
Abstract
Introduction:
Despite hip fractures being a great public health burden, only few studies have analyzed the relationship between hip fracture incidence and socioeconomic status. Many studies found an association; however, results are in part conflicting.
Objective:
To analyze the impact of regional-level socioeconomic status on the incidence of hip fractures in the Maltese Islands.
Method:
All individuals older than 50 years who presented to the acute care hospitals in Malta and Gozo with low-energy hip fractures between December 1, 2015, and November 30, 2016, were selected. Data on individual demographics, hip fracture type, surgical intervention, and hospital stay were collected. The percentage of hip fracture and socioeconomic status of each region in the Maltese Islands were calculated. These were then analyzed for any statistical association.
Results:
A moderate negative correlation (r = −0.5987, N = 454, P < .05) was found between the socioeconomic status and the incidence of hip fracture in each region. There was 5.9% (n = 27) mortality rate posed by these hip fractures. The average duration of hospital stay was 14 days, with an average delay to surgical intervention of 2 days.
Conclusion:
Despite the Maltese Islands having a small population (429 344 people) and a free universal national health service, our results show that districts with low socioeconomic status had a higher incidence of hip fracture. Further studies using individual socioeconomic data and longer duration are required.
Introduction
Hip fractures, especially in the infirm elderly individuals, have a great impact on morbidity, mortality, and duration of hospitalization, with most of these patients becoming institutionalised. 1 –5 A coordinated multidisciplinary approach is essential in delivering the best management for hip fractures. This includes the input from orthopedic surgeons, nurses, and geriatricians; occupational therapists, physiotherapists; and social workers. 1 Occasionally, depending on the individuals’ comorbidities and complications, other medical or surgical specialties might be involved.
Despite hip fractures being a great public health problem, 1,3 –5 only few studies have analyzed the association between hip fractures and socioeconomic conditions. However, the relationship between hip fractures and socioeconomic status remains unclear. Most of these studies found an increased incidence, 2,4 –9 while others found a decreased incidence 10,11 of hip fractures with low socioeconomic status. Some studies found association with only some socioeconomic indicators. 12 –15 Other studies found increased risk of hip fractures for some socioeconomic indicators, and a decrease, or no association for other socioeconomic markers. 16 –20 However, not all studies found an association between hip fractures and socioeconomic status. 21
To our knowledge, there have not been any demographic studies of hip fractures in the Maltese Islands that were published. To overcome this, we conducted a population-based study in the Maltese Islands to analyze the relationship between hip fractures and individuals’ demographic data. This study goes further to analyzes the impact of regional-level socioeconomic status on the incidence of hip fractures in the Maltese Islands.
Method
Study Area
The study area was the Maltese Islands
The total population in these islands at the end of December 2014 was estimated at 427 344 people. 23 There were circa 126 more men than women, with a quarter of the total population being elderly aged 60 years or above. 23 The Maltese Islands consists of 6 districts (Figure 1). These include The Northern Harbour (29.4% of total population), Southern Harbour (18.6% of total population), South Eastern (15.6% of total population), Northern (15.4% of total population), Western (13.8% of total population), and Gozo and Comino District (7.4% of total population). 23 At-risk-of-poverty rate was highest for individuals residing in the Southern Harbour District, at 17%. This was the lowest in the South Eastern and Western Districts. 24

A map of the Maltese Islands showing the 6 districts. 22
Data
All individuals older than 50 years who presented to the acute care hospitals in Malta and Gozo with low-energy hip fracture between December 1, 2015, and November 30, 2016, were included in this study. They were identified using the hospitals’ imaging database. Using the hospitals’ discharge database, the data of the individual demographics were obtained. This included the sex and age of the individual together with the locality of residence. Data including the date, type, and side of hip fracture; date and type of surgical intervention (if surgery performed in Malta); and the date of discharge from hospital were also obtained using the hospitals’ discharge database. In-hospital mortality was obtained using the hospitals’ main software, i.Clinical Manager (i.CM) version 2.1, which provides the date and time when the patient was certified as deceased.
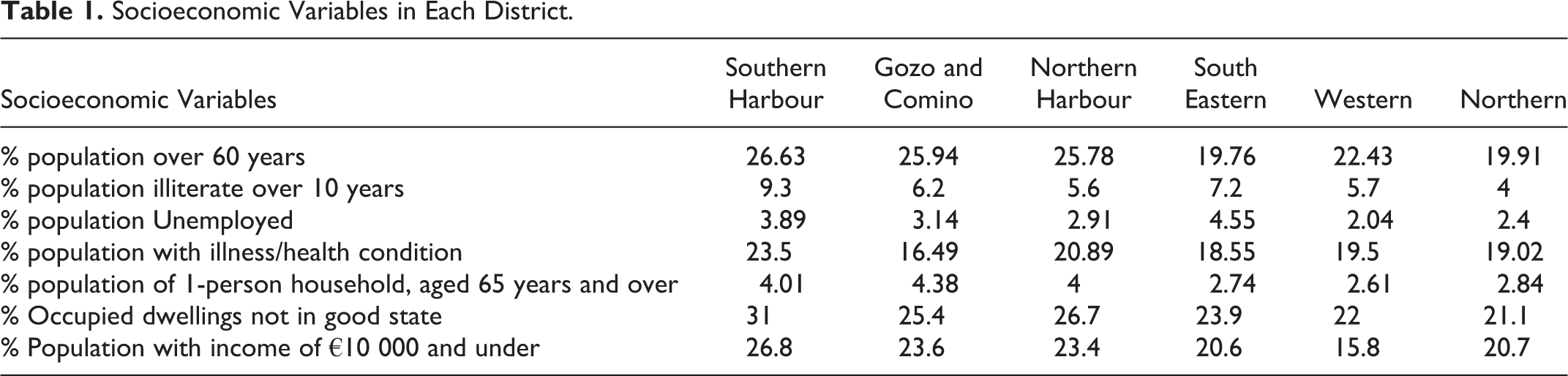
The socioeconomic status of each district was calculated using 7 socioeconomic variables. These included the percentage of population over 60; percentage of illiteracy over 10 years; percentage of unemployment; percentage of individuals with illness or health condition (chronic conditions requiring long period of supervision, observation or care); 25 percentage of individuals aged 65 and over living alone; percentage of occupied dwellings that are not in a good state (are in need of minor, moderate, serious repairs, or are dilapidated); 25 and percentage of population with an income of €10 000 and under in each district (Table 1). These data were obtained from the National Statistics Office, Malta. 24,25
Socioeconomic Variables in Each District.
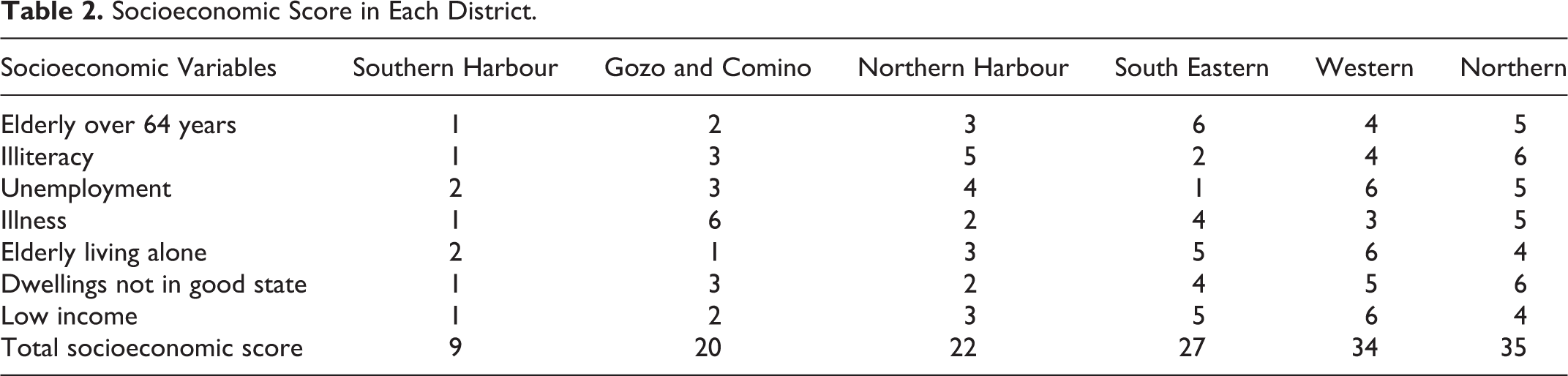
For every socioeconomic variable, each district was ranked. For every socioeconomic variable, 1 point was given to the district having the highest percentage of socioeconomic inequality, while 6 points were given to the district having the lowest percentage of socioeconomic inequality (Table 2).
Socioeconomic Score in Each District.
Statistical Analysis
The total points for each district were then tested for a significant correlation with percentage population above the age of 50 years, having sustained a hip fracture in each district. This was tested using Pearson correlation.
Results
There were 454 individuals older than 50 who presented to one of the acute care hospitals in Malta and Gozo between December 1, 2015, and November 30, 2016. The average age was 80.3 years, with females (n = 330) having almost a 3-fold risk of fracturing the hip than men (n = 124). The average delay to surgical intervention was 2 days, while the average hospital stay was 14 days. In-hospital mortality from these fractures was 5.9% (n = 27). Of all hip fractures, 5.3% (n = 24) occurred among foreigners who were holidaying in the Maltese Islands. Figure 2 shows the number of hip fractures and death in each month. The summer months having the lowest number of hip fractures and mortality.

A bar chart showing the number of hip fractures and deaths every month starting from December 2015 to November 2016 in the Maltese Islands.
The intertrochanteric fracture (n = 251) was then most common type of hip fracture, followed by intracapsular hip fracture (n = 155), subtrochanteric fracture (n = 37), and inter- and subtrochanteric fractures (n = 11; Figure 3). The most common type of surgical intervention was the dynamic hip screw (n = 258). This was followed by the Austin Moore hemiarthroplasty (n = 108), dynamic compression screw (n = 42), cemented total hip arthroplasty (n = 18), Thompson hemiarthroplasty (n = 10), cannulated screws (n = 8), and intramedullary nail (n = 3; Figure 4). In 7 individuals, no surgical intervention was carried out. Three individuals suffered mortality before the surgery, 2 individuals refused surgery, while another 2 were foreigners who preferred to undergo the surgical intervention in their country.

Bar chart showing the different types of hip fractures and their incidence from December 2015 to November 2016 in the Maltese Islands.

Bar chart showing the amount and types of surgical interventions for low-energy hip fractures from December 2015 to November 2016 in the Maltese Islands.
The Southern Harbour district had the highest rate of hip fractures (12.04 fractures per 10 000 individuals; n = 96; population: 79 741). This was followed by the Northern Harbour district (11.19 fractures per 10 000 individuals; n = 141; population: 126 027), Gozo and Comino (11.08 fractures per 10 000 individuals; n = 35; population: 31 592), the Western district (11.01 fractures per 10 000 individuals; n = 65; population: 59 063), the Northern district (7.26 fractures per 10 000 individuals; n = 48; population: 66 131), and the South-Eastern district (6.74 fractures per 10 000 individuals; n = 45; population: 66 790; Table 3).
Percentage Hip Fractures in Each of the 6 Districts.

Based on the score mentioned in the method section, the Southern Harbour district was found to have the lowest socioeconomic status (9 points). This was followed by Gozo and Comino (20 points), the Northern Harbour district (22 points), the South-Eastern district (27 points), the Western district (34 points), and the Northern district (35 points; Table 2).
The socioeconomic status of each district was tested using Pearson correlation for any relationship with the risk of hip fracture. A moderate negative correlation (r = −0.5987, N = 454, P < .05) was found (Figure 5).

Scatter plot showing the association between the socioeconomic score and the hip fractures per 10 000 individuals in each district.
Discussion
In this study, districts with a low socioeconomic status had a greater risk of hip fractures (Figure 5). Other studies with similar results include the study conducted by Quah et al. 6 The author used the English Indices of Multiple Deprivation 2007 (socioeconomic measurement) to analyze prospectively the relationship between socioeconomic status and the risk of hip fractures. It included individuals older than 65 years, between May 1991 and May 2009 in Queen’s Medical Centre, Nottingham. Populations with low socioeconomic status had 1.3 times higher incidence of hip fractures than the least deprived.
Oliveira published 2 papers 4,5 on her retrospective study in the Bone and Joint Decade (2000-2010) in Continental Portugal. Both show that for individuals between the age of 65 and 79 years, the incidence of hip fracture increases with lower socioeconomic status. However, this association disappears in women 80 years or older. Jones et al 8 in her population-based study in south, west, and north-eastern Wales, United Kingdom found that the risk of hip fracture was significantly higher in those with low Townsend scores (measurement of socioeconomic deprivation). Vidal et al 2 studied 352 patients with an age of 60 years or older who underwent surgery for hip fracture between 1995 and 2000 at a public university hospital in Rio de Janeiro, Brazil. In this study, 49% of patients had low socioeconomic status, while 60% of individuals were widowed, divorced, or single. Sanders et al 7 in a population-based 2-year retrospective study on osteoporosis in Australia, and Kaastad et al 9 in a similar study in Oslo, Norway, both showed an increased risk of hip fracture for individuals living in urban areas.
Johnell et al 12 conducted a study on 35 countries worldwide, Bacon and Hadden 13 in their study on US population, Guilley et al 14 in a study at Geneva university hospital in Switzerland, and Zingmond et al 15 in their study in California between 1996 and 2000, all show that individuals living in areas with low income have a higher risk of hip fractures. Furthermore, Zingmond et al 15 found that non-English speakers had a higher risk of hip fractures. Peel et al 3 in their study on the association of psychosocial factors with fall related hip fractures in Australia found that being married, living in present residence for 5 years or more, having private health insurance, using proactive coping strategies, having good level of life satisfaction, and participation in social activities in older age are all associated with a decrease in the incidence of hip fracture.
However, there were studies that found a decreased incidence of hip fracture with low socioeconomic status. These are the studies by Reyes et al 10 and Petit et al. 11 Reyes et al 10 , in a 3-year retrospective study of the Catalonian population in Spain found that people living in areas of lower socioeconomic status had a 30% lower risk of hip fracture. Petit et al conducted a study on French population in the year 2008. The risk of hip fractures was 2.42 times lower for those living in the most deprived areas compared to those living in the most affluent area. 11
There were studies that found increased risk of hip fractures for some socioeconomic indicators and a decrease or no association for other socioeconomic markers. 16 –20 A nationwide German study by Icks et al between 1995 and 2004 found that non-German population and those unemployed had a lower risk of hip fracture. 16 However, there was no association between income and the incidence of hip fractures. 16 Vestergaard et al, in his study in Denmark, also found no association between income and the incidence of hip fractures. However, low level of education, unemployment, and living alone were all associated with increased risk of hip fractures. Reimers and Laflamme in their study in Stockholm showed that being unmarried, and having low income increases the risk of hip fracture. 18 However, being born outside Sweden and having low social status were associated with a decreased risk of hip fracture. 18 Another study on Swedish population was conducted by Farahmand et al. This showed that married women who were gainfully employed and living in a 1-family house had lower risk of hip fracture. 17 However, employment and educational level were not associated with hip fracture risk. 17 Benetou et al found that individuals in Europe and United States with low education and living alone had higher hip fracture risk. 20
Not all studies found an association between hip fractures and socioeconomic status. In fact, West et al 21 published a 5-year retrospective study on all hospital admissions for falls and hip fractures between 1992 and 1997 aged 75 years or older in Trent, United Kingdom. Using the Townsend score as a measurement of socioeconomic status, despite an increased risk of falls was found with low socioeconomic status, there were no significant association between hip fractures and socioeconomic status.
As it can be seen from the literature review, only a few studies around the world have analyzed the association between risk of hip fracture and socioeconomic status. Most found an association; however, results are in part conflicting.
Our study used data form the National Statistics Office to calculate the socioeconomic status of each district. The absence of individual data to calculate each individual socioeconomic status is a limitation of this study. Another limitation of this study is that previous places of patients’ residence were not included. Participants in the study might have moved from one district to another. More specifically, elderly individuals living in deprived or isolated areas may have moved to another area, to live with or near relatives. This is not accounted for in this study. Another limitation of the study is that it was conducted over a period of only 1 year. We suggest that a future study of this area of study should be conducted over a period of a few years (maybe 3-5 years), in order to identify any patterns that occur across the years, which might confirm or refute our results.
Conclusion
Despite the Maltese Islands having a small population (429 344 people) and a free universal national health service, our results show that regions with low socioeconomic status have a higher incidence of hip fracture. However, further studies using individual socioeconomic data and longer duration are required. These studies will help in tailoring more effective preventative programmes that aim to reduce the risk of hip fracture.
Footnotes
Authors’ Note
This study was approved by the University of Malta Research Ethics Committee.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.