
Abstract
Introduction:
Osteoporosis remains an undertreated disease entity causing substantial morbidity and mortality. Proximal humerus fractures are a common sentinel fracture, providing an opportunity to intervene with antiresorptive therapy before more subsequent fractures occur. Despite the success of programs aimed to improve postfracture osteoporosis recognition and management, less than 30% of patients presenting with a fragility fracture are diagnosed or treated for osteoporosis nationally. Further elucidation of diagnosis and management of osteoporosis following humerus fracture is warranted.
Methods:
This study is a retrospective cohort review intended to demonstrate the current state and clinical import of osteoporosis diagnosis and management following a humerus fracture at a large academic tertiary care center without an established secondary fracture prevention program. All patients 50 years of age or older who presented with a new humerus fracture between 2008 and 2014 were included. Outcome measures included: The initiation of antiresorptive therapy or screening before fracture, within the year following fracture, or not at all.
Results:
One thousand seven hundred unique geriatric patients were seen for humerus fractures. Nineteen percent of these patients (n = 324) were already on an antiresorptive medication. Three percent of previously untreated patients were started on antiresorptive therapy during the year after their fracture, with 31 or 2% of untreated patients starting at any subsequent point. Seventy-six percent of patients (n = 1301) were never prescribed antiresorptive therapy.
Discussion and Conclusion:
In the absence of a dedicated program to improve secondary fracture prevention following minimal trauma spinal fractures, recognition and treatment of osteoporosis in patients remained inadequate over time despite numerous calls to action on the topic in the orthopedic literature and public health initiatives. Undertreatment of osteoporosis puts patients at increased risk for additional fractures. This study underscores an opportunity to improve bone health by aggressively screening for and treating osteoporosis in geriatric humerus fracture patients.
Introduction
Despite readily available treatments and screening protocols, osteoporosis remains an underrecognized and undertreated disease. Patients who develop fragility fractures are at increased risk of developing future fractures and should be promptly evaluated for osteoporosis. 1,2 Proximal humerus fractures are among the most common fracture sites in men and women. According to a Canadian multicenter osteoporosis study, humeral fractures are the fourth most common initial site for fragility fractures in women. 3 They are associated with both increased age and decreased bone mineral density. 3 In their 2014 call for the clinical diagnosis of osteoporosis, the National Bone Health Alliance listed proximal humerus fractures as a pathognomonic fragility fracture that should trigger a clinical diagnosis of osteoporosis. 4 Although these guidelines have not been universally accepted, proximal humerus fractures should trigger bone health evaluation and subsequent management.
The most effective approach to treating osteoporosis is to initiate treatment prior to significant bone mineral density loss; however, this is difficult to implement in asymptomatic patients. Therefore, proper implementation of pharmacological therapies as secondary prevention could mitigate the aforementioned burdens. 5 Therapeutic antiresorptive interventions, such as alendronate, risedronate, zoledronic acid, and denosumab, have been shown to be beneficial first line therapies for hip, nonvertebral, and vertebral fractures. 6 These Food and Drug Administration (FDA)–approved medications have been shown to reduce the risk of future nonvertebral fractures by approximately 50%. 7 Despite the efficacy of available medications, there is widespread international consensus that appropriate recognition, screening and management of osteoporosis is suboptimal. 8 -10
Although proximal humerus fractures may be thought of as more benign fractures compared to hip fractures, they nonetheless present an opportunity for intervention to lower the risk for future fragility fractures. One strategy to close this gap in care is implementation of a fracture liaison service (FLS). Mclellan et al report the success of FLS implementation over an 18-month period in a large health care system. Forty-six hundred patients were evaluated for fractures of the hip, wrist, and foot. Of those patients, 75% were recommended for BMD testing and 82% of those patients were found to have some degree of osteoporosis or osteopenia. 11 Despite the efficacy of programs like FLS, most patients’ osteoporotic needs remain unattended. Medicare data indicate the majority of women aged 65 to 85 who sustain a fracture are neither evaluated nor treated for osteoporosis in the year following fracture. 12
To date, no major study has been performed in the United States to analyze or address the osteoporosis care gap following humerus fractures in an institution without an existing FLS. A nationwide retrospective cohort study was performed in Korea by Kim et al in which they recognized that only 1.8% of patients received osteoporosis screening or therapy following a proximal humerus fracture. 13 Anecdotal evidence in the United States suggests similar rates at many major institutions. Cuddihy et al performed a similar study and acknowledged the care gap; however, their study was limited by a smaller patient population. 14 Limited data are available on the rates of osteoporosis screening and treatment following proximal humerus fractures in the United States at institutions lacking established secondary prevention efforts, such as FLS programs. Here, with a large patient population, we seek to better delineate diagnosis and treatment institution rates following humeral fracture at an academic level 1 trauma center with 6 affiliated community hospitals.
Methods
A retrospective cohort review was performed to demonstrate the post acute management of osteoporosis after incident humerus fractures in a large regional health care center prior to establishment of a secondary fracture prevention program. Data were extracted from the electronic medical records of all patients seen for a humerus fracture at a level 1 trauma center and its 6 community hospitals. Medical and pharmacy records were reviewed for all patients who presented to the emergency department after the age of 50 with a primary proximal humerus fracture using International Classification of Diseases, Ninth Revision (ICD-9) codes. Inpatient and outpatient medical records over a 7-year period (2008-2014), covering over 1000 physicians and almost all dual-energy X-ray absorptiometry (DEXA) scanners in the region were reviewed. Only patients who presented with their first humerus fracture were included in this study. Database was queried for ICD-9 prefix 812. The study period was selected based on the institution of a new medical record system in 2008 and terminated in 2014 which was 2 years before implementation of the International Classification of Diseases, Tenth Revision coding system.
The relative frequency of high-energy mechanisms of injury within this database was assessed using 2 methods. First, ICD-9 codes for high-energy mechanisms, such as gunshot wounds and car accidents were examined. The frequency of high-energy mechanisms was also assessed indirectly by determining the frequency of additional fractures recorded at the emergency department visit for the incident humerus fracture. Rib fractures were analyzed separately because of their relative prevalence and because they often occur through low-energy mechanisms.
To quantify osteoporosis screening in individuals presenting with incident humerus fractures, rates of DEXA scanning were assessed at several time points relative to fracture. All DEXA scan results were pulled from the system for individuals with incident humerus fractures. Time from DEXA scan to incident humerus fracture was assessed with a time lapsed variable. Dual-energy X-ray absorptiometry scans completed within 2 years prior to incident fracture were surveyed. DXA scans within 1 year following fracture among individuals without a DEXA scan in the prior 2 years were likewise recorded and considered part of appropriate management post fracture.
Treatment rates were assessed by measuring the rate of prescribing of FDA-approved medications for osteoporosis both before and after fracture. Food and Drug Administration–approved medications in the study period included bisphosphonates, teriparatide, denosumab, raloxifene, and calcitonin. Prior prescription of any of these FDA-approved medications was counted as a prior treatment for osteoporosis. Individuals who had not previously received a prescription for one of these medications were considered treatment-naive for osteoporosis. We also recorded cases that were first prescribed an osteoporosis medication for more than 1 year following their incident humerus fracture.
To assess whether treatment rates improved over time among treatment-naive humerus fracture patients, patients were subdivided by the year of their incident fracture, and the rate of new treatment among treatment-naive individuals within these annual cohorts was calculated.
Simple logistic regression was used to test for statistically significant trends in this rate over time. Rates of calcium and vitamin D supplementation were assessed both before and after fracture. An individual’s first recorded prescription for both calcium and vitamin D supplementation was recorded and compared to their incident fracture date to determine the timing of starting supplementation relative to fracture. A composite measure of treatment with either FDA-approved medications or calcium and vitamin D supplementation was calculated by examining the percentage of patients receiving treatment (1) prior to fracture, (2) within 1-year post fracture, and (3) greater than 1-year post fracture.
Results
Between 2008 and 2014, 1700 patients (50 years of age or older) presented to the emergency department with a humerus fracture. The mean age of this patient population was 72 years old with a standard deviation of 12.3. Seventy-six percent of these patients were female and 24% were male. The race breakdown was 94.4% Caucasian, 4.1% African American, and less than 1% all other.
Of the 1700 patients seen in the emergency department with a humerus fracture, 39 (2.3%) patients had received DEXA screening up to 2 years prior to their incident fracture (Figure 1). Sixteen (0.94%) patients received a DEXA 0 to 1 year following fracture. Nine (0.53%) patients received their first DEXA screening greater than 1 year following their incident humerus fracture. Overall, 96.2% of all patients throughout the time period of this review never received a DEXA scan.

The proportion of patients screened for osteoporosis at various time points relative to incident fracture; 2.9% of patients received dual-energy X-ray absorptiometry (DEXA) screening 2 years prior to incident fracture, 0.94% received a DEXA scan 0 to 1 years s/p fracture, and 0.53% received a DEXA scan greater than 1 year s/p fracture.
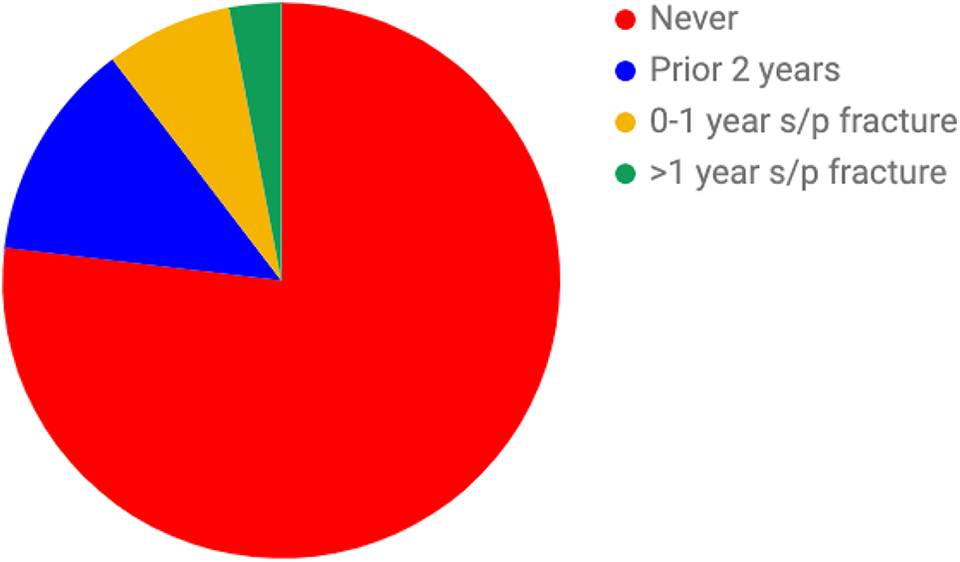
Three hundred twenty-four patients, representing 19.1% of the total population, had already been on pharmacotherapy 2 years prior to their incident humerus fracture. Of the patients who had never been prescribed osteoporosis medication before, 125 (2.4%) were subsequently prescribed pharmacotherapy 0 to 1 year following their fracture. Thirty-one (1.8%) of patients who were seen for an incident humerus fracture were prescribed pharmacotherapy greater than 1 year post fracture. Overall, 76.5% of the total patient population never received FDA-approved pharmacotherapy during the study period (Figure 2).

The rates of pharmacotherapy at various time points relative to incident humerus fracture; 19.1% of patients were started on pharmacotherapy within 2 years prior to incident fracture, 2.4% were begun on pharmacotherapy 0 to 1 years s/p fracture, and 1.8% were started on pharmacotherapy greater than 1 year after incident fracture.
Of the 1700 patients seen, 217 (12.8%) were supplemented with vitamin D and calcium up to 2 years prior to their incident humerus fracture. Of the patients who were never given vitamin supplementation prior to their fracture, 125 (7.4%) were given vitamin D/calcium 0 to 1 year following their ER visit. Fifty-one (3%) of supplement-naive patients received supplementation greater than 1 year following their humerus fracture. In total, 76.9% of all patients who reported to the ED with a humerus fracture never received vitamin supplementation throughout our study period (Figure 3).
Rates of calcium and vitamin D supplementation at various time points relative to incident humerus fracture; 12.8% of patients were already prescribed vitamin supplementation up to 2 years prior to incident fracture; 7.4% were prescribed vitamins 0 to 1 year s/p fracture; and 3% were prescribed vitamin supplementation greater than 1 year s/p fracture.
Four hundred seventeen (24.5%) patients were treated with prescriptions or vitamins up to 2 years prior to their incident humerus fracture. Of the patients who were never treated prior to their fracture, 120 (7.1%) were treated 0 to 1 year following their fracture. Seventy-five (4.4%) treatment-naive patients were treated at some point 1 year after their humerus fracture. Overall, 64% of all patients seen for a humerus fracture were never prescribed an FDA-approved pharmacotherapy and/or vitamin supplementation at any point in the study period (Figure 4).
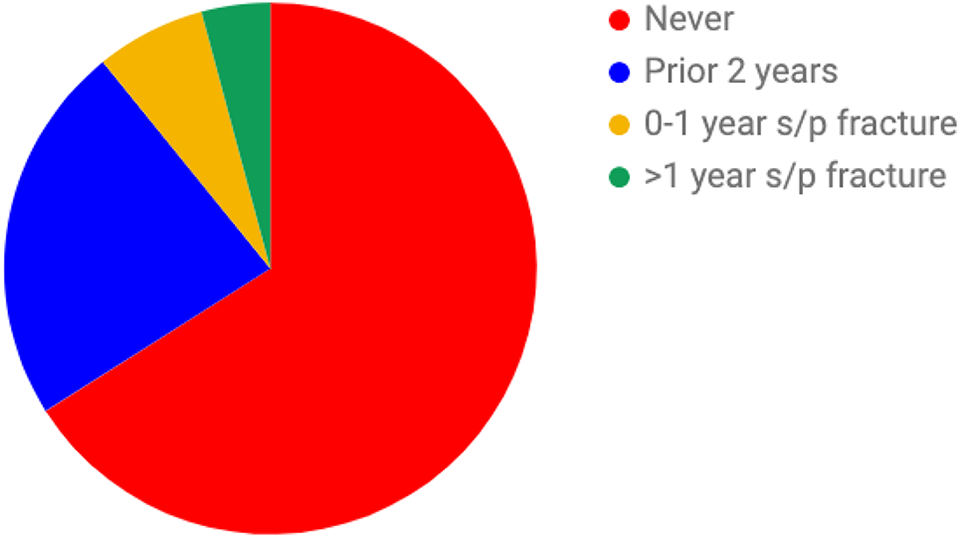
Rate of either pharmacotherapy or vitamin supplementation at various time points relative to incident humerus fracture; 24.5% were started on some medication up to 2 years prior to their incident fracture; 7.1% were started on some medication within 1 year after incident fracture; and 4.4% were started greater than 1 year after.
Unfortunately, we noted that there was no significant trend in improvement of treatment over the study period (Figure 5; Table 1). Regression analysis demonstrated a statistically insignificant 42% reduction (P = .13) in treatment rates from 2008 to 2014.
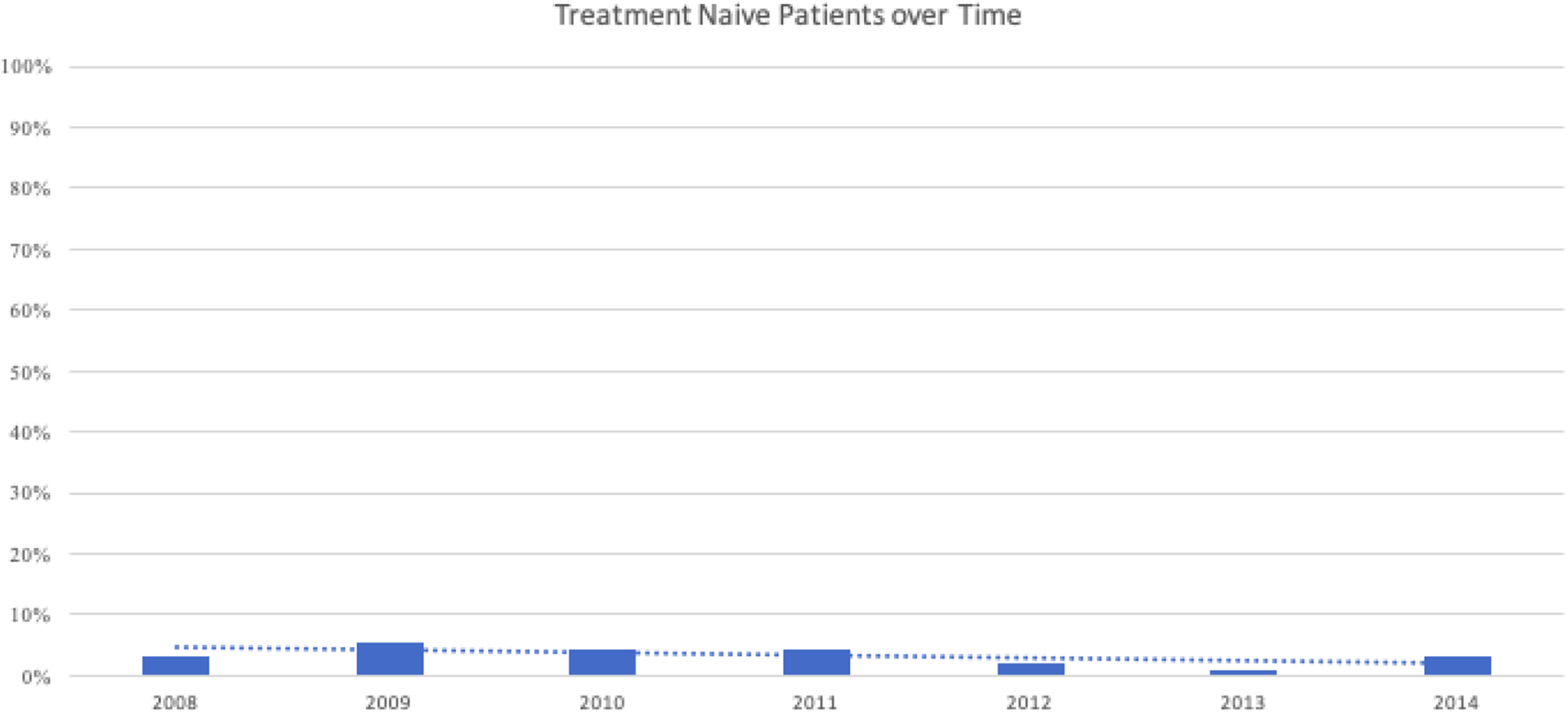
Percentage of patients who had never been treated for osteoporosis who were started on therapy following incident humerus fracture during each year of this study. Regression analysis shows a statistically insignificant decrease in treatment initiation rates.
The Percentage of Treatment-Naive Patients Who Were Started on Treatment After Incident Humerus Fracture at Each Year of This Study.

Discussion
There is little debate that patients who sustain proximal humerus fractures should be evaluated for osteoporosis and appropriate treatment should be initiated. Our data indicate that diagnosis and treatment of osteoporosis was insufficient in this vulnerable high-risk population. Of the 1700 patients who were seen for a new humerus fracture in the emergency department, 98% of patients never received DEXA screening following their incident fracture. Of note, the hospital system operates most of the regional scanners. When accounting for the patients who received scanning 2 years prior to and/or 1 year following injury, only 55 (3.2%) patients received a DEXA which could have directed the treatment of their likely underlying osteopenic state. In 2001, the National Institute of Health concluded that, currently, BMD measurements using DEXA and the World Health Organization’s T-score criteria should be used to establish a definitive diagnosis of osteoporosis. 15 Given this criteria, it is evident that the vast majority of the patients in this study failed to receive adequate diagnostic workup for osteoporosis.
We found that in addition to weak diagnostic workup, the institution of appropriate treatment rates was low. Approximately 77% of patients never received vitamin D or calcium supplementation at any point in this study. We readily acknowledge that the predictive value of vitamin and mineral supplementation for osteopenic/osteoporotic patients may be reduced as patients and clinical staff do not always carefully record nonprescription supplements. Therefore, it is possible that we underestimate the rate of vitamin and mineral supplementation.
That being said, the role of vitamin D and calcium supplementation for the management of osteoporosis has been demonstrated. Moreno et al demonstrated a statistically significant risk reduction in vertebral and nonvertebral fractures when patients were given vitamin supplementation (calcium with vitamin D) compared to a placebo. 16 This underscores the importance of initiating vitamin therapy in patients diagnosed with osteoporosis. The efficacy of vitamin therapy is greatest in patients who are deficient. A significant proportion of the US population is deficient in vitamin D at baseline. 17 The observed low rate of supplementation in this study suggests that we are undertreating this population.
We postulate that using the introduction of FDA-approved prescription pharmacotherapy is a more accurate metric of osteoporosis treatment. When antiresorptive agents and vitamin supplementation are analyzed together, only 612 (36%) patients in our population received any sort of treatment at any time point in our study. Of the 1700 patients in our populations, 399 (33%) patients were prescribed pharmacotherapy either before or after their incident humerus fracture. A meta-analysis conducted by Bolland et al demonstrated that most pharmacotherapy measures (including bisphosphonates and denosumab) resulted in a long-term risk reduction for future fractures. 18 These data indicate that providers are missing a key pharmacological intervention that could help reduce the mortality associated with their osteoporotic state.
The time period of this study overlapped with the President’s Decade on Bone Health in the United States, which aimed to promote bone health and prevent future fractures. 19 Additionally, several initiatives such as Own The Bone and 2million2many were designed to raise awareness and launch initiatives to address deficiencies in osteoporosis recognition and management. 20,21 When FDA-approved pharmacotherapy initiation rates in treatment-naive patients were analyzed over time, we saw decline from 2008 to 2014. Although this trend was statistically insignificant, it is suggested that treatment rates during this time period did not improve, despite increasing awareness of this care gap and an emphasis on the critical nature of bone health by the surgeon general. 19 Our study indicates that treatment rates did not improve despite increasing public awareness
One limitation of our data set is the lack of injury mechanism coding by the emergency department, which means that some of the humerus fractures included in our data might have been due to a traumatic event. Although there are preexisting ICD-9 modifiers that correspond to certain mechanisms of injury, these were not analyzed because the mechanism of injury data set was felt to be inconsistently coded. Nonetheless on review of outpatient demographics, geriatric female patients are more likely to sustain osteoporotic fractures due to low-energy mechanisms and should be worked up for osteoporosis no matter the mechanism.
Additionally, our data set includes providers from a single academic tertiary care health care system with 6 affiliated community hospitals, which may limit generalizability. Unfortunately, in an unpublished survey, regional treating physicians agreed that the conclusions drawn from this study accurately depict the pattern of osteoporosis management. Most physicians cited time limitations as the primary factor preventing them from addressing the underlying disease process in the setting of osteoporotic fractures. Another frequently cited reason for undertreatment had to do with disagreement on which specialty should be instituting treatment.
This underscores the need for implementation of a dedicated multidisciplinary FLS to improve diagnosis, appropriate management, and decrease health care cost by decreasing morbidity in this vulnerable population.
Conclusion
There is a consistent gap in the recognition and management of osteoporosis in patients sustaining proximal humerus fracture. Proximal humerus fractures in the geriatric population are an opportunity to institute treatment which has been shown to decrease subsequent fractures and their resultant morbidity. Instituting a FLS to manage these patients may be the most efficient step in improving bone health and improving long-term osteoporosis outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.