
Abstract
Background:
Patient reported outcome measures (PROMs) are becoming well recognized as an important component of health care outcomes and determinants of value in patient-centered care. Yet, there is emerging recognition that guidance is lacking in the utilization of PROMs in hip fracture patients. The aim of this study was to collect input from hip fracture patients and their health care advocates as proxies to identify outcomes that are important and to gain insight into which ones are of greatest importance.
Methods:
A cross-section of patients aged 65 and older treated for hip fractures at a single level 1 trauma center within the previous 3 to 9 months was identified. Semistructured telephone interviews of patients and/or health care proxies were performed in 2 phases: (1) concept identification and conceptual framework development and (2) item generation and assessment of relative importance of health care outcomes. Each phase was completed by separate patient cohorts.
Results:
Sixty-four interviews were completed. Eighteen interviews with 13 patients and 5 proxies were completed for framework development. Forty-six interviews with 33 patients and 13 proxies were completed for the assessment of relative importance. Care team and communication were reported as important in hip fracture patients. Physical outcomes were ranked as most important by only 9% of respondents. “Having confidence that I/my loved one received the best care possible” was perceived as very important by 98% of respondents and “Having access to the surgeon” was perceived as very important by 76% of the respondents.
Conclusions:
In our study, communication between patients and care providers as well as collaboration among patients’ care providers ranked as the most important postoperative preferences in our cohort. Notably, physical outcomes were ranked as most important by only 9% of respondents.
Keywords
Introduction
The number of elderly adults in the United States is steeply rising. In 2014, individuals aged 65 and older represented 14.5% of the US population. By 2040, this number is expected to increase to 21.7% of the population. 1 This surge in the number of older individuals will impact many health care specialties, but its effect on the practice of orthopedic surgery will be profound. It is estimated that 1 of every 3 elderly individuals will sustain a fall each year. Falls are responsible for 95% of hip fractures. 2,3 Currently, over 300 000 elderly people are hospitalized annually for hip fractures. 4,5 As the elderly population increases, the number of hip fractures will also rise. 1,6,7
Patient reported outcome measures (PROMs) are becoming well recognized as an important component of health care outcomes and determinants of value in patient-centered care. However, there is emerging recognition that guidance is lacking in the utilization of PROMs in hip fracture patients. 8,9 In addition, very little work has been accomplished to understand patient priorities in outcomes following hip fracture care. Most research regarding the identification of patient priorities in hip fracture care and recovery (largely accomplished outside of the United States) points to the need for consideration of the complexity of the patient’s medical and cognitive status. 8,10 -14 Further, there is great variation in the patient demographics of those experiencing and recovering from hip fracture, which further complicates the identification of a single set of priorities for all hip fracture patients and points to the need to understand how best to incorporate health care proxies. 15 -17
Given the growing incidence of hip fractures, the known variation in physiological and neurological wellness in this population, 15 and the lack of knowledge regarding patient priorities during recovery from hip fracture, we sought to gather pilot data on the priorities of patients who have sustained hip fractures. To ensure assessment of priorities of patients with potentially a greater number of medical comorbidities, including cognitive impairment, data from health care advocates or proxies were also sought. The primary goal of our work was to determine and rank outcome priorities in a small cohort of hip fracture patients.
Methods
All patients aged 65 and older and treated for hip fractures at our institution are entered into a hip fracture registry. Following institutional review board approval, this registry was utilized to identify patients who had sustained an isolated low-energy hip fracture in the previous 3 to 9 months. A cross-sectional study design consisting of semistructured interviews of patients or proxies was executed. Chart reviews were performed via the electronic medical record to ascertain whether each patient was an independent decision maker or whether the patient had a health care agent. During the standard care delivery process, health care agents were identified as proxies when the patient was unable to advocate for himself/herself secondary to dementia, Alzheimer disease, or memory loss, or when a physician-documented inability to make independent health care decisions was identified. Responses were obtained directly from the patients themselves whenever possible. However, the inclusion of proxies allowed identification of priorities for patients with cognitive deficits. Exclusions to study participation were non-English speaking patients or patients with a diagnosis of cognitive impairment with no health care proxy named in the electronic medical record.
The study was conducted at Regions Hospital, a large urban, community hospital, which also serves as the region’s level 1 trauma center. All data were collected by Health Partners Institute and documented in research electronic data capture (REDCap) system. 18 Two phases of the study were undertaken: (1) concept identification and conceptual framework development and (2) item generation and assessment of relative importance of health care outcomes. Each phase was completed by separate patient cohorts (Figure 1).

A flow diagram illustrating the process of patient invitation and enrollment, including those who were excluded or declined participation.
Phase 1: Concept Identification and Conceptual Framework Development
To identify important outcomes following hip fracture, we conducted in-depth semistructured interviews with patients and/or their proxies. (Appendix 1A) Invitation letters were sent to identified patients (or health care agents) to explain the purpose of the study and to invite them to participate. Prospective respondents were given the option to either participate or opt-out of the study. If they did not opt out, patients (or health care agents) were contacted 1 week later by a trained interviewer. Semistructured telephone interviews were conducted and the patients’ responses were recorded. Interviewers asked open-ended questions relating to the patient’s experience during their recent hip fracture treatment.
The semistructured telephone interview scripts were adapted based upon initial results to include questions about functional outcomes. These questions were fielded with an additional group of patients and health care agents (Appendix 1B).
Upon completion of semistructured interviews, responses were distilled into themes, and a set of declarative statements was produced. These were reviewed by all project team members for face validity and further categorized into themes for group analysis. The resulting thematic report was used as the basis for the conceptual framework leading to item generation.
Phase 2: Item Generation and Assessment of Relative Importance of Health Care Outcomes
In the second phase, a telephone-based interview survey was then designed to assess the relative importance of the patient-centered components of orthopedic care and outcomes. Questionnaire items were generated using the thematic report summarizing prior interview data. Best practices for question writing and survey development were used. 19 Upon completion of the draft instrument, it was reviewed for face validity by a panel of content experts including an orthopedic surgeon, a hospitalist, a clinical research director, and survey methodologists not directly involved in the questionnaire development. 20
Steps were taken to minimize the cognitive load on participants by limiting each section to no more than 5 declarative statements. To avoid ceiling effects in outcomes reported as important, respondents were asked to further rank their “very” and “somewhat” important statements. The interview script was crafted to facilitate patient understanding. Two separate scripts were created and tailored for either patients or proxies.
A priori we sought to obtain 50 consents and completed surveys. The same invitation and contact protocol used in phase 1 was employed. Preliminary invitation letters were sent to inform as well as to provide the opt-out option. Up to 10 contact attempts from interviewers were made to patients who did not opt out. During interviews, patients were asked to rate the importance of each declarative statement on a scale of 4 options: very important, somewhat important, somewhat not important, or not at all important. After a relative importance had been recorded for each declarative statement in a section, the interviewer repeated the items that had been identified as very or somewhat important, and the participant was then asked to quantitatively rank the top 2 most important health care components in the given section. At the conclusion of the interview, participants were then asked to quantitatively rank each of the 6 sections based on their overall relative importance.
All telephone encounters concluded with the EQ-5D-3L questionnaire and the visual analogue scale (VAS) for pain assessments to describe the study cohort of hip fracture patients. 21 Proxies were asked to respond/provide information relative to the patient.
Results
A total of 148 eligible patients and/or proxies were contacted and 64 interviews were completed with a 43% response rate. Eighteen interviews with 13 patients and 5 proxies were completed for framework development. Forty-six interviews with 33 patients and 13 proxies were completed for the assessment of relative importance. Figure 1 describes the project flow and subject recruitment process. Demographics for the full cohort, including 46 females and 18 males, are given in Table 1.
Demographics of Hip Fracture Patients Included in Self-reported and Proxy-Reported Results.
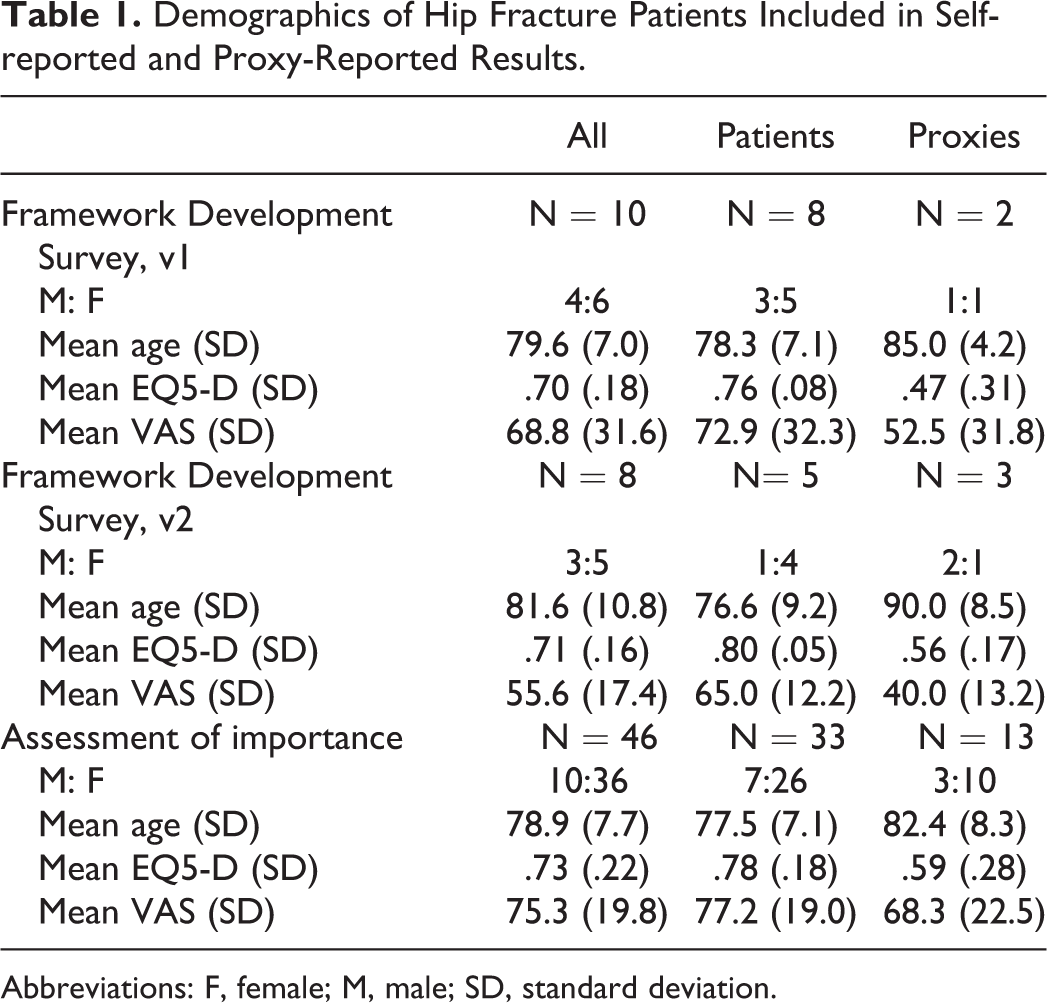
Abbreviations: F, female; M, male; SD, standard deviation.
Phase 1: Concept Identification and Conceptual Framework Development
Enrollment for this phase occurred from May 2014 through June 2015. An iterative process was utilized in the generation of the conceptual framework, and 2 versions were required before thematic saturation was thought to be achieved by the team and content experts (see Appendix 1A and B).
Upon completion of semistructured interviews, the text from each recorded call was coded and placed into a matrix (MSExcel, Microsoft Corp). Next, interview responses were studied, organized into categories, concepts were distilled, and themes were grouped. Results were finally reviewed by the full team to ensure that all categories, concepts, and themes were appropriately represented from the data set. This work resulted in identifying the following themes: People, Communication, Coordination, Physical outcomes, Feelings, and Expectations during transition from the hospital. Example quotes from the respondents include the following: “Went pretty well, it was new to me…They got me up really well the first time. Wish they would have done more treatment.” (ie. physical therapy) (Patient ID #52, Q2, 89 y.o., F) “…I am more interested in them being interested in me than in what is going on around me…” (Patient ID #34, Q7, 85 y.o., M) “The thing that scared me the most and the thing that I ended up liking the most was helping to overcome my fear. Going up and down the stairs. The persistence, help you gain the trust.” (Patient ID #51, Q7, 72 y.o., M)
Phase 2: Item Generation and Assessment of Relative Importance of Health Care Outcomes
Based upon the result from the previous phase, the final survey included the 6 categories: People, Communication, Coordination, Physical outcomes, Feelings, and Expectations during transition from the hospital. A series of declarative statements related to each category was developed and utilized in a telephone survey for this second phase (Appendix 2). Enrollment for this phase of the project occurred from June 2016 through May 2017.
Analysis of the results from this portion of the project included a direct rating of the percentage of responses for “very important” and (95% CI) regarding each declarative statement within each category. These were then ranked by highest percentage.
Within the category of People, the statement “Having confidence that I received the best possible care” was ranked #1 overall, and independently with patients and proxies with 98% overall, 97% of patients and 100% of proxies responding with “very important.”
Within the category of Communication, the statement “Getting all questions answered” was ranked #1 overall, and independently with patients (94% and 94%, respectively), while proxies rank this statement as #2 with 92% with “very important.” In the Communication category, the statement which resulted in the #1 ranking by proxies was “Having the care team explain things in language that is understandable,” with 100% stating that this was “very important.”
Within the category of Coordination, the statement “Feeling like all members of the care team are on the same page” was ranked #1 overall, and independently with patients and proxies with 84% overall, 84% of patients and 85% of proxies responding with “very important.”
Within the category of Feelings, the statement “Feeling like my wishes (wishes of the patient) are being heard” was ranked #1 overall, and independently with proxies (78% and 92%, respectively), while patients ranked this statement as #2 with 73% stating “very important.” In this category of Feelings, the statement which resulted in the #1 ranking by patients was “Feeling like the care team understands the impact of this event in my life,” with 76% stating that this was “very important.”
Within the category of Physical Outcomes, the statement “Avoiding complications after fracture treatment” was ranked #1 overall, and independently with patients (93% and 94%, respectively), while proxies ranked this statement as #2 with 92% stating “very important.” In this category of Physical Outcomes, the statement which resulted in the #1 ranking by proxies was “Having the care team set and explain realistic goals for my physical outcomes,” with 100% stating that this was “very important.”
Finally, for the category of Expectations, the statement “Being connected with resources such as equipment, home modifications, rehabilitation, or support for daily activities after leaving the hospital” was ranked #1 overall, and by patients and proxies independently (78%, 75%, and 85%, respectively.)
After a relative importance had been recorded for each declarative statement in a section, the interviewer repeated the items that had been identified as very or somewhat important, and the participant was then asked to quantitatively rank the top 2 most important health care components in the given section. All results for percentages and confidence intervals of patients and proxies responding “very important” are given in Table 2.
Results of Rating and Ranking in the Assessment of Relative Importance.

At the conclusion of the interview, participants were asked to quantitatively rank each of the 6 sections based on their overall relative importance. Figure 2 depicts the percentage of patients/proxies who ranked each category as either “most important” or “second most important” overall. Care team and communication were reported as important in hip fracture patients. Physical outcomes were ranked as most important by only 9% of respondents. The relative importance within the Care Team category: “Having confidence that I/my loved one received the best care possible” was perceived as very important by 98% of respondents and “Having access to the surgeon” was perceived as very important by 76% of the respondents.

A bar chart demonstrating the percentage of patients ranking each outcome category as either “most important” or “second most important” overall.
Discussion
There exist today many instruments to assess physical function, 22,23 hip-specific function, 24 -26 and quality of life in hip fracture patients. 27,28 While most of these require direct patient reporting, none have been designed specifically for the hip fracture patient population, nor take into consideration patient preferences for outcomes on which to report. 10 This omission is even more acutely true in the frailer, elderly patients, who have historically been broadly excluded from hip fracture trials and clinical outcomes research on the topic. 16,17
Recent systematic reviews have assessed the quality of PROMs used in hip fracture care. Haywood et al 29 reviewed and summarized the acceptability of 28 PROMs and concluded that there was only minimal evidence supporting the use of only a few measures, and most measures currently utilized have very limited relevance to this patient population. 29 In addition, PROMs do not necessarily address the patient’s own priorities. Patient involvement in PROM development, evaluation, or implementation in hip fracture outcomes has not been reported. 10,30,31 Current and future research priorities around PROMs in hip fracture patients must seek to understand which outcomes matter most to the patients themselves. In addition, due to the wide variation in health status at baseline in hip fracture patients, this work must also determine how best to appropriately incorporate proxy or health care advocate completion. 16,17
Our study sought to conduct interviews to determine outcome priorities of hip fracture patients. This work identified the following themes: People, Communication, Coordination, Physical outcomes, Feelings, and Expectations during transition from the hospital. Sims-Gould et al described the expectations of a cohort of 48 patients who were within a year of hip fracture. 32 By employing a semistructured format and a mixed-method study design similar to our own, they determined that, in this community dwelling, cognitively sound population, managing expectations, focusing on physical activity, and maintaining optimism during recovery were the most important themes.
We also worked to understand the rank order of importance of identified priorities in a second cohort of hip fracture patients. Care team and communication were reported as important in hip fracture patients, including the relative importance within the Care Team category: “Having confidence that I/my loved one received the best care possible” was perceived as very important by 98% of respondents and “Having access to the surgeon” was perceived as very important by 76% of the respondents. Physical outcomes were ranked as most important by only 9% of respondents, including subcategories of goals for physical outcomes, avoiding complications, avoiding ongoing pain, and recovery of prefracture activities.
Prior authors have hypothesized that outcomes important to younger, more healthy and independent patients, might be different from those important to a person who perceives themselves as nearing the end of life. Griffiths et al 10 and others have not been able to identify a PROM specific to the assessment of hip fracture patient nor any robust evidence of the quality and acceptability of nonhip fracture specific PROMs used for hip fracture patients. 29,33 These authors conclude that clarity in which outcomes of health care are considered most relevant to hip fracture patients do not currently exist, and it is unlikely that a single PROM could be developed for the entire spectrum of patients experiencing hip fracture. Therefore, our work in understanding relative importance could lead to important development of appropriate PROMs for this patient population.
Limitations in our study can be identified. We have only included a small sample of hip fracture patients, though our response rates (64 of 148, 43%) are similar to Griffiths et al (31 of 62, 50%). 10 We also included patients who were 3 to 9 months posthip fracture in each phase of the study. Selection of this time point is in range with other qualitative research reports in this patient population 10,32 and allows sufficient time for adequate recovery in the immediate postoperative period, though the impact of memory recall at this time point is unknown. In addition, this pilot work did not allow the possibility to compare and analyze patient and proxy responses, and prior work in a similar population does indicate some limitations to proxy responses, specifically in patients having dementia or cognitive impairment. 34 By attempting to include all patients or their proxies, regardless of cognition status, our work is susceptible to underreporting of pain or its importance. Though this limitation is unable to be resolved within the scope of this work, our findings of importance in physical outcomes, including pain, being ranked as most important by only 9% of respondents, aligns with the results of Griffiths et al, 10 who reported that pain was “not considered a major problem.” Finally, the methods of survey development tailored to the geriatric population must be further explored and perfected, but our study is unique step in this important direction.
In our study, communication between patients and care providers as well as collaboration among patients’ care providers ranked as the most important postoperative preferences in our cohort. Additionally, physical outcomes were ranked as most important by only 9% of respondents. This preliminary work and findings can promote future research in geriatric orthopedic outcomes and serve as the foundation for the development of a validated measure of patient-preferred outcomes in elderly hip fracture patients to be used at a national scale. This work may also be used to evaluate the relative value of innovative care models that are designed to improve more than traditional functional outcomes.
Footnotes
Appendix 1
Appendix 2
Categories and Statements of Importance: Six categories of care, each containing no more than 5 declarative statements
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded a Clinical Research Committee grant through the Department of Orthopaedic Surgery, University of Minnesota.