
Abstract
Purpose:
The purpose of this study was 2-fold: 1) to investigate the age-related frequency, demographics and distribution of the middle-aged and geriatric orthopedic trauma population and 2) to describe the age-related frequency and distribution of hospital quality measure outcomes and inpatient cost.
Methods:
All patients > 55 years of age who required orthopedic, trauma, or neurosurgery consults at 3 hospitals within an academic medical center from 2014 to 2017 were prospectively followed. On initial evaluation, each patient’s demographics, injury severity, and functional status were collected. Patients were grouped into low and high-energy mechanism cohorts and divided into 5 groups based on age. Hospital quality measures including length of stay, complications, discharge location, and cost of care was compared between age groups. Data were analyzed using ANOVA and Chi-square tests.
Results:
A total of 3965 patients were included in this study of which 3268 (82%) sustained low-energy trauma and 697 (18%) sustained high-energy trauma. With increasing age, more patients had more comorbidities, were less likely to be community ambulators, and more likely to use assistive devices (p < 0.05). Patients in older age groups had longer lengths of stay, more complications, were more likely to need ICU level care, and were less likely to be discharged home (p < 0.05). Rates of mortality were also greater in patients of more advanced age in both low and high-energy cohorts, and the calculated risk triage tool (STTGMA) score increased with each age bracket (p < 0.05). Total cost of care differed between age groups in the low-energy cohort (p = 0.003).
Conclusion:
This epidemiological study provides a clear picture of the frequency and distribution of demographic, physiologic characteristics, outcomes, and cost of care in a middle-aged and geriatric orthopedic trauma population as evaluated by the STTGMA risk tool. Risk profiling of geriatric trauma patients allows for the establishment of baseline norms.
Introduction
The incidence of traumatic injuries in patients age 55 and older continues to increase in the United States according to the American College of Surgeons Trauma Quality Improvement Program (ACS TQIP). 1 In 2016, patients age 55 and older comprised 42.56% of all traumas and 57.63% of trauma-related deaths. 2 As the population ages, these numbers are predicted to increase. These middle-aged and geriatric trauma patients tend to have worse functional recovery and often require early intervention in order to make strides toward improvement in their functional status. 3 -5 Geriatric patients who lose even one ADL following a traumatic incident are more likely to sustain additional traumas, require placement in a rehabilitation facility, and have higher rates of mortality. 6,7 The elements that contribute to the decline in these patients are multifactorial and include Glasgow Coma Scale (GCS), sociodemographic characteristics, comorbidities, frailty, and lower pre-trauma level of functioning. 8 -12
It is important to better understand the characteristics of middle-aged and geriatric patients who present with traumatic injuries in order to anticipate their needs and resource utilization. There are few studies that provide a comprehensive characterization of injury patterns, sociodemographic data, patient outcomes, and cost data for middle-aged and geriatric trauma patients. This study aims to provide quantitative data to fill this void.
Patients and Methods
This study was an institutional review board-approved prospective analysis of all patients aged 55 years or older who were evaluated by the orthopedic, trauma, and/or neurosurgery teams within the emergency department at 2 American College of Surgeons (ACS) certified academic level 1 trauma centers and 1 academic tertiary referral center within a single academic medical center between October 1, 2014 to September 30, 2017. As defined by ACS guidelines, 13 trauma activation tiers 1, 2, and 3 were included in this study. A total of 3965 consecutive patients met the inclusion criteria for this study.
Study variables were collected prospectively at the time of initial patient evaluation. Data collection included variables that comprise the Score for Trauma Triage in the Geriatric and Middle-Aged (STTGMA), an inpatient mortality risk assessment tool developed by this same group which can be used in the emergency department to better identify those middle-aged and geriatric patients who would benefit from early intervention. STTGMA has been validated in the National Trauma Data Bank and in multiple Level 1 Trauma Centers as a reliable risk and cost stratification tool. 14 -16 These variables included patient age, Glasgow Coma Score (GCS), mechanism of injury, Abbreviated Injury Severity (AIS) sub-scores for the head and neck (AIS-HN), chest (AIS-CHS), and pelvis and extremity (AIS-EXT), as well as Charlson comorbidity index (CCI), ambulatory status, serum albumin levels, use of assistive device, and pre-injury anticoagulation status. Patient demographics, injury severity, and functional status were then utilized to calculate a validated STTGMA score that is reported as a percentage risk of inpatient mortality.
Information regarding length of stay, complications during hospitalization, need for intensive care unit/step-down unit level care, and locations of disposition were collected via chart review. Minor complications included surgical site infection, decubitus ulcer, urinary tract infections, and acute anemia. Major complications included acute renal failure, septic shock, pneumonia, acute respiratory failure, acute myocardial infarction, deep vein thrombus, pulmonary embolism, cardiac arrest, stroke, and inpatient mortality. Patients were followed for 90 days to observe for readmissions and 1 year to observe for mortality.
Direct variable cost data for inpatient hospitalization was obtained from the hospital cost accounting system at one American College of Surgeons certified academic Level 1 Trauma Center. ICD-10-CM codes for injury characteristics were obtained from the electronic medical record of all participating hospitals. Patients were first divided into low-energy and high-energy mechanisms of injury. Within these 2 large groups patients were subdivided into 5 cohorts based on age: 55-60 (Group 1), 61-70 (Group 2), 71-80 (Group 3), 81-90 (Group 4),
Statistical Analysis
All comparisons were made among cohorts within the larger mechanism-of-injury cohorts. No comparisons were made between low and high-energy subgroups except for injury distribution. Statistical methods were used to assess for differences between age groups. Statistical significance was defined as p < 0.05. Primary study measures included major and minor complications, hospital quality measures, mortality, and cost which were obtained from the medical record by designated research staff. Data were evaluated using ANOVA and Chi-Square tests. All calculations were performed using SPSS version 23 (SPSS Inc., Chicago, Illinois).
Results
A total of 3966 patients met the inclusion criteria and were included in this study. There were 3268 (82%) low-energy mechanism of injury patients and 697 (18%) high-energy mechanism of injury patients. The average age of the low-energy cohort was 75.53 (SD 11.83) and the average age of the high-energy cohort was 68.25 (SD 10.07). The majority of both cohorts was female with the percentage of male patients decreasing with increasing age. In addition, mean CCI, anticoagulation status, ambulator status, and use of assistive device varied between age groups in both the low and high-energy cohorts. With increasing age, patients had more comorbidities, were more likely to be on anticoagulation at baseline, had lower ambulator status, and were more likely to use assistive devices (Tables 1 and 2). STTGMA scores, which reflect an increased risk of inpatient mortality, also increased with increasing age. Complete descriptive data and calculated STTGMA scores for each age group are summarized in Tables 1 and 2.
STTGMA Variables in Low Energy Injury Mechanism Injuries Grouped by Age.

Note: * = statistically significant value; GCS: Glasgow Coma Scale; AIS H/N: Abbreviated Injury Severity Head/Neck; AIS Chest: Abbreviated Injury Severity Chest; AIS E/P: Abbreviated Injury Severity Extremity/Pelvis; CCI: Charlson Comorbidity Index; STTGMA: Score for Trauma Triage in the Geriatric and Middle Aged
STTGMA Variables in High Energy Injury Mechanism Injuries Grouped by Age.

Note: * = statistically significant value; GCS: Glasgow Coma Scale; AIS H/N: Abbreviated Injury Severity Head/Neck; AIS Chest: Abbreviated Injury Severity Chest; AIS E/P: Abbreviated Injury Severity Extremity/Pelvis; CCI: Charlson Comorbidity Index; STTGMA: Score for Trauma Triage in the Geriatric and Middle Aged
Length of stay increased with advanced age with the average length of stay for patients aged 55-60 and 91+ in the low energy cohort being 2.77 days and 5.25 days, respectively (p < 0.0005). In contrast, there was no statistically significant difference between the length of stay of the different age groups in the high energy cohort. However, while not statistically significant, patients in Group 1 had lower lengths of stays than those in Group 3 and 4. With respect to complications, both minor and major complications varied between age groups in both the low- and high-energy cohorts with the rate of complications increasing with increasing age. The most common complications included urinary tract infections and acute anemia for the low energy cohort with the addition of acute respiratory failure for the high energy cohort (Tables 3 and 4). Furthermore, the need for ICU level care increased with age in both the low energy and high energy cohorts. In observing discharge patterns, the rate of favorable discharge decreased with increasing age in both the high and low energy cohorts with only 12% of patients over 90 years of age who sustained a low energy injury being discharged home. In addition to less patients being discharged home, the rate of readmission at both 30 and 90 days increased for older patients in the high energy cohort. By contrast, the rate of readmission at both 30 and 90 days did not differ for patients in the low energy cohort (Tables 5 and 6). Lastly, mortality rates within 1 year for both low and high energy cohorts increased with increasing age (p < 0.0005) (Tables 7 and 8).
Complications in Low Energy Mechanisms Cohort Grouped by Age.
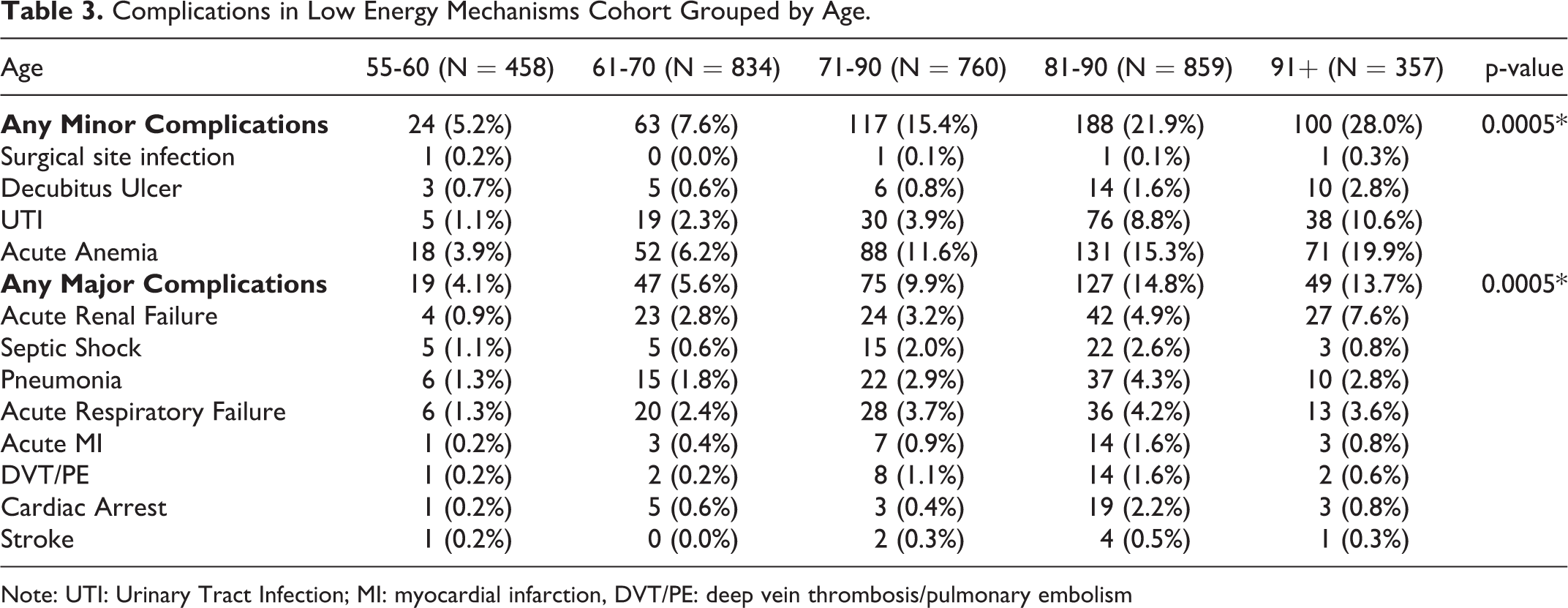
Note: UTI: Urinary Tract Infection; MI: myocardial infarction, DVT/PE: deep vein thrombosis/pulmonary embolism
Complications in High Energy Mechanism Injuries Grouped by Age.
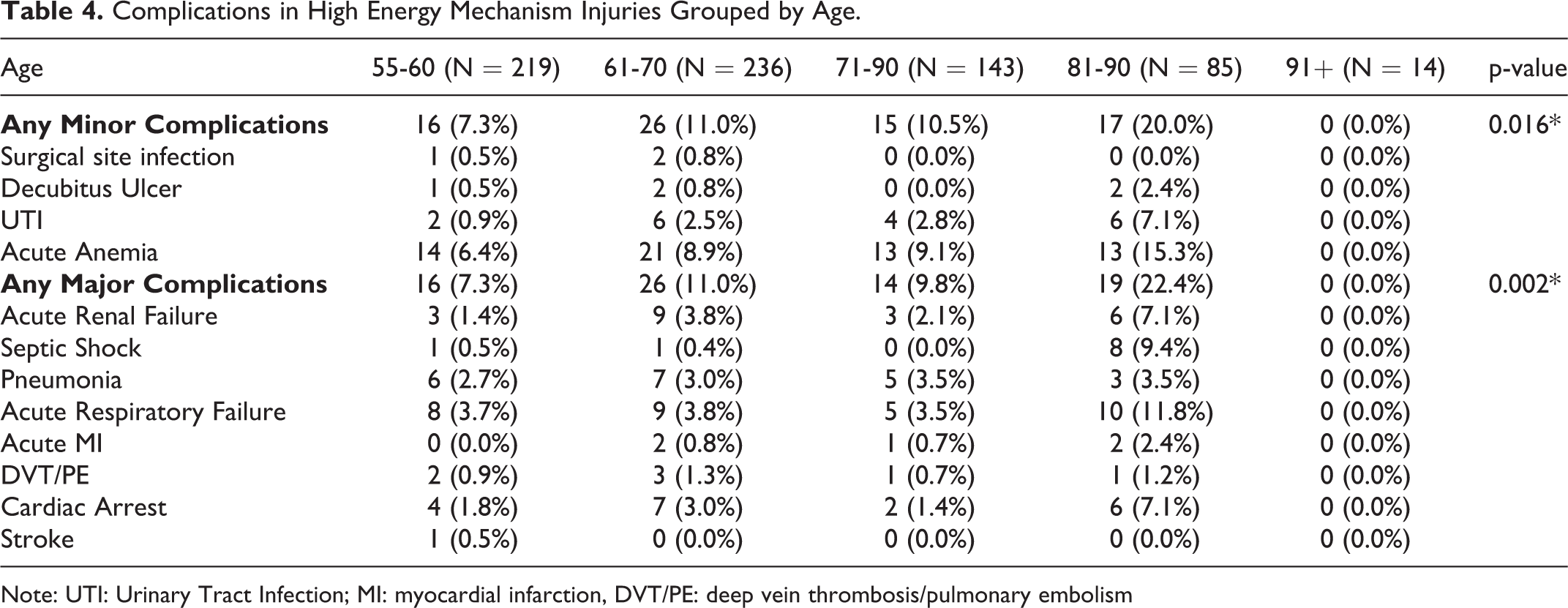
Note: UTI: Urinary Tract Infection; MI: myocardial infarction, DVT/PE: deep vein thrombosis/pulmonary embolism
Hospital Quality Measures in Low Energy Injuries Grouped by Age.

@Denotes the number of patients in each cohort from the single ACS certified Level 1 Trauma Center from which inpatient hospital direct variable cost data was obtained.
Hospital Quality Measures in High Energy Injuries Grouped by Age.

@Denotes the number of patients in each cohort from the single ACS certified Level 1 Trauma Center from which inpatient hospital direct variable cost data was obtained.
Mortality of Middle-Aged and Geriatric Trauma Patients Suffering Low Energy Mechanism Injuries Grouped by Age.

Mortality in High Energy Mechanism Injuries Grouped by Age.

The total cost of care was significantly higher in the older age groups in the low energy cohort. The mean cost of care in patients over 91 was nearly $4000 greater than that of the 55-60 age group. Additionally, specific subgroups of cost including expenses for Room/Board, Pharmacy, Pathology Laboratory, Radiology, Cardiology and Allied Health increased with increased age (p < 0.05) (Table 5). In the high energy cohort, the total cost of care was not significantly different between age groups; however, there were specific subgroups of cost that did vary between age groups with older patients having greater cardiology and radiology expenses (p < 0.0005 and p = 0.026, respectively) (Table 6).
The injury distribution of the cohorts along with corresponding ICD-10-CM codes are shown in Table 9. The most common injury patterns for low energy patients was injuries to hip and thigh (ICD-10-CM S70-79) followed by injuries to knee and lower leg (S80-89). The most common injury patterns for patients in the high energy cohort were injuries to the head/neck (S00-S19) followed by injuries to the knee and lower leg (S80-89).
Distribution of Injuries by ICD-10-CM Code for Patients with High- and Low- Energy Injury Mechanisms.

Discussion
This study highlights the distribution of demographic, physiologic characteristics, outcomes, and cost of care of middle-aged and geriatric orthopedic trauma patients by age. As demonstrated in this study, patient length of stay, hospital complications, need for ICU care, mortality, and cost of care increases with increasing age.
Our data demonstrates increased risk of mortality with increasing age in both the low and high-energy cohorts. This is consistent with previous findings by Konda et al who reported that the factors predictive of inpatient mortality among elderly patients included age, GCS score, and AIS Head/Neck and AIS Chest. 14,15 Other studies have reported a doubling in mortality rate of patients above the age of 74 compared to those between 65 and 74 years of age. 13,17 When looking at all adult trauma patients, the risk of mortality significantly increases at 57 years of age and keeps increasing with age. 17
This finding that mortality increases with age in middle-aged and geriatric trauma patients has caused discussion within the field surrounding the correct quantitative definitions for middle-aged and geriatric populations. As nearly a quarter of patients seen as trauma activations across the United States are 65 years of age or older, it is important to understand the impact of age on mortality to make guidelines surrounding triage. The Advanced Trauma Life Support (ATLS) recommends transport of any traumatically injured patient over the age of 55 years old to a trauma center. Caterino et al. recommended an age cutoff of 70 years after determining that patients greater than 70 years old had a significantly greater mortality rate when adjusting for Injury Severity Indices (ISIs). 13 However, Konda et al. determined that historic ISIs have only fair to moderate predictive capacity for mortality for geriatric patients with low energy traumatic injuries and have moderate to excellent predictive capabilities for high energy traumas in geriatric patients. 14 The authors concluded that high and low energy cohorts should subsequently be evaluated separately to avoid overestimating the effects of medical comorbidities and underestimating the effect of age. Therefore, it is important to analyze outcomes of middle aged and geriatric trauma patients by injury mechanism as done in this study.
The increase in mortality rate with increasing age is seen in the general trauma population as well. Analysis of demographic and mortality data from the National Trauma Data Bank (NTDB) demonstrates that this trend of increasing mortality with age has been stable since 2005 with the percentage of trauma patients over the age of 55 dramatically increasing (Table 10). 18 From 2005, the percentage of trauma patients over the age of 84 has doubled from 5.26% of all cases to 9.97% of all cases. Similarly, the percentage of trauma patients between the 65-74 has increased from 5.62% to 10.23%. The recorded number of trauma patients annually has also been increasing steadily since 2008 (506,452 in 2008 to 861,888 in 2016). In addition, the percentage of high injury severity injuries (ISS above 15) has remained stable within each age group for the past decade.
Trauma Incidence by Age Group and Associated Case Mortality Rate From 2005-2016 (Obtained From NTDB Data).

In addition to increased mortality, our analysis demonstrates that with increasing age, patients in the low energy cohort had hospitalizations with longer lengths of stay. While there was not a statistically significant difference in length of stay between all age groups in the high energy cohort, patients above the age of 80 had overall longer admissions than those younger than 80. These longer admissions were associated with increased number of complications, both major and minor, and the need for ICU level care. Upon discharge, older patients were more likely to be discharged to a post-acute facility and have higher readmission rates.
Prediction of hospital quality measures and cost of care has become increasingly important in the past decade given the emphasis on value-based care and new reimbursement models. It is imperative for hospital systems to advocate for continued/increased funding for these middle-aged and geriatric trauma patients. This study highlights the expected hospitalization cost of care and hospital quality measures for each age group for both low and high energy mechanisms of injury. With this information, hospital systems can more accurately predict resource utilization for their patients to provide better care for their patients. As the population ages and incidence of middle aged and geriatric trauma increases, understanding this population will become more important.
Our finding of increased resource utilization with increasing age is consistent with other studies in the literature. Age as a risk factor for increased hospital length of stay and complications in geriatric trauma patients has been demonstrated in several studies. 19 This correlation even remains after controlling for patient comorbidities and ISS score. However, the mean/expected length of stay, complications, cost of care for different age groups are not cited in these studies. 19,20 Furthermore, previous analyses including those from our institution have demonstrated that several injury severity scores including TRISS, ISS, and STTGMA, can predict mortality and length of stay. Of these scores, only STTGMA includes age as a continuous variable. This study demonstrates that age alone also correlates with hospital quality measures, mortality, and admission cost of care. This allows hospitals upon initial presentation with limited information, simply age and mechanism of injury, to determine roughly the resources and outcomes of middle-aged and geriatric trauma patients.
While this study incorporated patients from several institutions over a 3-year period, they were all located in one urban metropolitan area which may not be reflective of the patient population at other institutions. Second, given the low incidence of patients over the age of 80 who sustain high energy injury patterns, the number of patients in the older high energy cohorts is small relative to the other cohorts in this study. This low number may contribute to the lack of statistical significance seen for some measures in the high energy cohort including length of stay and cost of care. However, given the lack of epidemiological data of this patient population published in the literature, we feel that this analysis is important to report. Third, hospital costs vary between institutions and the direct cost data reported in this manuscript may not be representative of other institutions around the country. However, direct cost data is more accurate than often reported charge data.
In conclusion, this epidemiological study provides novel data regarding the frequency and distribution of demographic and injury characteristics, hospital quality measure outcomes, and hospital resource utilization costs associated with middle-aged and geriatric orthopedic trauma populations. Risk profiling of geriatric trauma patients via a prospective database and using the validated STTGMA tool allows for the establishment of baseline norms for injured patients to help guide management for acute, short term, and long-term care.
Footnotes
Authors’ Note
IRB approval was obtained for the data collected in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.