
Abstract
Introduction:
Participants who sustain a fragility fracture are at increased risk for subsequent fractures. Despite the consequences of recurrent fractures, bone mineral density (BMD) testing and treatment rates for osteoporosis after a fracture remain low. The New York University (NYU) Langone Osteoporosis Model of Care was developed to identify women at increased risk for recurrent fractures and to reduce the rates of subsequent fracture through patient and physician education.
Methods:
Women aged 50 years and older who had a fracture and received their care at NYU affiliated hospitals were contacted via mail after discharge. Participants were provided educational materials explaining decreased bone strength and its possible relationship to their fracture and were asked to complete a questionnaire. One year postfracture, participants were sent follow-up questionnaires requesting their most recent fracture treatment and BMD information. Educational material was also provided to the treating orthopedic surgeons.
Results:
Overall, 524 patients were contacted and 210 (40%) enrolled. By the end of 24 months, 92 participants completed their 1-year questionnaire (44% of the enrollees). Forty-two (46%) participants had undergone new BMD testing and 37 (40%) were receiving antiresorptive medications, including 6 (6%) who had not been prescribed these medications before enrolling in the program.
Conclusions:
The Osteoporosis Model of Care is a simple and cost-effective educational program, which improved comprehensive fracture care in an actual clinical setting. Patient enrollment remains a challenge in implementing the program. Our program highlights difficulties in providing community-dwelling participants with appropriate postfracture care. With increasing concern among the public regarding the use of bone strengthening medications and continued low postfracture treatment rates, educating patients with high fracture risk is critical to reducing the rate of subsequent fracture. Our Model of Care Program demonstrates both the success and limitations of a postfracture educational approach using discharge diagnosis data to identify patients with fracture.
Keywords
Introduction
Osteoporosis is a systemic disorder of bone characterized by low bone mass and compromised bone strength resulting in increased fragility and susceptibility to fracture. 1 It is the most common disease of bone, and its consequences (fracture) impose significant social and economic burdens on affected individuals and the health care system. More than 2 million osteoporotic fractures occur annually in the United States, resulting in over US$17 billion in costs. Osteoporotic fracture rates and their costs are expected to rise to 3 million and US$25.3 billion, respectively, by the year 2025. 2 It is estimated that 40% of American Caucasian women and 13% of American Caucasian men older than 50 years will experience at least 1 clinically apparent fragility fracture in their lifetime. 3 Patients who survive hip fractures are often faced with the sudden and permanent loss of mobility and functional independence. 4,5 Both hip and vertebral fractures are associated with increased mortality rates, particularly in the first-year period following the fracture. 6
Identifying women who are at increased absolute fracture risk is critical to developing rational and cost-effective treatment strategies that will reduce the incidence of fragility fractures. Patients with previous osteoporotic (fragility) fractures are at a particularly increased risk for sustaining subsequent fractures. 7,8 Several studies have shown that the greatest increase in all fracture rates occurred within the first year after either incident vertebral or nonvertebral fractures. 9 –12
Over the past decade, advances in imaging and the introduction of a number of effective pharmacologic and nonpharmacologic modalities have made it possible to identify and treat individuals at increased risk for fractures. 13 –18 Unfortunately, the majority of patients who have sustained a fragility fracture never undergo bone density testing or receive bone strengthening medications. 19 Most studies report rates of 10% to 25% for testing and treatment of osteoporosis after sustaining an osteoporotic fracture. 20 –24 Furthermore, many patients with fragility fracture do not appreciate the possible association between their fracture and their underlying bone strength. 25,26 This has resulted in osteoporosis management that is often ignored, overlooked, or fragmented. 27
To date, the most significant predictor of physicians’ decision to treat patients with bone strengthening medications following a fracture has been a low bone mineral density (BMD) test result. 28 This finding highlights the importance of bone density testing in influencing physician behavior. Several studies have attempted to address this need by utilizing methods aimed at improving physician and patient awareness through educational tools, patient reminders to schedule follow-up visits, and summaries of treatment options using telephone, mail, and face-to-face interventions. 29 –33 Others have involved more complex and expensive care coordination techniques. 34 –37 Despite these different approaches, most patients do not receive indicated bone strengthening medications after sustaining a fragility fracture.
The New York University (NYU) Langone Medical Center Osteoporosis Model of Care has been developed to identify those patients at greatest risk for sustaining a fracture: women older than 50 years who present with fragility fracture. The goals of the program are to increase the number of such patients who receive BMD testing and if indicated receive bone strengthening medications through an educational program initiated several weeks after the acute fracture event. The patients in our study are identified according to discharge data from the 2 inpatient and 2 ambulatory sites that care for patients with fractures. Although contacting patients at the time of fracture may have improved patient compliance, that approach was not practical for our population, which receive acute fracture care in geographically separate sites. Patients are educated about the possible relationship between their fracture and decreased bone strength and are encouraged to discuss fracture risk management with their physicians. Additionally, the program has been structured to involve the treating orthopedist as an intermediary to reinforce the value of the program and the reasons for which it has been developed. In a related aim, the Model of Care Program encourages the orthopaedic surgeon to integrate a bone health screening program into their postfracture care treatment protocol. Finally, the program has been created with the hope that it would be replicated and used by other institutions so that it might have a broader impact on increasing the number of at-risk patients who receive appropriate bone strengthening treatments. Such treatment could help reduce the incidence of recurrent fractures, including those associated with significant morbidity, increased mortality, and large societal resource expenditures.
Materials and Methods
Patients
The Model of Care program identified patients discharged from the NYU Medical Center’s Tisch Hospital, NYU Hospital for Joint Diseases (NYU HJD), and Rusk Rehabilitation Institute from November 2006 to October 2009. Patient’s discharge information was provided monthly by the Finance Department within 20 days after the end of the previous month. Following review of the discharge data, a packet of educational material, questionnaires, and a self-addressed stamped envelope was mailed to the identified female patients aged 50 years and older who had sustained a fracture and received their fracture treatment at any of the above-mentioned facilities. We included lower leg, femur (nonhip), hip, pelvis, vertebral, forearm, wrist, and humerus as fracture sites eligible for inclusion in our program as has been done by other postfracture programs.
Interventions
The initial package mailed to patients included an introductory letter, a 1-page questionnaire, and osteoporosis-related educational material. Follow-up calls were made 2 weeks later to patients who had not returned their questionnaires. Once verbal contact was established, the Model of Care program was explained and discussed with the patient. The patient was asked to fill out the questionnaire and return it. This first questionnaire evaluated the patient’s diagnosis and reviewed their osteoporosis treatment history, as well as any history of other fracture(s) prior to their hospitalization. The program’s research coordinator then contacted the treating orthopaedic surgeons to inform them that their patients were candidates for the program and to enlist their support in enrolling the patients. Educational materials describing the Model of Care Program were provided to the surgeon on request.
A second mailing was subsequently sent to all nonrespondents, containing only the introductory letter and the 1-page questionnaire. At the time of the second mailing, the patient’s surgeons were again contacted to alert them that their patients had not answered the questionnaire, to encourage them to emphasize to their patients the importance of bone strength in fracture prevention, and to solicit their support in encouraging their patients to participate in the Model of Care Program.
Patient responses to questionnaires were entered into the Model of Care database. Whenever a primary care physician/personal orthopedist was identified by the patient, a letter explaining the program’s objectives and goals was sent to that physician in order to reinforce the goals of the program and the importance of patient education to their care of patients with fracture.
A second questionnaire was sent to each patient, 6 months and 1 year postfracture. The 6-month questionnaire was developed to evaluate patient responses to the program structure and whether they found the educational content useful. The annual questionnaire solicited information regarding the patients’ “bone health” including new fractures, diagnostic studies, and information on any bone strengthening medications they have or had been using.
Results
A total of 625 patients who had sustained a fracture were identified, and 524 were contacted by the Model of Care Program. Of these patients, 210 (40%) responded to the initial questionnaire and were enrolled in the program. The age breakdown of the respondents was similar to that of all 625 of the qualifying patients (Table 1).
Baseline Characteristics.

The most common incident fracture of respondents was an ankle fracture (30%). Table 2 lists all fracture sites and their incidence rates. Forty-one percent of the participants had a history of a prior fracture. At the time of the initial questionnaire, 57% of respondents stated that they had been told that they had osteoporosis or osteopenia, 79% had a previous bone density test, and 40% were taking antiresorptive medications. Table 3 lists aspects of the bone health history of all participants, and Table 4 lists the relevant medical history of those enrollees who were not being treated for osteoporosis at the time of their recent fracture.
Incident Fractures Among Respondents.

Bone Health History of Enrollees.
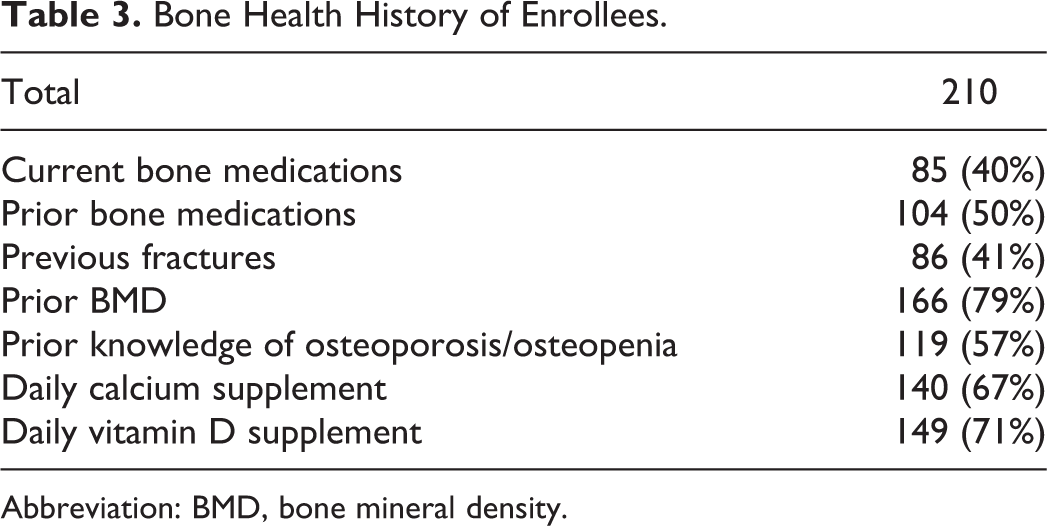
Abbreviation: BMD, bone mineral density.
Bone Health History of Enrollees Untreated for Osteoporosis at the Time of Fracture.

Abbreviation: BMD, bone mineral density.
Over 90% of enrollees in the Model of Care program responded to the 6-month questionnaire regarding their impression of the educational information they had received regarding osteoporosis prevention/treatment. Program enrollees overwhelmingly reported that the educational material provided to them was very helpful and that they were pleased that someone was taking the time to educate the public about fractures and osteoporosis.
By October 2009, 183 of the initial enrollees had been sent the 1-year follow-up questionnaire, of which 92 (50%) responded. Table 5 lists the age ranges of the follow-up respondents. Excluding the program’s patients who already had BMD testing within the previous 2 years, 46% of enrollees underwent new bone density testing in their first postfracture year. Forty percent of patients were receiving antiresorptive medications, including 6% who had not been prescribed these medications before the intervention. Five (5%) patients had a new fracture during the assessment interval (Table 6).
Ages of Follow-Up Respondents.

Follow-Up Data.

Abbreviation: BMD, bone mineral density.
Discussion
The impact of osteoporosis and fragility fractures has been detailed thoroughly, both from personal and public health viewpoints. 2 –6 Nevertheless, many postmenopausal women who sustain a fracture neither undergo appropriate bone density testing nor are advised to start bone strengthening medications as part of their postfracture medical care. 23 –28
Patients with previous fragility fractures are at significantly increased risk for sustaining another fracture, particularly within the first year after an incident fracture. 7 –12 Johnell et al examined the pattern of fracture risk over 5 years following a prior fracture at the spine, shoulder, or hip in a cohort of over 1900 Swedish patients. Such patients had a significant increase in risk for subsequent fracture immediately after a fracture compared to the general population, with relative risks as high as 18 for hip fractures and 7.2% total recurrence rate within the first year. 9 In a 2001 study, Johnell et al followed over 28 000 patients admitted for vertebral fractures, with clinical assessments at 6 months and 4 years postfracture. Again, an increased incidence in recurrent fractures of all types was noted at 6 months, with relative risk ratios as high as 32. Thereafter, fracture incidence declined toward but did not reach baseline risk. 10 In evaluating 2725 postmenopausal women who were randomized to placebo groups in 4 large osteoporosis treatment trials, Lindsay et al noted that among untreated patients with a new vertebral fracture, the risk of an additional vertebral fracture during the following year was nearly 20%. 11 Huntjens et al studied 1921 patients who had nonvertebral fractures and found that the absolute risk of recurrent nonvertebral fractures was 17.6% over 5 years and was once again highest within the first year with a 6.4% total recurrence rate. 12
Previous attempts at improving the percentages of patients who undergo bone density testing and/or receive bone strengthening medications have been encouraging but inadequate. Hawker et al identified patients with fragility fracture having no prior diagnosis of osteoporosis and informed them, as well as their physicians, of their osteoporosis risk via standardized letter. A 3-month phone interview showed an odds ratio of 5.22 for a new bone density test, but patients were not more likely to receive a treatment recommendation. 33 Cranney et al performed a randomized trial in which both patients and physicians were contacted by mail at 2 weeks and 2 months after a wrist fracture. Patients were reminded to follow-up with their primary care physician and were given a checklist of fracture risks. Physicians were given an educational tool and treatment algorithm. They noted that 53% of the intervention group had new BMD testing as opposed to 26% of usual care controls, with 28% versus 10% being started on new medications. 32 Majumdar et al have used similar interventions in several randomized trials after incident wrist fractures, using telephone-based patient education and mailed guidelines to physicians. Bone mineral density testing rates were higher in the intervention groups (52% vs 18%), but the treatment effect was again less robust (22% vs 7%). 31 Feldstein et al created an intervention based on patient-specific clinical guideline advice to the primary care provider via electronic medical record message plus an educational letter mailed to the patient. In their study, 43% of intervention patients underwent new BMD testing, as compared to 6% of the usual care patients. They utilized questionnaires to the patient for enrollment and had a 64% response rate. 37
In order to improve postfracture bone density testing rates and increase the number of patients who receive indicated bone strengthening medications, the Osteoporosis Model of Care Program was developed. It is designed to identify those at increased risk for sustaining a subsequent fracture and to optimize postfracture care by providing educational materials to both patients and their treating orthopaedic surgeon.
The enrollment goal of the Model of Care Program was projected at a minimum of 50% of eligible participants, but we did not reach that level as only 210 of the 625 (40%) patients elected to complete the initial questionnaire. A significant proportion of our participants (79%) had undergone bone density testing at some time before sustaining their incident fracture, and 40% of patients were using bone strengthening medications at the time of their fracture. Forty-one percent of our enrollees had a history of a previous fracture, a figure similar to the number reported by Roux et al from a European cohort of 3402 women taking osteoporosis medications. 38 The relatively high percentage of women in both our and Roux et al’s studies suggest that both cohorts involved populations at increased fracture risk.
Sixty percent of enrollees were not using any bone strengthening medications at the time of their incident fracture, although 20% of them had used such treatment in the past. Bessette et al reported on a group of 738 patients who had sustained a fragility fracture while not being treated for osteoporosis and found that 8.5% had been prescribed osteoporosis medication in the past. 19 The Model of Care patients who were not being treated at the time of their fracture were more likely to have had a previous bone density than were the patients reported by Bessette et al (70% vs 31.4%), although similar percentages had a fracture prior to enrollment (34% vs 28.3%). The untreated Model of Care patients were also more likely to be taking calcium (51% vs 39%) and vitamin D (59% vs 38%) than the Bessette’s Canadian cohort (Table 4).
Ninety-five of the 183 patients from the original cohort followed up at 1 year (50%). As a result of our intervention, 46% of the enrolled participants underwent new BMD testing within the year after their fracture, a finding similar to that found in several randomized controlled trials involving osteoporosis educational interventions. Forty percent of enrollees were taking antiresorptive medications after the first year, with 6% starting their medication after the intervention. This figure is also consistent with those reported in other patient education-based studies. 35 –37 The small increase in treatment rates after the intervention may be explained by the high baseline rate of treatment in the Model of Care patients. The rate of fracture recurrence among those who were followed at 1 year (5%) was in line with several previous studies, 9,12,38 but the significance of this finding is mitigated by the relatively small number of patients involved in the program. The relatively high number of ankle fractures (not traditionally considered a fragility fracture) was also seen in a Danish study involving subsequent fractures over a 10-year period of time. 39
The Model of Care Program is not a randomized controlled clinical trial, however, the demographics of enrollees has allowed comparisons with previous osteoporosis intervention studies. As with a number of prior efforts, patient enrollment has been a major challenge in implementing our program. In our program, only 210 women (40% of those contacted) responded to the initial questionnaire and were enrolled in the Model of Care. Specific patient issues with enrollment may have included patient disinterest in the program or a feeling of being too old to participate. Some patients may not have wanted their primary care physicians and/or orthopedists contacted. Others were simply not able to be reached due to incorrect phone numbers and addresses. Relying on patients to answer questionnaires from home instead of at physician appointments may have decreased compliance. The need to get patient “buy in” has increased appreciation of the need for more aggressive patient follow-up and how critical enlisting the involvement of the referring orthopaedic surgeon is to the program’s success.
Despite the ongoing difficulties with patient enrollment, the Osteoporosis Model of Care program demonstrates that it is possible to create a simple and effective educational program that can be easily replicated, which improves the standard of comprehensive fracture care. As with other programs designed to reach patients at increased fracture risk, modifying traditional physician and patient “medical behavior” remains a significant hurdle. Among the program’s underlying hypotheses was the obvious need to make both the orthopaedic surgeons and their patients who have sustained a fracture aware of the possible connection between their fracture and their overall bone strength.
We hope that the NYU Langone Medical Center Osteoporosis Model of Care Program can serve as a template for other health care institutions who wish to develop a cost-effective system that improves the postfracture care of high-risk postmenopausal women and reduces the incidence of subsequent fractures in this population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The NYU Langone Medical Center Osteoporosis Model of Care Program was financially supported by the Fan Fox and Leslie R. Samuels Foundation.