related to walking ability and knee function were measured before TKA and at 2, 4, and 8 weeks after TKA. Knee ROM was measured before TKA and at 1, 2, 4, and 8 weeks after TKA (Table 1).
Three-Dimensional (3D) Gait Analysis
The gait pattern at SWS without the HWA was measured via 3D gait analysis (Vicon Nexus ver. 1.8.5, Vicon Motion Systems Ltd., Oxford, UK). We employed a widely used marker set (Plug-in Gait lower body model, Vicon Motion Systems Ltd.) to calculate the joint angle after the definition of segments. Kinematic data were collected at a sampling rate of 200 Hz. We measured 5 gait cycles and calculated the mean to create a graph depicting the sagittal angle of the hip, knee, and ankle joint. To standardize the time of 1 gait cycle as 100%, all data were interpolated using the third spline. Gait kinematics were measured preoperatively and at 5 weeks after TKA.
Results
All sessions were completed without adverse events.
Knee Function Parameters and Walking Ability
Table 2 summarizes the knee function and walking ability results. Active and passive knee extension ROM increased steadily, and a full passive knee extension angle (0°) was achieved at week 8. Knee flexion ROM at week 8 increased to almost the same level as that measured pre-TKA. Knee extension torque exhibited early improvement, increasing past pre-TKA levels at weeks 4 and 8. Knee flexion torque at weeks 2, 4, and 8 were lower than that measured pre-TKA. The WOMAC-p score at weeks 4 and 8 was higher than that measured pre-TKA. The WOMAC-f score at week 8 was also higher than that measured pre-TKA. SWS and MWS at week 2 were almost at pre-TKA levels, and at weeks 4 and 8, SWS and MWS surpassed pre-TKA levels.
Results of the Knee Function and Walking Ability Tests.

Gait Kinematic Parameters
Gait kinematics are summarized in Figure 2. The patient’s preoperative gait was characterized by a decreased knee ROM throughout the gait cycle; this is known as SKG. In contrast, the knee flexion angle at week 5 changed during the loading response (LR) phase; this is known as double knee action. There was an increased knee ROM range throughout the gait cycle, and an increased knee flexion angle during the swing phase. Hip extension and ankle plantar flexion angle also increased at week 5, compared to that measured pre-TKA.

Hip, knee, and ankle joint angle from the sagittal plane during 1 gait cycle at self-selected walking speed. The solid line represents preoperative ROM and the dashed line represents ROM at week 5. One walk cycle is displayed as 100%, and the left initial contact is displayed as 0%.
Discussion
In this study, we investigated the safety, feasibility, and effectiveness of the HWA for rehabilitation of a patient who underwent TKA. The patient completed 18 gait-training sessions with the HWA without any adverse events such as knee pain or skin redness or abrasion. Therefore, we consider the HWA as a safe and feasible option for implementation after TKA. Postoperative knee extension ROM, knee extension torque, SWS, and MWS exhibited remarkable improvement, indicating that improvement in knee function and walking ability had been successfully obtained.
To contextualize the effect of the HWA treatment, we compared the recovery of knee function and walking ability of the patient in the present case with that of patients receiving the same surgical procedure and postoperative rehabilitation protocol, but without the HWA, in our previous report. 17 Her knee extension torque at weeks 4 and 8 and her WOMAC-f score at week 8 were higher than those of the conventional group, suggesting a satisfactory improvement in the knee joint function and ADL. Based on these results, we considered her knee function improvement to be equal or higher degree than that of patients receiving conventional physical therapy. In terms of walking ability, her SWS and MWS at weeks 2, 4, and 8 improved more than those of the conventional group. In fact, her SWS and MWS nearly plateaued at week 4. Satisfactory passive and active knee extension ROM were obtained after TKA. Because the patient in the present study had a severe knee contracture, her knee flexion ROM was slightly lower than that of the conventional treatment group. As this patient had severe preoperative knee pain, her WOMAC-p score at week 8 was lower than that of the conventional group, although it was higher than her score measured pre-TKA.
The patient in the current study exhibited an almost equal level of recovery of walking ability with that of patients undertaking a postoperative rehabilitation program using the hybrid assistive limb (HAL), an exoskeleton-type rehabilitation robot. 17 These results suggest that gait training with the HWA may contribute to the early recovery of walking ability of patients who undergo TKA, similar to that observed in the HAL-based program. Given that patients who undergo TKA do not have severe paralysis, strong assistance and large-scale equipment are not necessary. The HWA is lighter than other exoskeleton devices and easy to wear, reducing the patient burden. Therefore, gait training with the HWA may be an effective rehabilitation method for TKA patients.
Regarding gait kinematics during SWS, although our patient exhibited SKG at preoperative measurement, her gait improved to such an extent that she exhibited double knee action and larger knee ROM range at week 5. Additionally, her hip extension and ankle plantar flexion angle during the terminal stance phase also improved from pre-TKA to week 5. It has been reported that a post-TKA gait pattern is characterized by a slow walking speed, reduced knee flexion during the LR and swing phases (thus exhibiting SKG), and co-activation of the rectus femoris-muscle and hamstrings. 23,24 HWA assistance has the effect of lifting the thigh during the swing phase and assisting with hip extension during the stance phase, thereby promoting knee flexion. These results suggest that the HWA assists the patient to follow the correct walking pattern by assisting with hip flexion/extension, leading to improved gait kinetics.
This study had some limitations. We investigated only 1 patient receiving HWA intervention, and the follow-up period was only 8 weeks after TKA since the focus was on early postoperative improvement. In future, to verify these findings, comparative studies with larger sample sizes are required.
Conclusion
In this study, we investigated the safety, feasibility, and effectiveness of gait training with the HWA for a TKA patient. We assessed walking ability, knee function, and the gait kinematics parameter., and discovered that gait training with the HWA may have contributed to the early improvement in gait after TKA.
Footnotes
Acknowledgments
We would like to thank the Physical Therapy Department at Ibaraki Prefectural University of Health Sciences Hospital, represented by Kazuhide Tomita, the manager of Department of Rehabilitation, Tomoyuki Matsuda, the manager of the Department of Physical Therapy, and Keiko Miyamoto, robotic technical assistant. We would like to thank Editage (![]() ) for the English language editing.
) for the English language editing.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Honda Motor Corporation lent us the HWA free of charge for this research.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partly supported by a Grant-in-Aid for Project Research of the Ibaraki Prefectural University of Health Sciences (1961 -1, 1962 -1) and Japan Society for the Promotion of Science KAKENHI (20H01147).