
Abstract
Introduction:
Physiological and Operative Severity Score for the enUmeration of Mortality and Morbidity (POSSUM) and Portsmouth POSSUM (P-POSSUM) are general surgical tools used to efficiently assess mortality and morbidity risk. Data suggest that these tools can be used in hip fracture patients to predict morbidity and mortality; however, it is unclear what score indicates a significant risk on a case-by-case basis. We examined the POSSUM and P-POSSUM scores in a group of hip fracture mortalities in order to assess their accuracy in identification of similar high-risk patients.
Materials and Methods:
Retrospective analysis of all consecutive mortalities in hip fracture patients at a single tertiary care center over 2 years was performed. Patient medical records were examined for baseline demographics, fracture characteristics, surgical interventions, and cause of death. Twelve physiological and 6 operative variables were used to retrospectively calculate POSSUM and P-POSSUM scores at the time of injury.
Results:
Forty-seven hip fracture mortalities were reviewed. Median patient age was 88 years (range: 56-99). Overall, 68.1% (32) underwent surgical intervention. Mean predicted POSSUM morbidity and mortality rates were 73.9% (28%-99%) and 31.1% (5%-83%), respectively. The mean predicted P-POSSUM mortality rate was 26.4% (1%-91%) and 53.2% (25) had a P-POSSUM predicted mortality of >20%. Subgroup analysis demonstrated poor agreement between predicted mortality and observed mortality rate for POSSUM in operative (χ2 = 127.5, P < .00001) and nonoperative cohorts (χ2 = 14.6, P < .00001), in addition to P-POSSUM operative (χ2 = 101.9, P < .00001) and nonoperative (χ2 = 11.9, P < .00001) scoring.
Discussion/Conclusion:
Hip fracture patients are at significant risk of both morbidity and mortality. A reliable, replicable, and accurate tool to represent the expected risk of such complications could help facilitate clinical decision-making to determine the optimal level of care. Screening tools such as POSSUM and P-POSSUM have limitations in accurately identifying high-risk hip fracture patients.
Introduction
In the United States, more than 2 million osteoporotic fractures occur annually, which costs more than 17 billion US dollars. Of those, 14% were hip fractures, which accounted for 72% of the total cost. 1,2 Similar trends and burden from hip fracture management are observed around the world, especially in developed nations. 3 Despite tremendous advances in geriatric fracture care with the advent of geriatric fracture centers and comanagement, 4 -7 osteoporotic hip fractures are associated with high rates of morbidity and mortality to affected patients. 8 -11 Reports of 1-year mortality rates are as high as 84.4% 8 for patients treated nonoperatively and 38% in operative patients. 9 Patients with multiple medical comorbidities are at an even higher risk of serious complications, morbidity, and death. 12 -14
As health care shifts from service-based to value-based care, accurate identification of the patients at highest risk for adverse outcomes is important. 15,16 Over the past several decades, there have been multiple scoring tools developed and utilized to stratify patient risk. 17 Some of the most commonly used tools are the American Society of Anesthesiologists score, 18 Charlson Comorbidity Index, 19 Elixhauser Comorbidity Index, 20 and Nottingham Hip Fracture Score. 21 The Physiological and Operative Severity Score for the enUmeration of Mortality and Morbidity (POSSUM) score was originally described by Copeland et al in general surgery patients in 1991 as an attempt to provide a simple, objective audit tool to assess morbidity and mortality risks. 22 -26 It consists of a 12-factor, 4-grade physiological score and a 6-factor, 4-grade operative severity score that was established with multivariate discriminant analysis techniques and includes parameters that are routinely collected throughout a patient’s hospital stay. 22 In 2002, the POSSUM score was adapted and validated for Orthopaedic surgery. 27 Since then, it has been independently studied for hip fracture patients, 9,28 including one prospective study by Wright et al in which the predictive value of the POSSUM score was assessed. 29 One potential concern of the POSSUM score, however, is that it has been shown to overpredict the risk of mortality and may require further calibration. 23,26,28 To address this, the POSSUM scale was adjusted from exponential scoring to linear scoring during the development of the Portsmouth POSSUM (P-POSSUM) score. 23
Despite being able to prospectively stratify patients at risk for mortality with variable accuracy, there is sparse literature focused specifically on mortality cases and whether or not these mortalities were expected. It is our hypothesis that POSSUM and P-POSSUM would accurately predict the degree of morbidity and mortality in a cohort of hip fracture mortalities. The primary aim of the study is to assess POSSUM and P-POSSUM scores as risk stratification tools to guide management and resource allocation of individual hip fracture patients. The secondary aim is to determine the strengths and limitations of these predictive tools.
Materials and Methods
After institutional review board approval was obtained, a retrospective review was performed on a consecutive cohort of all hip fracture (intracapsular and extracapsular) mortalities at a tertiary care referral hospital in the UK over a 2-year period. The patients were identified from mortality records, reflecting data used to complete death certificates. Exclusion criteria included survival following hip fracture and incomplete medical records.
Patients were admitted to the Orthopaedic service following presentation to the emergency department and hip fracture diagnosis made. Patients were managed according to the British Orthopaedic Association—British Geriatric Society “Blue Book” guidelines, 30 with early admission and comanaged care between surgeons and geriatricians. Details of the operative intervention were dependent on the fracture pattern and surgeon preference. Surgery was performed within 36 hours whenever possible. Postoperatively, there was a continuation of comanaged care using a multidisciplinary team approach according to national guidelines. 30 Palliative care with nonoperative fracture management was initiated if patients were deemed too high risk for surgery following a review from both a geriatrician and an anesthesiologist due to the presence of one or more of the following: acute respiratory failure, renal failure, congestive heart failure, active pneumonia, and/or cancer.
Patient medical records were examined for baseline demographics, fracture type, management, and cause of death. Although there were often comorbidities and diagnoses contributing to a patient’s death, the single cause of death assigned on the patient’s death certificate was used for the purposes of analysis in the study. Twelve physiological and 6 operative variables were identified and scored as depicted in Online Appendix 1 (adapted from Mohamed et al).
27
The POSSUM morbidity and mortality risk were then calculated using the equations as published by Copeland et al
22
: Morbidity Risk = ln[R/(1−R)] = −5.91 + (0.16 × physiological score) + (0.19 × operative severity score), where R is the predicted risk of morbidity. Mortality Risk = ln[R/(1−R)] = −7.04 + (0.13 × physiological score) + (0.16 × operative severity score), where R is the predicted risk of mortality.
Subsequently, the P-POSSUM mortality risk was calculated using the equation: ln[R/(1−R)] = −9.065 + (0.1692 × physiological score) + (0.1550 × operative severity score), where R is the predicted risk of mortality as described by Prytherch, Hosmer, and Lemeshow. 23,31 -33
Statistical analysis was completed using Microsoft Excel (Excel Version, 2018) for Windows. The predicted morbidity and mortality rates were then interpreted to provide measures of clinical significance. Predicted number of deaths (number of patients × mean risk) was compared with the reported number of deaths occurring within 20° ranges of predicted mortality rate and input into frequency tables to facilitate comparison by means of the χ2 test as described by Prytherch et al. 23 . Yates correction was utilized for χ2 analysis due to small sample size. 34 Given the increased mortality in geriatric hip fracture cases managed nonoperatively, 8 hip fracture cohorts managed operatively and nonoperatively were separated and analyzed via χ2 analysis. Data are described as mean values with standard deviation, unless otherwise specified. Significant results were assumed if P < .05.
Results
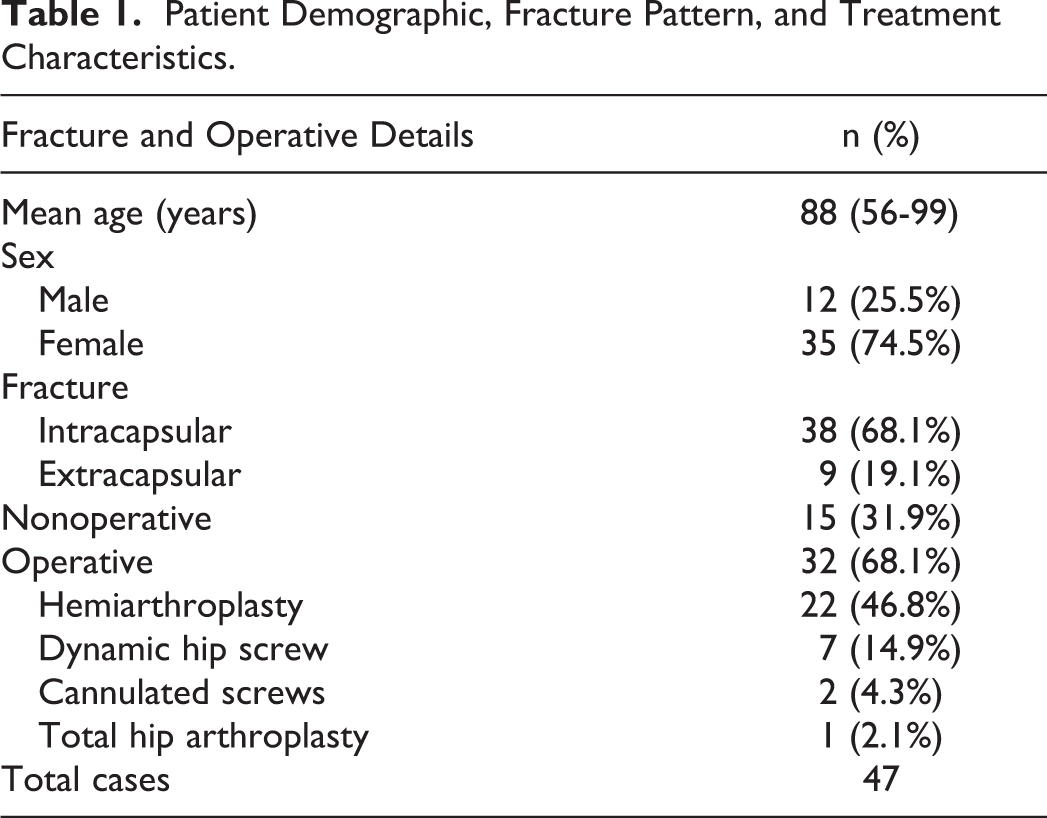
Over a period of 24 months, 47 hip fracture mortalities were identified. Surgery was performed on 32 (68.1%) patients and 15 (31.9%) were treated nonoperatively. Details on baseline demographics, fracture characteristics, and type of surgical procedure are shown in Table 1. Data on mean surgical delay and cause of death are demonstrated in Table 2. The mean time to death, from admission for nonoperative cases, and, from surgery for operative cases, was 20 days (range, 1-65 days).
Patient Demographic, Fracture Pattern, and Treatment Characteristics.
Summary of Delay to Surgery, Time to Death, and Cause of Death.

a The single cause of death assigned on the patient’s death certificate was utilized to indicate cause of death despite other contributing medical comorbidities.
The mean overall POSSUM physiological score was 32.2 (18-35) and the mean POSSUM operative score was 11.6 (9-18). Based on the mean POSSUM scores, the predicted mortality for all patients was 31.1% (5%-83%; Tables 3 and 4, Figure 1). Of the entire cohort, 94% had a predicted mortality less than 50%, and 50% had a predicted mortality less than 20%. When nonoperative cases were excluded, the predicted POSSUM mortality for those treated operatively was 24.9% ±18.3% with mean physiological score of 30.3 ± 8.3 and mean operative score of 11.1 ± 0.6. Chi-square analysis of the operative cohort demonstrated poor agreement between predicted mortality and observed mortality rate (χ2 = 127.5, 4 degrees of freedom, P < .00001; Table 4, Figure 1). In the nonoperative cohort, the average POSSUM mortality was 41.1% ±14.7% with mean physiological score of 36.3 ± 8.2 and mean operative score of 12.5 ± 2.9. Chi-square analysis of the nonoperative cohort demonstrated poor agreement between predicted mortality and observed mortality rate (χ2 = 14.6, 4 degrees of freedom, P < .00001; Table 6, Figure 1).
Summary of POSSUM and P-POSSUM Scoring.

Abbreviation: POSSUM, Physiological and Operative Severity Score for the enUmeration of Mortality and Morbidity; P-POSSUM, Portsmouth POSSUM.
Patients Treated Operatively Grouped by Calculated Risk of Mortality for POSSUM.a

Abbreviation: POSSUM, Physiological and Operative Severity Score for the enUmeration of Mortality and Morbidity.
a Grouped by 20% risk increments. Predicted deaths = number of patients per cohort × mean risk. Statistical methods by means of χ2 analysis.
Patients grouped by calculated risk of mortality for Physiological and Operative Severity Score for the enUmeration of Mortality and Morbidity (POSSUM) and Portsmouth POSSUM (P-POSSUM). Grouped by 20% risk increments.
Patients Treated Operatively Grouped by Calculated Risk of Mortality for P-POSSUM.a

Abbreviation: P-POSSUM, Portsmouth POSSUM.
a Grouped by 20% risk increments. Predicted deaths = number of patients per cohort × mean risk. Statistical methods by means of χ2 analysis.
Patients Treated Nonoperatively Grouped by Calculated Risk of Mortality for POSSUM.a
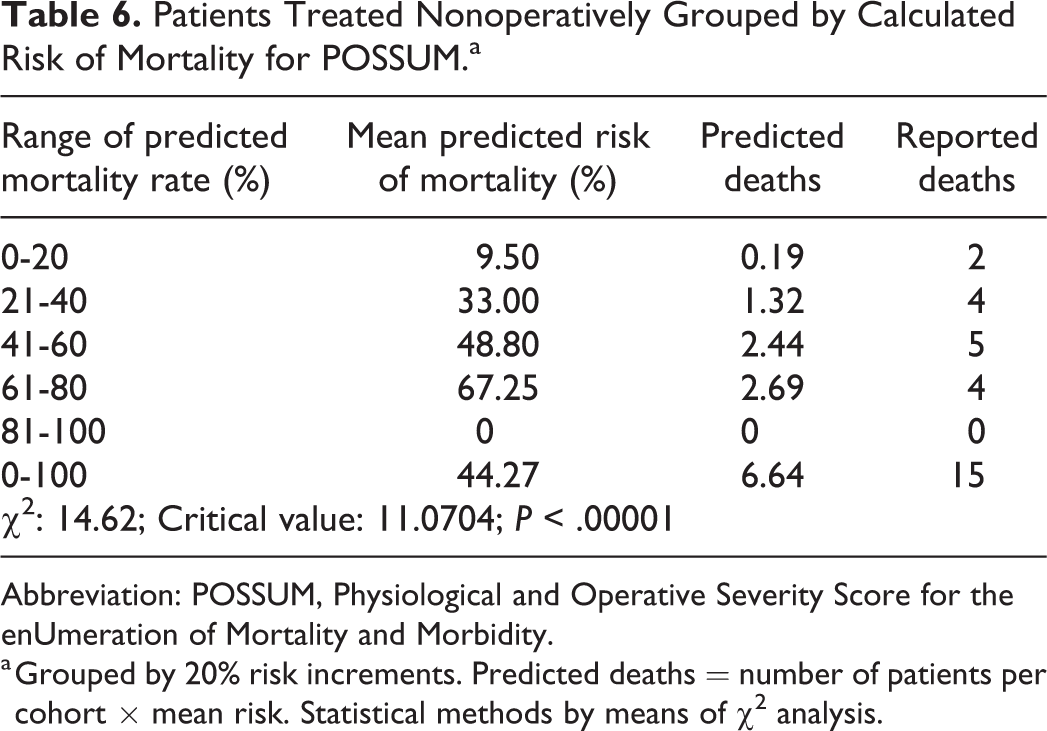
Abbreviation: POSSUM, Physiological and Operative Severity Score for the enUmeration of Mortality and Morbidity.
a Grouped by 20% risk increments. Predicted deaths = number of patients per cohort × mean risk. Statistical methods by means of χ2 analysis.
Using the P-POSSUM calculation adjustment, the predicted mortality for all patients was 26.4% (1%-91%; Table 3). Of the entire population, 94% had a predicted mortality rate less than 50%, and 59% had a predicted mortality rate less than 20% (Tables 3 and 6, Figure 1). Even more strikingly, by P-POSSUM scoring, 50% of the mortalities were in patients estimated to be very low risk (ie, 0%-10% risk; Table 8 and Figure 2). When nonoperative cases were excluded, the mean P-POSSUM mortality was 19.5% ±21.4%. For the operative cohort, χ2 analysis demonstrated poor agreement between predicted mortality and observed mortality rate (χ2 = 101.9, 4 degrees of freedom, P < .00001; Table 5, Figure 1). In the nonoperative cohort, the average P-POSSUM mortality was 41.1% ±24.7% with χ2 analysis demonstrated poor agreement between predicted mortality and observed mortality rate (χ2 = 11.9, 4 degrees of freedom, P < .00001; Table 7, Figure 1).

Patients grouped by calculated risk of mortality for Physiological and Operative Severity Score for the enUmeration of Mortality and Morbidity (POSSUM) and Portsmouth POSSUM (P-POSSUM). Grouped by 10% risk increments.
Patients Treated Nonoperatively Grouped by Calculated Risk of Mortality for P-POSSUM.a
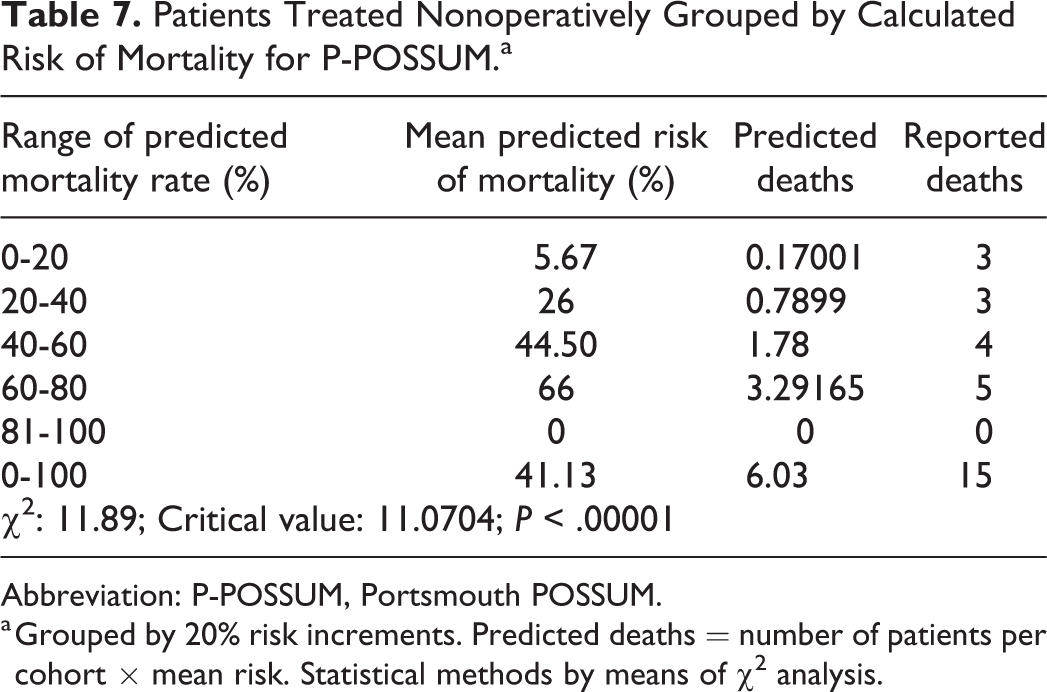
Abbreviation: P-POSSUM, Portsmouth POSSUM.
a Grouped by 20% risk increments. Predicted deaths = number of patients per cohort × mean risk. Statistical methods by means of χ2 analysis.
Patients Grouped by Calculated Risk of Mortality for POSSUM and P-POSSUM.a

Abbreviation: POSSUM, Physiological and Operative Severity Score for the enUmeration of Mortality and Morbidity; P-POSSUM, Portsmouth POSSUM.
a Grouped by 10% risk increments. Numbers shown as percentage of cohort.
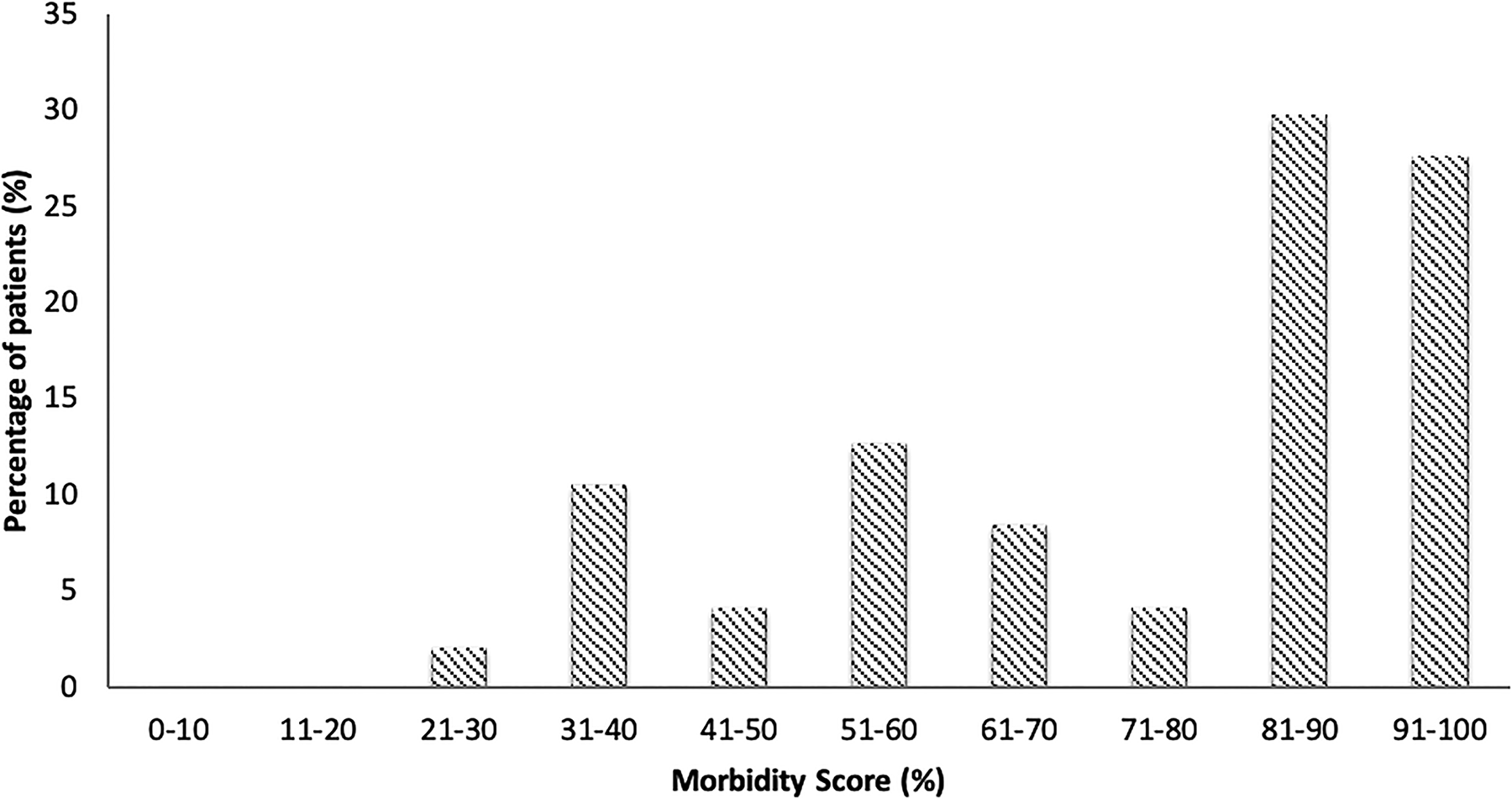
Based on the POSSUM scale, the predicted morbidity rate was 73.9% (28%-99%; Table 3, Figure 3). Eighty-three percent of patients had predicted morbidity >50% and 62% (29/47) patients had morbidity score of >75. One (2%) patient had a predicted morbidity score <30% (Figure 3).

Physiological and Operative Severity Score for the enUmeration of Mortality and Morbidity (POSSUM) morbidity score distribution for patient cohort.
Discussion
The morbidity, mortality, and financial burden 1,35 associated with hip fracture management poses significant challenges to Orthopaedic surgeons. Providers must be equipped with the tools necessary to identify the highest risk patients and be able to make evidence-based management decisions on candidacy for operative interventions versus palliative measures. To our knowledge, this study is the first of its kind and found that the POSSUM scoring system underpredicted the observed mortality rate in hip fracture cohorts managed both operatively and nonoperatively. Physiological and Operative Severity Score for the enUmeration of Mortality and Morbidity scoring shows promise in its ability to effectively predict high morbidity levels and was substantially more accurate in estimating mortality when applied to nonoperative patients. However, this study highlights the potential limitations of POSSUM and P-POSSUM scoring systems for prospective risk stratification of mortality in hip fracture patients, especially for those patients undergoing operative management. Despite the value of POSSUM and P-POSSUM scoring for assessing a large and diverse cohort of patients, it should be used with caution on a case-by-case basis in the management of hip fractures due to underestimation of mortality risk.
Prior studies have evaluated the predictive value of the POSSUM and P-POSSUM scales for mortality in general surgery 22,23,29 and hip fracture cohorts. 9,27 -29 However, no prior studies have retrospectively evaluated isolated cases of mortality to determine the accuracy of POSSUM and P-POSSUM scales in predicting mortality on a case-by-case basis. The findings of the present study, in which over 50% of hip fracture mortalities were classified as minor risk (<10%) by the P-POSSUM score, are in contrary to the existing literature on POSSUM and P-POSSUM scoring as audit and risk-assessment tools. In a study of 1000 general surgery patients, Prytherch et al found the POSSUM score overpredicted mortality. This was especially true in low-risk patients in whom the mortality was predicted 7× greater than the observed mortality. In the same study, the predicted accuracy of P-POSSUM much more closely matched that of the observed. 23 An audit by Ramanathan et al reiterated these findings that the postoperative application of the POSSUM scale to a cohort of hip fracture patients had a tendency to overpredict mortality by approximately 5% (15% predicted vs 10% observed). 28 Similarly, Young et al demonstrated that POSSUM overpredicted mortality when applied to 225 patients undergoing surgical management for femoral neck fractures at a single institution. 9 Furthermore, Wright et al demonstrated that prospective POSSUM and P-POSSUM scoring accurately predicted mortality in a cohort of patients undergoing surgical management of femoral neck fractures with observed: expected (O: E) mortality ratios of 1.9 and 0.95, respectively. 29 They concluded that orthopedic POSSUM accurately predicts mortality in patients with femoral neck fractures. 29 However, through the application of these scoring systems to a cohort of hip fracture mortalities, the present study highlights that these risk assessment tools cannot be relied upon on the individual level in order to predict mortality risk. The underprediction of mortality in the present study is likely attributable to the application of the POSSUM scoring system in an individualized manner, for which the tool was not initially designed. This study serves as an important reminder that prediction and screening tools, while effective when used in appropriate circumstances, must be implemented and applied cautiously.
However, POSSUM scoring system was effective in predicting morbidity. Consistent with the criterion of Mohamed et al, morbidity was characterized by the presence of infection (pulmonary, urinary, surgical site, septicemia, fever), deep or superficial hemorrhage, wound complications such as seroma, thromboembolic events, or cardiac, respiratory, or renal complications throughout the follow-up period. 27 In the present study, only 2% of patients (1/47) had a predicted morbidity rate of <30%, and 83% (39/47) of patients had a predicted morbidity rate of >50%. The ability of POSSUM scoring to accurately predict morbidity is consistent with previously, controlled studies in orthopaedic, 36,37 general surgery, 38 and critical care patients. 39 Despite the limitations of accurate mortality prediction in the present study, the accurate prediction of morbidity by POSSUM scoring affords some utility in facilitating discussion with patient and family, deciding nonoperative versus operative treatment, identifying patients who need an advanced work up, and planning for the appropriate level of perioperative care. Furthermore, the POSSUM scoring system serves as a simple, effective indicator of patient morbidity risk that can be used and easily understood in communication with other medical specialties in order to efficiently guide clinical management.
Despite prior studies accurately predicting mortality in hip fracture rate in a large cohort of patients, 22,23,27 -29 this study highlights the limitations of the use of POSSUM and other risk assessment tools designed for a diverse cohort of patients on an individual basis. To our knowledge, this was the first study to examine the use of Physiological and Operative Severity Score for the enUmeration of Mortality and Morbidity (POSSUM) and P-POSSUM scoring in cohorts of hip fracture patients managed both operatively and nonoperatively. In the present study, the 68% operative fixation rate is lower than the estimated operative rate of 80% in similar high-risk fracture patients by other studies. 40 However, this difference is likely explained by the relatively large number of patients in this cohort being deemed poor surgical candidates due to their suboptimal medical conditions and multiple comorbidities. As a result, subgroup analysis was performed in order to identify potential differences between operative and nonoperative cohorts. Although analysis demonstrated greater accuracy of mortality prediction in the nonoperative compared to operative patients, there remained poor agreement between expected and observed mortality outcomes when the scoring systems were applied to either cohort. Clinicians should be aware of the potential limitations of predictive tools, understand the possibility for misrepresentation of a patient’s true clinical condition, and instead use them as an adjunct to comprehensive care. Expectations for treatment should be cautious and realistic, irrespective of the score and perceived risk to patients with hip fractures.
This study had several limitations. First, the POSSUM and P-POSSUM scores were originally intended for use in general surgical patients. The use of POSSUM has been adapted to orthopedic patients as the O-POSSUM; however, the use of the POSSUM in lieu of the O-POSSUM has minimal effect on the final scoring as the adaptation is limited to minor restructuring of the operative score for greater surgical relevance. Second, POSSUM and P-POSSUM scoring estimate 30-day mortality, whereas our study included all mortalities within a 2-year period regardless of time from presentation. The inclusion of mortalities greater than 30 days from presentation may have falsely elevated the predicted morbidity and mortality of the cohort. However, the mean time to death of the sample was 20 days and was within the intended timeframe for the POSSUM and P-POSSUM scores. Third, the concept of “morbidity” is difficult to define and even more difficult to quantify in scoring systems such as POSSUM and P-POSSUM. Such scoring systems do not address conditions such as delirium or change in function. However, these conditions are often preceded by acute and objectively measurable conditions such as infection, renal failure, and cardiopulmonary disease, which POSSUM scoring accounts for. Finally, due to the retrospective design and absence of a control group, the results of this study should be interpreted with caution when assessing the scoring systems and may be susceptible to selection and informational bias.
Conclusion
The use of POSSUM and P-POSSUM scores for hip fracture patients underpredicted the risk of most mortalities. Despite prior studies demonstrating accurate mortality prediction by POSSUM and P-POSSUM scoring systems, these events were significantly underpredicted in mortality cases in the present study when applied to individual patients. Although these tools are accessible, quick, and simple-to-use, health care professionals should be cautious when applying these tools to make management decisions on individual hip fracture patients. Nevertheless, the accurate prediction of patient morbidity by POSSUM scoring demonstrates its potential utility as an adjunct to assessing risk, guiding discussion with the patient and family members, and facilitating management decisions such as operative candidacy and level of care allocation. Importantly, in an effort to balance a patient’s true clinical condition with that being predicted, clinicians should approach all hip fracture patients with great diligence regardless of their perceived risk. The present study’s findings highlight the need for an accurate predictive scoring tool for hip fracture patients.
Supplemental Material
Supplemental Material, Appendix1Tiff - POSSUM and P-POSSUM Scoring in Hip Fracture Mortalities
Supplemental Material, Appendix1Tiff for POSSUM and P-POSSUM Scoring in Hip Fracture Mortalities by William L. Johns, Benjamin Strong, Stephen Kates and Nirav K. Patel in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Stephen Kates is the editor of Geriatric Orthopaedic Surgery & Rehabilitation.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.