
Abstract
Introduction:
As life expectancy increases, the incidence of shoulder arthroplasty continues to increase as well. There are few shoulder arthroplasty studies investigating perioperative complication, readmission, and mortality. Furthermore, with bundled payments on the horizon, the cost of shoulder arthroplasty has become a significant issue. Clarifying risk factors for the need for postdischarge acute care will be critical information due to the high cost of such care. The goal of this study was to compare discharge disposition, length of stay (LOS), perioperative complications, readmission, and mortality in elderly and nonelderly cohorts to determine whether age is a risk factor for shoulder arthroplasty.
Materials and Methods:
We retrospectively compared 89 elderly patients (80 years or older) and 86 nonelderly patients (79 years or younger) who underwent hemiarthroplasty, total shoulder arthroplasty, reverse total shoulder arthroplasty, or revision shoulder arthroplasty from 2007 to 2015. Baseline characteristics were compared between the 2 cohorts. We then compared discharge disposition, LOS, 90-day complication rate, readmission, and mortality between the 2 cohorts.
Results:
Average length of hospitalization and percentage of patients with greater than 2 days of hospitalization were significantly higher in the elderly cohorts. Forty-four percent of the elderly cohorts were discharged to a skilled nursing facility compared to 6% in the nonelderly cohorts (P < .0001). There were no significant differences found in 90-day major complication rate, readmission, or mortality.
Discussion:
Shoulder arthroplasty is a valuable surgery for various indications in the elderly population. However, the likelihood of a patient to need a prolonged hospitalization or skilled nursing facility care after surgery are important questions that need to be answered. Our study shows that age over 80 years is a risk factor for prolonged hospitalization and need for skilled nursing facility care after shoulder arthroplasty.
Conclusion:
We conclude that elderly patients who undergo shoulder arthroplasty are significantly more likely to have extended hospitalizations and to be discharged to skilled nursing facilities compared to nonelderly patients.
Keywords
Introduction
The prevalence of shoulder osteoarthritis and arthropathy will continue to rise with the aging of our population, leading to a greater number of elderly candidates for shoulder arthroplasty. Kim et al found that from 2000 to 2008 shoulder arthroplasty overall increased 2.5-fold and 3.5-fold in the elderly candidates, which they defined as age 65 and older. 1 Although literature reporting perioperative complication risk and cost analysis is vast in the total hip and total knee arthroplasty, it is in its infancy in the shoulder arthroplasty literature. 2 With bundled payments on the horizon, health-care providers need to better understand prognostic patient factors for increased service utilization in the postoperative period, such as the use of skilled nursing facilities (SNFs) and home health care. In the hip and knee arthroplasty literature, one study has shown that 40% of the entire cost for a single episode of total joint arthroplasty is spent on post-hospital discharge care. 3 Furthermore, SNFs represent 45% of these post-discharge payments after hip or knee arthroplasty. 3 In 2014, payments to SNFs totaled nearly US$29 billion in Medicare expenditures 3 and daily charges at SNFs following hip and knee arthroplasty averaged US$486. 4 Although there are obvious limitations comparing shoulder arthroplasty to hip and knee arthroplasty, the fact is that there is very little shoulder arthroplasty literature on post-hospital discharge and cost, especially pertaining to SNFs. Although discharge-to-home rates are higher in shoulder arthroplasty (67%) 5 compared to hip and knee arthroplasty (58%), 3 there is still a large proportion of patients who need post-hospital discharge subacute care. Clarifying risk factors for complications, readmission, and likelihood of the need for post-discharge acute care in this population is of the utmost importance in helping to define post-hospital course and care expenditures.
Several studies in the shoulder arthroplasty literature have reported on perioperative outcomes of the elderly candidates with mixed results, but most of these studies only followed their patients through discharge, 30-day follow-up, or 60-day follow-up 6 -8 or did not report a date range. 9 These studies are not adequate, though, as single payment bundles are covering up to 90 days after discharge. During this time, the stakeholders in the bundle are liable for all costs of patient treatment, regardless of whether readmissions are related to the index surgery. 10 Although procedures in this study were not part of a bundled payment initiative, 90-day outcome data are necessary to fully define at-risk populations for shoulder arthroplasty. The goal of this study was to compare the elderly candidates (80 years old and above) to younger adults (79 years old and younger) with regard to discharge disposition, 90-day perioperative complications including revision arthroplasty, 90-day readmission, and 90-day mortality, which will have significant cost implications in the future.
Materials and Methods
We used a retrospective cohort design for this study. We identified all patients who had undergone hemiarthroplasty, total shoulder arthroplasty (TSA), reverse total shoulder arthroplasty (RTSA), or revision shoulder arthroplasty from 2007 to 2015. All surgeries, preoperative, and postoperative clinic visits took place at Virginia Commonwealth University in Richmond, Virginia. All surgeries were performed by a single fellowship-trained shoulder and elbow surgeon (N.D.B.). All patients underwent general anesthesia with a supraclavicular or interscalene nerve block. A total of 109 patients aged 80 or older (mean age: 84.0 years) who underwent hemiarthroplasty, TSA, RTSA, and revision arthroplasty were identified. Eighty-six of these patients (1 hemiarthroplasty, 24 TSA, 49 RTSA, and 15 revisions) had at least a 90-day follow-up (average 20.7 months) and were included in the study. Three additional patients died within the 3-month perioperative period but were included in the analysis. We then randomly identified 109 patients aged 79 or younger (mean age: 60.7 years) who had undergone the same procedures during the same time period. Eighty-five of these patients with at least 90-day follow-up and 1 patient who died in the 90-day postoperative period were included in the analysis. Eleven hemiarthroplasties, 42 TSR, 30 RTSA, and 3 revision arthroplasties were included. Preoperative comorbidity data were collected and compared between the 2 cohorts (Table 1). The analyzed variables included obesity status (body mass index ≥30), history of diabetes mellitus, coronary artery disease (CAD), stroke or transient ischemic attack, deep venous thrombosis (DVT) or pulmonary embolism (PE), atrial fibrillation (A fib), hypertension, chronic kidney disease, obstructive sleep apnea, hypothyroidism, anemia, asthma, and chronic obstructive pulmonary disease. Our primary outcome measure was discharge disposition (home vs SNF). Secondary outcome measures included length of stay (LOS), major complications, readmission rates, and mortality. Major complications included organ space infection, sepsis, transfusion, reintubation or delayed weaning off of the ventilator, cardiac event, neurological event, pneumonia, venous thromboembolism, return to the operating room, and acute renal failure.
Baseline Characteristics.

Abbreviations: A fib, atrial fibrillation; CAD, coronary artery disease; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; DM, diabetes mellitus; DVT, deep venous thrombosis; HTN, hypertension; OSA, obstructive sleep apnea; PE, pulmonary embolism; TIA, transient ischemic attack.
For our statistical analysis, we performed an a priori power analysis based on a previous study 11 and determined a sample size of 79 patients needed in each cohort to detect a 20% difference in the proportion of patients discharged to an SNF. Pearson χ2 tests (or Fisher exact tests, where appropriate) were used for categorical variables. Two-tailed student t tests were used for continuous variables. Relative risks (RRs) with 95% confidence interval (CI) were calculated for each variable. P Values less than .05 were considered significant. We also performed a subgroup analysis on discharge disposition and LOS for 3 different time periods based on the year of surgery (2007-2009, 2010-2012, and 2013-2015). This analysis was done to ensure that changing trends in patient discharge following shoulder arthroplasty would not be confounding variables in our conclusions. All statistics were performed on IBM SPSS Statistics version 24.
Results
Thirty-nine (44%) of the 89 patients in the elderly cohort were discharged to an SNF compared to 5 (6%) of 86 in the nonelderly cohort (RR = 7.5, 95% CI: 3.1-18.2, P ≤ .0001). Average length of hospitalization was 3.6 days (4.9 for SNF-bound patients and 2.6 for home-bound patients) in the elderly cohort compared to 2.2 days (4.4 for SNF-bound patients and 2.1 for home-bound patients) in the nonelderly cohort (P ≤ .0001). Fifty-two (58%) of the 89 patients in the elderly cohort had a hospital stay greater than 2 days compared to 18 (21%) of 86 in the nonelderly cohort (RR = 2.8, 95% CI: 1.8-4.4; P = .0013). The 90-day mortality rate was 3.4% in the elderly cohort compared to 1.1% in the nonelderly cohort (RR = 2.9, 95% CI: 0.3-27.3, P = .35). Ninety-day major complications occurred in 19% of the elderly cohort compared to 10% of the nonelderly cohort (RR = 1.9, 95% CI: 0.9-3.9, P = .08). In the elderly cohort, there were 8 cases of acute renal failure, 2 strokes, 1 PE, 2 DVTs, 1 case of pneumonia, 2 myocardial infarctions, and 1 case of A fib with rapid ventricular response requiring transfer to intensive care unit. In the nonelderly cohort, there were 4 cases of acute renal failure, 1 seizure, 1 reintubation postoperatively, and 3 cases of return to the OR. The cases requiring return to OR included 1 periprosthetic fracture, 1 prosthesis dislocation, and 1 surgical wound requiring irrigation and debridement. The 90-day readmission rate was 3.4% in the elderly cohort versus 4.7% in the nonelderly cohort (RR = 0.72, 95% CI: 0.2-3.1, P = .66). These results are summarized in Table 2.
Summary of Results.
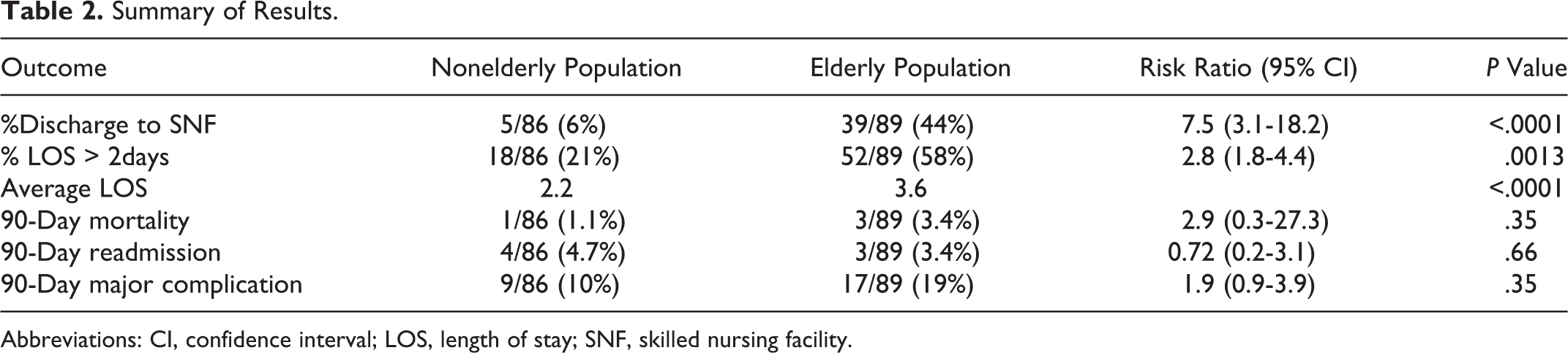
Abbreviations: CI, confidence interval; LOS, length of stay; SNF, skilled nursing facility.
A subgroup analysis of discharge disposition and LOS was also performed for the following time periods based on the date of surgery: 2007 to 2009, 2010 to 2012, and 2013 to 2015. The number of patients in each subgroup by cohort was as follows: 2007 to 2009 group—16 elderly candidates and 25 nonelderly candidates, 2010 to 2012 group—31 elderly candidates and 30 nonelderly candidates, 2013 to 2015 group—42 elderly candidates and 31 nonelderly candidates. The 2007 to 2009 group had a significantly lower rate of discharges to SNF (10%) compared to the 2010 to 2012 group (27%, P = .04) and the 2013 to 2015 group (32%, P = .01). The rates of SNF discharge were not different between the 2010 to 2012 and 2013 to 2015 groups (P = .53). Length of stay in the hospital was significantly longer in the 2013 to 2015 group (3.8 days) compared to the 2007 to 2009 group (2.3 days, P = .01) and the 2010 to 2012 group (2.8 days, P = .04). There was a trend but no significant difference between LOS in the 2007 to 2009 and 2010 to 2012 groups (P = .07).
Discussion
As patient life expectancy continues to increase, a concomitant increase in the prevalence of shoulder arthritis and demand for shoulder arthroplasty is expected. Shoulder arthroplasty is and will continue to be a valuable surgery for various indications in the elderly population. However, precise indications and contraindications need to be further defined. A systematic review of 23 studies from 2007 showed consistent improvements in pain, range of motion, and patient satisfaction in patients of all ages undergoing shoulder arthroplasty. 12 In particular, satisfaction was reported as 97% in TSA and 80% in hemiarthroplasty.
Success in shoulder arthroplasty has also been reported in the extremely elderly population. Churchill reported on 7 shoulders in 6 patients aged 90 or older who underwent shoulder arthroplasty with a 2-year follow-up. 13 There were no deaths or complications in the 90-day postoperative period. One death occurred 13 months after surgery from pneumonia. The author reported significant improvements in SF-36 scores and concluded that shoulder arthroplasty is a safe and effective procedure in carefully selected patients older than 90. Ricchetti et al compared 90-day outcomes in patients aged 80 years or older to those aged 50 to 69. 11 They found no differences in complication rates between the 2 groups but did report an increased transfusion rate and decreased rate of discharges to home in the elderly group. They reported no deaths. They concluded that there were no differences in complication rates between elderly and middle-age adults undergoing TSA, although they only had 40 and 46 patients in each arm of the study.
In our study, LOS, percentage of patients staying over 2 days, and percentage of patients discharged to SNFs were all higher in the elderly population. There was no difference in readmission rate, major complication rate, or mortality rate. However, our study was likely not powered to detect these differences if they exist.
Our subgroup analysis by time period of surgical date produced some interesting results. We had predicted that discharge disposition would have led to a larger percentage of home discharges and that LOS would decrease as time progressed. Our analysis revealed just the opposite. The LOS in the 2013 to 2015 group was significantly longer than the earlier 2 time periods and discharge to SNF was significantly lower in the 2007 to 2009 group compared to the later time periods. Part of these results can be explained by a higher number of elderly patients having surgery during each successive time period (16 in 2007-2009, 31 in 2010-2012, and 42 in 2013-2015). This increase in elderly patients undergoing shoulder arthroplasty is consistent with the nationwide trend 1 and is a great example of the importance of investigating outcomes of shoulder arthroplasty in this population.
Strengths of our study include that it was adequately powered for our primary outcome variable, discharge disposition. This study also follows perioperative outcomes for 90 days, which should be the new benchmark for outcome studies in shoulder arthroplasty. Weaknesses include the retrospective nature of the study and the inclusion of multiple types of arthroplasty with different proportions of each surgery in each cohort. Also the study was almost certainly underpowered to detect significant differences in 90-day mortality, 90-day readmission, and 90-day major complication rate. Also, prevalence of CAD, asthma, and sleep apnea was significantly different between the 2 cohorts and may have been confounding variables influencing our results. Finally, this was a study of a single surgeon at a single institution, so the external validity of this study could be questioned.
Conclusion
We believe this study shows that elderly patients are much more likely to have prolonged hospital stays and be discharged to SNFs, both of which are associated with significantly increased costs. We also believe, in light of this study’s findings, that the surgeon should have a detailed discussion with elderly patients regarding their postoperative course and likelihood to be discharged to home versus SNF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Douglas Boardman has financial relationships with Depuy and Biomet.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.