
Abstract
Introduction:
Cognitive impairment can hinder a fracture patient’s capacity to consent to surgery and negatively impact their postoperative recovery and rehabilitation. National guidelines recommend screening for cognitive impairment upon admission, and the Abbreviated Mental Test Score (AMTS) is a commonly used tool for this. This project aimed to assess current practice regarding documentation of AMTS among frail fracture patients upon admission and to improve AMTS documentation following a simple intervention.
Methods:
Baseline data were obtained by inpatient chart review throughout November to December 2018 in a district general hospital with emergency fracture services. All patients admitted with a fragility hip fracture and patients over 65 years with any fracture were included. National guidelines and baseline results were then distributed among junior doctors. Following an intervention, further data were collected throughout January to February 2019.
Results:
Preintervention, 40 suitable patients (mean age: 82 years) were identified; 9 (22.0%) of whom had an AMTS recorded upon admission. Among the hip fracture subgroup (n = 25), 7 (26.9%) had an AMTS recorded. Postintervention, 39 patients (mean age: 80 years) were identified; 15 (38.5%) of whom had an AMTS recorded. Among the hip fracture subgroup (n = 30), 11 (36.7%) had an AMTS recorded. Statistical analysis demonstrated a significant improvement in AMTS documentation both among the overall cohort (P = .001) and hip fracture patients (P = .019). No significant association was found between AMTS documentation and patient age (P = .566), grade of admitting doctor (P = .058), or prior cognitive/mental health disorder (P = .256).
Discussion:
A small yet significant improvement in AMTS documentation among elderly/hip fracture patients was observed following distribution of educational material. Further work should explore the effect of cognitive impairment on outcomes related to orthopedic injuries beyond hip fractures.
Introduction
Impaired cognitive function is common among elderly fracture patients and can be seen in a spectrum of forms, ranging from chronic dementia, acute delirium, or acute or chronic confusional states. Lower cognitive status upon admission has been previously associated with poorer functional rehabilitation among hip fracture patients. 1 Patients with dementia have been shown to be at higher risk of hip fracture than their cognitively intact counterparts, 2 while fracture history may be an independent risk factor for developing dementia among patients aged over 65 years. 3 Thus, it is possible that an elderly patient may first be identified as having underlying cognitive impairment upon presentation with a fracture.
Both acute delirium and underlying dementia can affect a patient’s capacity to consent for surgery, hinder their postoperative recovery, and affect their discharge destination. Perioperative delirium affects approximately one-third of patients with hip fractures 4 and has been associated with longer inpatient stays and higher 1-year mortality rates. 5 Hip fracture patients with prediagnosed dementia have been shown to be significantly more likely to develop delirium postoperatively. 5
Thus, in 2012, the British Orthopaedic Association Standards for Trauma and Orthopaedics (BOAST) guidelines stated that one should “Assess patient’s risk of delirium or dementia by actively looking for cognitive impairment when patients first present with hip fracture and perform regular re-assessment.” 6 More recently, the British Orthopaedic Association extended their guidelines beyond hip fractures, stating that all elderly or frail orthopedic trauma patients should routinely be assessed using a validated delirium assessment tool such as the 4AT. 7
Numerous scoring systems have been described in acute and chronic cognitive impairment, documentation of which can aid in the detection of cognitive impairment upon admission and for subtle changes in cognition during the inpatient stay. Folstein’s Mini-Mental State Examination 8 is a tool used to estimate the severity of cognitive impairment and to follow the course of cognitive changes in a patient over time. However, the 30-point questionnaire can be somewhat cumbersome and thus many nonspecialists prefer the Abbreviated Mental Test Score (AMTS) as described by Hodkinson. 9 The AMTS comprises a series of 10 questions; a score of less than 6 is generally regarded to be suggestive of impaired cognition. 9 However, the AMTS is felt to be too crude compared with other more comprehensive scales to monitor for subtle changes in cognition over time. 10
The AMTS is historically in widespread use throughout the United Kingdom including Northern Ireland. Although the AMTS is also not typically regarded as a validated delirium tool, serial AMTS testing has been shown to be helpful in identifying acute cognitive dysfunction in the elderly population, 11 with a decline of 2 or more points having high sensitivity and specificity for diagnosing postoperative delirium. 12 The function of the 4AT, as recently suggested by the British Orthopaedic Association, and the AMTS has been found to be comparable in the hip fracture population. 13 The AMTS is commonly used in Northern Ireland in the clinical setting 14 and has also been used in numerous studies assessing change in cognitive function among hip fracture patients. For example, Odor et al compared the impact of regional anesthesia on pre- and postoperative AMTS, 15 and Tahir et al used the AMTS on admission to assess baseline cognitive function when screening for postoperative delirium. 5 Thus, it has been suggested that, due to its brevity and sensitivity, the AMTS is a very useful screening test for elderly trauma patients to assess for impaired cognition of any cause. 16
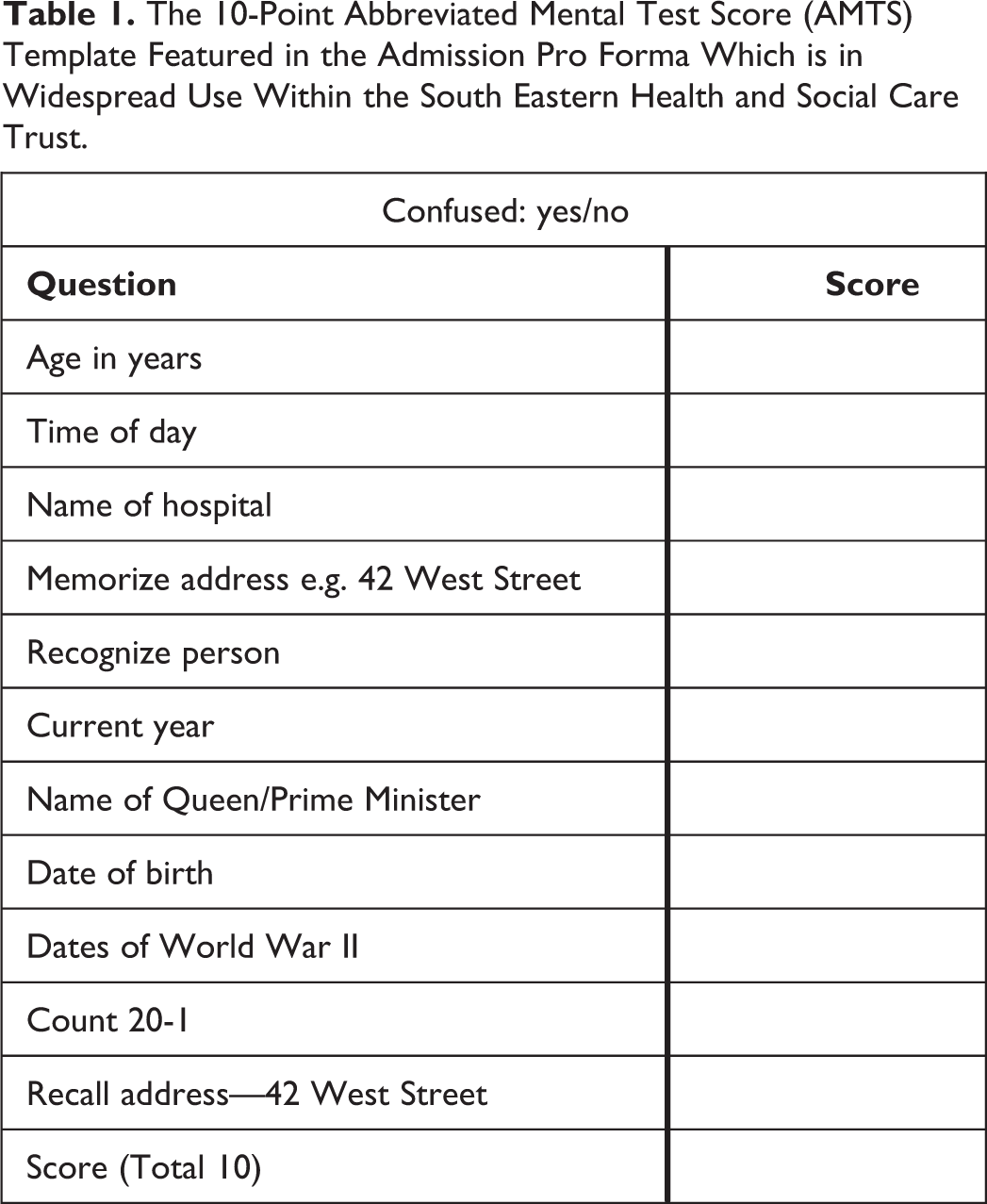
Research has shown that while many orthopedic junior doctors are aware of the importance of the use of the AMTS, only a small proportion (approximately 10%) can identify all 10 questions involved. 16 In light of this, and in keeping with BOAST guidelines, an AMTS template (Table 1) has been incorporated into the admission proformas used within Northern Ireland’s South Eastern Health and Social Care Trust Trauma & Orthopaedic Unit to serve as an aide memoire. There is also an option to select whether or not the patient appears confused. In cases where the AMTS is not recorded upon admission, this is usually completed during orthogeriatrician review, which may occur several days following admission and possibly after surgery has been completed.
The 10-Point Abbreviated Mental Test Score (AMTS) Template Featured in the Admission Pro Forma Which is in Widespread Use Within the South Eastern Health and Social Care Trust.
Consideration of cognitive impairment upon admission is of particular relevance in Northern Ireland. Formal diagnoses of both mild cognitive impairment and dementia are routinely made by psychogeriatricians in the community setting. Such psychiatric outpatient clinic letters are not currently accessible on the Northern Ireland Electronic Care Record (NIECR), 17 which is used in the acute hospital setting. Therefore, information available to doctors in the acute setting may be inaccurate or incomplete. Furthermore, recent changes in Northern Ireland legislation, namely the Deprivation of Liberty Safeguards implemented in December 2019, mean that depriving a patient who lacks capacity of their liberty could be an infringement of their human rights. Keeping a patient in hospital for fracture management where they are not free to leave could be considered a deprivation of liberty. Thus, it is important to determine whether or not a patient has capacity to accept or decline treatment and act in accordance with legislation as necessary.
The aim of this project was to review current practice within the unit regarding documentation of AMTS upon admission among elderly orthopedic trauma patients including hip fracture patients. As an intervention, BOAST guidelines and initial findings were then distributed among junior doctors (foundation year doctors/core surgical trainees) responsible for clerking-in acute fracture patients. The audit loop was then closed to determine the effectiveness of the intervention.
This work was conducted in a district general hospital with emergency trauma and orthopedic services. Current practice within the unit is that after a patient has been accepted for orthopedic admission, they would be clerked-in by a junior member of the surgical team and then subsequently reviewed in-hours by a senior member of the orthogeriatric team. The patient would typically be consented for surgery by a more senior member of the orthopedic team during the post-take ward round. As per Northern Ireland’s regional policy, patients deemed to have capacity to consent for surgery sign “Form I” preoperatively. Alternatively, if a patient were deemed not to have capacity but the procedure was believed to be in the patient’s best interests, the surgeon signs “Form IV,” ideally after consultation with the next of kin and considering any previously expressed wishes. Wherever possible, efforts to treat reversible causes of acute confusion, for example, infection and electrolyte disturbances, are made prior to surgery.
We hypothesized that older patients and those with known cognitive or mental health disorders would be more likely to be screened for cognitive impairment upon admission. We also hypothesized that core trainees would be more aware of the importance of screening for cognitive impairment than foundation year doctors and thus more likely to document the AMTS.
Methods
Data were obtained by means of inpatient chart review and access to the NIECR. Information regarding AMTS upon admission and upon subsequent orthogeriatrician review was recorded, in addition to the nature of consent form used (if applicable) and any history of cognitive impairment/mental health disorders.
Preintervention data were collected throughout November and December 2018. Patients were included if they were admitted to the unit under the care of the Trauma & Orthopaedic team with an acute orthopedic injury and aged >65 years or if they sustained a fragility hip fracture at any age.
The findings from the first cycle of data collection and a copy of BOAST guidelines were distributed in electronic format to all junior doctors in the unit responsible for completing the required admission paperwork. Postintervention data were then collected in a similar manner throughout January and February 2019.
Statistical analysis was performed using Stata 15.0 (StataCorp 2017, Stata Statistical Software: Release 15; StataCorp LLC). Comparisons were undertaken using χ2 tests for comparison of categorical variables and t tests for continuous variables. For pre- and posttest comparisons of the AMTS, a McNemar χ2 test was utilized. Multiple logistic regression analyses were used to determine the factors influencing AMTS recording. A P value of less than .05 was considered statistically significant.
Results
Patient Demographics
In total, 79 patients were included in the analysis: 40 in the preintervention arm and 39 in the postintervention arm. Preintervention, 40 suitable patients (25 females and 15 males), mean age 81.7 years (range: 65-96), were identified. Of these patients, 25 (62.5%) sustained a hip fracture, mean age 82.1 years (range: 66-94). Other injuries were fractures of the distal femur (n = 3), tibia (n = 3), ankle (n = 2), acetabulum (n = 1), humerus (n = 1), cervical spine (n = 1), and periprosthetic femoral fracture (n = 2), as well as prosthetic hip dislocation (n = 1) and quadriceps tendon rupture (n = 1).
Postintervention, 39 suitable patients (24 females and 15 males), mean age 80.4 years (range: 42-95), were identified. Thirty of these patients (76.9%) sustained a hip fracture, mean age 82.7 years (range: 42-95). Other reasons for admission were fractures of the femoral shaft (n = 4), distal femur (n = 3), and acetabulum (n = 2).
Regarding grade of admitting doctor, 22 patients (55.0%) in the preintervention group and 26 (66.7%) in the postintervention group were admitted by a foundation year doctor. Eighteen patients (45%) in the preintervention group and 12 (30.8%) in the postintervention group were admitted by a core trainee. For 1 patient in the postintervention arm, the grade of admitting doctor was unspecified.
Recording of AMTS
Figure 1 demonstrates the recording of the AMTS for both the overall cohort and the hip fracture subgroup, pre- and postintervention.

The recording of the Abbreviated Mental Test Score (AMTS) for both the overall cohort (A) and the hip fracture subgroup (B) both pre- and postintervention is demonstrated. Note a small but significant increase in the recording of the AMTS has been achieved postintervention for both the cohort overall and the hip fracture subgroup. Red: AMTS not recorded; blue: AMTS recorded.
Preintervention, only 9 (22.5%) of the 40 patients in the overall cohort and 7 (28.0%) of the 25 patients in the hip fracture subgroup had their AMTS recorded by the admitting doctor (Table 2). Table 2 also shows whether these patients were recorded as being confused or not upon admission. In the multiple regression model, there was no significant association between whether the AMTS was recorded upon admission and patient age (P = .566), sex (P = .412), type of injury (P = .206), confusional status (P = .118), or grade of admitting doctor (P = .058).
Documentation of the Abbreviated Mental Test Score (AMTS) and Confusional Status Upon Admission Among the Pre- and Postintervention Cohorts.

Abbreviations: AMTS, Abbreviated Mental Test Score.
Postintervention, 15 (38.5%) of the 39 patients in the overall cohort and 11 (36.7%) of the 30 patients in the hip fracture subgroup had their AMTS recorded by the admitting doctor (Table 2). In the multiple regression model, there was no significant association between whether the AMTS was recorded upon admission and patient age (P = .214), sex (P = .120), type of injury (P = .453), confusional status (P = .473), or grade of admitting doctor (P = .494). Statistical analysis demonstrated a significant improvement in AMTS documentation both among the overall cohort (P = .001) and the hip fracture patients (P = .019).
Nature of Consent Form
Thirty-seven patients underwent operative management in both the pre- and postintervention cohorts. All hip fracture patients underwent operative intervention (preintervention n = 25, postintervention n = 30). Table 3 outlines the nature of consent form used among the overall cohort and for the hip fracture subgroup pre- and postintervention.
Nature of Consent Form Used for Patients Undergoing Operative Intervention.a

Abbreviations: AMTS, Abbreviated Mental Test Score.
a Form I is used among patients believed to have capacity to make decisions regarding their treatment. Form IV is used among patients felt to lack capacity and therefore the clinician is acting in the patient’s best interests.
Table 3 also demonstrates the number of patients in each of the groups who had an AMTS recorded upon admission or upon subsequent orthogeriatrician review (median time to orthogeriatrician review was 1 day following admission for both the pre- and postintervention arms). The mean AMTS for each type of consent form for the overall cohort and hip fracture subgroup, pre- and postintervention, is shown. The mean AMTS was calculated in cases where there was an AMTS score available, either from the admitting doctor’s assessment or from the orthogeriatrician’s assessment if not completed by the admitting doctor.
Prior Cognitive/Mental Health Disorder
As outlined in Table 4, 15 (37.5%) of the 40 patients in the preintervention cohort and 17 (43.6%) of the 39 patients in the postintervention cohort had evidence of prior cognitive or mental health disorder.
The Incidence of Known Prior Significant Cognitive or Mental Health Disorder Among the Pre- and Postintervention Cohort.

Overall, those with prior cognitive or mental health disorders were not significantly more likely to have their AMTS recorded upon admission (P = .256) but were however less likely to be consented for surgery using Form I (P = .001). Older patients were also less likely to be consented using Form I than younger patients (P = .03). The mean age of those being consented using Form I was 79.6 years (standard deviation: 10.32 years), whereas the mean age of those consented using Form IV was 85.3 years (standard deviation: 5.75 years).
Discussion
The aim of this project was to improve AMTS documentation upon admission among frail fracture patients. Following a simple brief intervention, a statistically significant improvement in AMTS documentation was demonstrated for both the overall elderly fracture patient cohort and the hip fracture subgroup.
The neuropathological hallmarks for Alzheimer’s disease are β-amyloid senile plaques and τ-neurofibrillary tangles which accumulate in the parietal and neocortical regions of the brain. Mild cognitive impairment is regarded as a transitional stage between normal aging and Alzheimer disease and has been associated with neurofibrillary tangles in the hippocampus and other medial temporal regions. Introduced into the literature in 1988 by Reisberg and colleagues, Small et al highlighted that mild cognitive impairment is characterized by a cognitive decline without impairment in the ability to carry out activities of daily living. 18 Interestingly, a large proportion of older hip fracture patients without prediagnosed dementia have been found to have evidence of Alzheimer disease pathology on analysis of cerebrospinal fluid biomarkers. This may in fact suggest there is a possibility of preclinical dementia among certain hip fracture patients. 19
The significance of cognitive impairment, resulting from preexisting dementia or acute delirium, is well established among hip fracture patients. A patient’s capacity to make decisions regarding their management and functional rehabilitation may be hindered. Delirium has been associated with increasing age, female sex, underlying dementia, poorer general physical health, chest or urinary infections, and increased length of hospital stay. 4,5 Inadequate analgesia has also been shown to negatively affect a patient’s AMTS, and regional analgesia has been found to reduce the risk of AMTS deterioration perioperatively. 15 Following hip fracture, patients with impaired cognition are less likely to return to their own homes or have successful rehabilitation. 1 Furthermore, hip fracture patients with delirium have been found to experience increased length of hospital stay and increased 1-year mortality, 5 and delirium superimposed on dementia is a strong predictor of functional dependence, institutionalization, and mortality. 20
Hip fracture surgery has been associated with a higher incidence of delirium than elective orthopedic surgery. 21 However, the literature is lacking regarding the role of cognitive impairment in the recovery and rehabilitation regarding other orthopedic injuries, as studied in this cohort. We suggest that cognitive impairment may be of particular relevance among those with injuries affecting weight-bearing status (eg, ankle fractures) or use of mobility aids (eg, distal radial fractures).
Challenges can also arise when managing patients with delirium on an acute trauma ward, and antipsychotics are often prescribed in elderly patients. However, current evidence does not support the use of antipsychotics for the prevention of delirium, and antipsychotics have not been shown to improve delirium duration or severity. 22 From our current results, it is unclear if the AMTS specifically helps with the management of delirium in the acute orthopedic patient. However, a low AMTS upon admission may highlight that a patient has a degree of cognitive impairment and is thus more likely to experience perioperative delirium.
Interestingly, we found that older fracture patients were not significantly more likely to be screened for cognitive impairment upon admission than younger patients. We suggest that if an elderly patient has an established dementia diagnosis, the admitting doctor may not see it necessary to record the AMTS. It should also be remembered that the AMTS value achieved upon admission cannot be assumed to represent the patient’s best cognitive function, as their cognition may be affected for various reasons, including pain, unfamiliar environment, and time of day.
To our knowledge, this is the first reported study of associations between the AMTS and type of consent form used in Northern Ireland. Although the numbers were too small to make meaningful statistical comparisons, the mean AMTS for both the pre- and postintervention arms were greater than 8/10 among those consented using Form I and below 4/10 among those consented using Form IV (Table 3). While it is important to remember that level of cognition and capacity are difficult to define numerically, and capacity is regarded as time- and question-specific, we suggest that further work is warranted to investigate whether a cutoff score exists at which the clinician can have reasonable confidence in saying that a patient likely lacks capacity.
None of the patients had an AMTS recalculated between the time of initial AMTS recording and their surgery in cases where there was a delay of a few days in getting to theater. This may be significant as patients previously deemed to lack capacity may have improved with the correction of reversible factors; similarly, patients deemed to have capacity upon admission may have developed delirium. None of the patients had their AMTS recalculated postoperatively or prior to discharge. Therefore, we were not able to objectively determine whether undergoing surgery was associated with a deterioration in the AMTS.
Disappointingly, only a small improvement in the number of patients having their AMTS recorded upon admission was seen following education and distribution of BOAST guidelines. We suggest that barriers to compliance with BOAST guidelines include competing demands from more clinically urgent tasks (particularly during out-of-hours work), the assumption that the AMTS will be subsequently recorded by the orthogeriatric team, and possible lack of awareness due to rotational/shift-based work seen among junior doctors.
Future work should explore the effectiveness, or otherwise, of highlighting the clinical relevance of BOAST guidelines during both the unit induction sessions with each rotation of junior doctors and weekly junior doctor teaching sessions. A focus group to explore trainee understanding of the importance of screening for cognitive impairment may also help to identify further barriers to compliance and means by which these may be overcome.
It can also be suggested that while the AMTS score upon admission with a fracture may not be entirely representative of baseline cognitive function, it plays an important role in encouraging the trauma team to screen for dementia and/or delirium and perhaps refer onward where appropriate, as well as identifying patients who may be at heightened risk of perioperative delirium. The AMTS may also serve as part of a preoperative risk assessment tool for cognitive impairment in the fracture clinic setting among patients with other orthopedic injuries for whom the decision is made to operate at outpatient review.
We are mindful that this project was commenced prior to the update on the British Orthopaedic Association guidelines suggesting the use of a validated delirium assessment tool. 7 These guidelines have more recently suggested the use of the 4AT, which has been shown to be both a sensitive and specific method of screening for delirium in hospitalized older people. 23 However, in the United Kingdom, and in our trauma unit, the AMTS has historically been used. We suggest that an area for further work would be to compare AMTS and 4AT scores upon admission and postoperatively.
Conclusion
In conclusion, a small but significant improvement in compliance with BOAST guidelines was seen following distribution of BOAST guidelines in written format. Further work should explore means by which compliance with these guidelines can be improved and also the effect of cognitive impairment on outcomes related to injuries beyond hip fractures.
Footnotes
Authors’ Note
Approval obtained from the South Eastern Health and Social Care Trust audit department.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.