
Abstract
Introduction:
Eccentric (negative) resistance exercise of the legs using specialized machines has been reported to be useful and often superior to standard exercise following total knee arthroplasty (TKA). Movements that utilize body mass and gravity as a mode of eccentric resistance exercise in a more pragmatic rehabilitation paradigm may also be useful in reversing chronic muscle impairments observed years following surgery. This study explores whether an eccentrically biased, body mass resistance exercise induces greater magnitude of sagittal plane extensor angular impulse of the support torque and individual net joint torque contributions during both squatting and lunging movement patterns 6 weeks following TKA.
Methods:
Cross-sectional laboratory-based study design including 10 patients following primary unilateral TKA (6.5 ± 0.8 weeks.). All patients completed 3 trials of the squat and lunge movement pattern under both a concentric and an eccentric condition. Extensor angular impulse of the support torque and net joint torque contributions were calculated by integrating the joint torque versus time curves. A Two-way analysis of covariance was conducted and contracts of clinical interest were computed using Wald posttest. P Values for all pairwise comparisons were adjusted for multiplicity using Bonferroni multiple comparison procedure.
Results:
The eccentric condition, compared to the concentric condition, displayed larger magnitude of extensor angular impulse during both the squat (P < .001) and lunge (P < .001) movement patterns for the support torques. Similarly, the eccentric condition, compared to the concentric condition, displayed larger magnitude of extensor angular impulse of the hip, knee, and ankle (P < .001) during both movement patterns.
Conclusion:
Eccentrically biased, body mass movement exercises can produce higher levels of extensor angular impulse on the surgical limb in patients early after TKA. Patients in this study were able to tolerate the higher extensor angular impulse demands and performed the eccentrically biased conditions (without specialized machines) that could be beneficial in postoperative rehabilitation.
Keywords
Introduction
Greater than 600 000 total knee arthroplasty (TKA) procedures are performed annually to relieve arthritic knee pain in the United States, with estimates of an increase to 3.48 million surgeries by 2030. 1,2 Select geriatric, orthopedic, and rehabilitation journals highlight the impact of this by reporting TKA outcomes as their most highly cited papers. 3 Despite excellent pain relief, the increasing frequency of and spotlight on TKA physical function lags behind especially during higher demand tasks requiring increasing amounts of muscular strength. 4 With that, rehabilitation countermeasures are being modified and new approaches explored. Most patients do perceive and self-report their functional outcomes as generally improved in comparison with preoperative measures. 5 -7 However, performance-based measures of physical function, such as timed walking, chair rising, and stair climbing, reveal only marginal improvements after surgery. 8 -10 These deficits are considered recalcitrant and persist years following surgery. 11
Chronic muscle weakness has been directly related to these impaired functional performance measures, particularly deficits of the hip and knee extensor muscles. 11 -16 Lower limb muscle weakness is prevalent in persons with knee arthritis, and approximately 60% of preoperative quadriceps strength is lost within the first month following surgery. 12,17,18 Further, an approximate 20% quadriceps strength deficit 19 -21 is positively linked to impairments in mobility and physical activity 11,22 and muscle dysfunction remains as long as 12 months postoperatively. Lower limb strength can improve following surgery, though restoration of the surgical limb strength to levels of the contralateral limb or that of healthy matched peers rarely occurs. 11
Muscles undergoing eccentric (negative) loading provide greater strength adaptations as compared to concentric (positive) loading. 23 Eccentrically based resistance exercise as a rehabilitation approach following orthopedic surgery of the knee has been very successful with amplified muscle size of the lower limb extensors and physical function improvements that exceed traditional modes of resistance exercise. 24 -26 Eccentrically based strength and movement training are important modes of TKA postoperative rehabilitation as limitations in commonly reported daily and recreational activities (ie, squatting, descending stairs, hiking) are related to impairments in joint function during tasks requiring eccentric muscle activity. 13 Due to its lower metabolic demand and greater force production, eccentrically based rehabilitation has the capacity to accelerate strength and facilitate movement patterns earlier in the rehabilitation process. 25,27 Most studies have described eccentrically based rehabilitation training as designed to externally load joints using highly specialized expensive equipment that may not be available nor pragmatic in many rehabilitation settings. In lieu of specialized exercise equipment, eccentrically based rehabilitation that externally loads the lower limb joints via a patients’ own body mass may be more feasible and as effective in promoting muscle and movement training shortly following TKA.
Traditionally, standard rehabilitation exercises focused on whole-body movement involve an equal amount of both concentric and eccentric muscle activity. By emphasizing and temporally extending the eccentric component of movement using the patients’ own body mass, a greater joint load onto the surgical limb may be possible. This greater demand on the muscle may better prepare patients following TKA who are weak and continue to struggle with tasks requiring eccentric muscle control. Angular impulse of each joint is a surrogate measure of muscle demand, that is, muscle force production of the lower limb, and is simply derived from the extensor torque curves during functional tasks. 28 No study has compared the joint kinetic angular impulse differences using simple whole-body movements (ie, squatting and lunging) that eccentrically bias the exercise by temporally extending the eccentric movement component relative to the concentric movement component during the early stage of TKA postoperative recovery.
Therefore, the purpose of this study was to compare the lower limb extensor angular impulse between 2 conditions, standard eccentric/concentric versus an eccentrically biased eccentric/concentric approach, during rehabilitation activities (squat and lunge movements). We hypothesized that the eccentrically biased condition would result in a greater magnitude of sagittal plane extensor angular impulse of the support torque during both the squat and lunge movement patterns at 6 weeks following TKA. We further hypothesized that the eccentrically biased condition would result in a greater magnitude of the sagittal plane extensor angular impulse of the individual lower limb joints (hip, knee, and ankle) during both movement patterns.
Methods
Participants
A cross-sectional laboratory-based study was conducted that recruited patients who underwent a primary unilateral TKA between January 2015 and January 2016 and met the following inclusion criteria: between 45 and 70 years of age; body mass index (BMI) less than 40; University of California, Los Angeles (UCLA) activity scale of greater than or equal to 3; and no prior knee joint replacement procedure to either limb. All TKA participants were evaluated at 6 weeks from surgery (mean, 6.5 ± 0.8 weeks) and were all attending outpatient physical therapy. All surgical procedures were performed by 1 of 3 board-certified orthopedic surgeons and were recruited from the University of Utah Orthopaedic Center (Salt Lake City, Utah). All testing was completed in a single session at the Motion Capture Core Facility, Department of Physical Therapy and Athletic Training, University of Utah. Each participant was informed of the procedures and informed consent was verified via a signed document approved by the institutional review board of the University of Utah.
Instrumentation
Kinematic data were captured using a 10-camera 3-dimensional (3D) motion analysis system (Vicon; Oxford Metrics LTD, Oxford, United Kingdom) at a sampling frequency of 200 Hz. Ground reaction force data were obtained using 2 embedded force platforms (Advanced Mechanical Technologies, Inc, Newton, Massachusetts) at a sampling rate of 1000 Hz. All synchronization of kinematic and kinetic data was digitally converted to a single laboratory computer for data collection and postprocessing.
Testing Procedures
Prior to the participant’s entry into the laboratory, the system was calibrated and anthropometric measures were obtained. Participants wore compressive shorts, shirt, and their own athletic shoes. A virtual model and attributing coordinate systems for each segment was computed based on 50 spherical retroreflective markers placed on the following landmarks: seventh cervical spinous process, manubrium of the sternum, inferior body of the sternum, bilaterally on the anterior/posterior superior iliac spines, right spine of scapula, iliac crests, greater trochanters, acromions, medial and lateral epicondyles of the femurs, medial and lateral malleoli, first and fifth heads of the metatarsals, dorsum of the feet, and calcaneal tuberosities. One rigid cluster with 4 noncollinear markers was placed at the base of the lumbar spine and 2 nonrigid clusters with 4 noncollinear markers were placed at the lateral side of each thigh and shank.
All participants completed 3 trials of both movement patterns (squatting and lunging) under 2 distinct conditions (concentric and eccentric). For the squatting movement pattern, participants were instructed to lower their body mass down (approximately 75° knee flexion position) and return to the starting position (approximately 0° knee flexion; Figure 1). For the lunging movement pattern, participants were instructed to step with their surgical limb from one force platform to the other, while lowering their body mass down (approximately 60° knee flexion position) and return to the starting position (approximately 0°; Figure 2). For both movement patterns, participants were instructed to provide equal weight or as much weight through the surgical limb as tolerable. The concentric condition was defined as the participants spending equal amount of time (3 seconds) during both the lowering (eccentric) and rising (concentric) phases for both movement patterns. The eccentric condition was defined as the participants spending a longer duration (5 seconds) during the lowering phase and a shorter duration during the rising (1 second) phase for both movement patterns. Once participants were instructed to begin, a temporal countdown was performed to allow the participants to constrain the timing for each condition. Trials in which participants lost their balance, used their upper arms for support, or stepped off the adjacent force platform were excluded. The average of the 3 trials for each movement pattern within each condition was computed for statistical analysis.
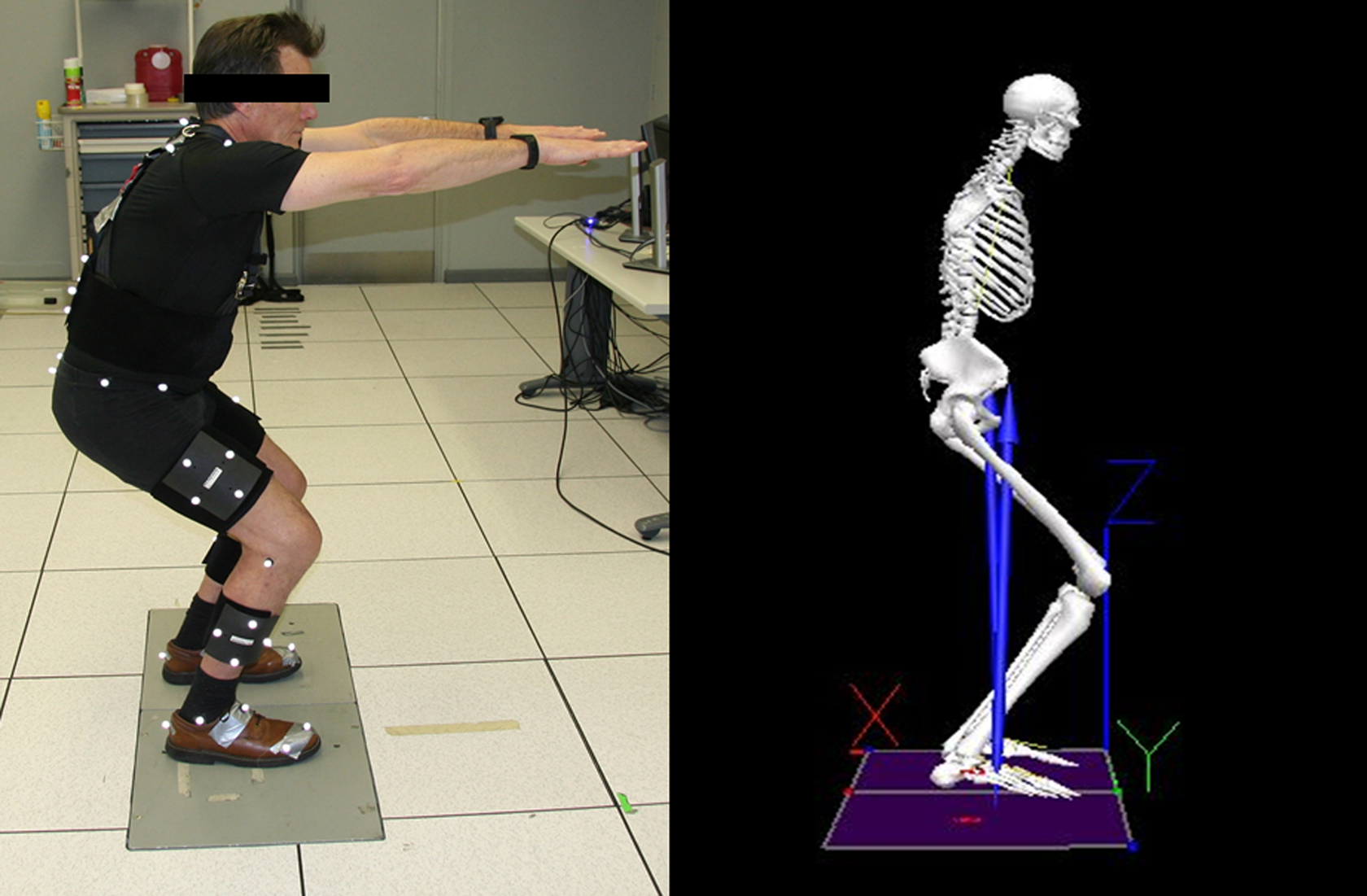
Patient with total knee arthroplasty performing the squatting movement pattern (left) and 3-dimensional (3D) motion capture model illustration (right).
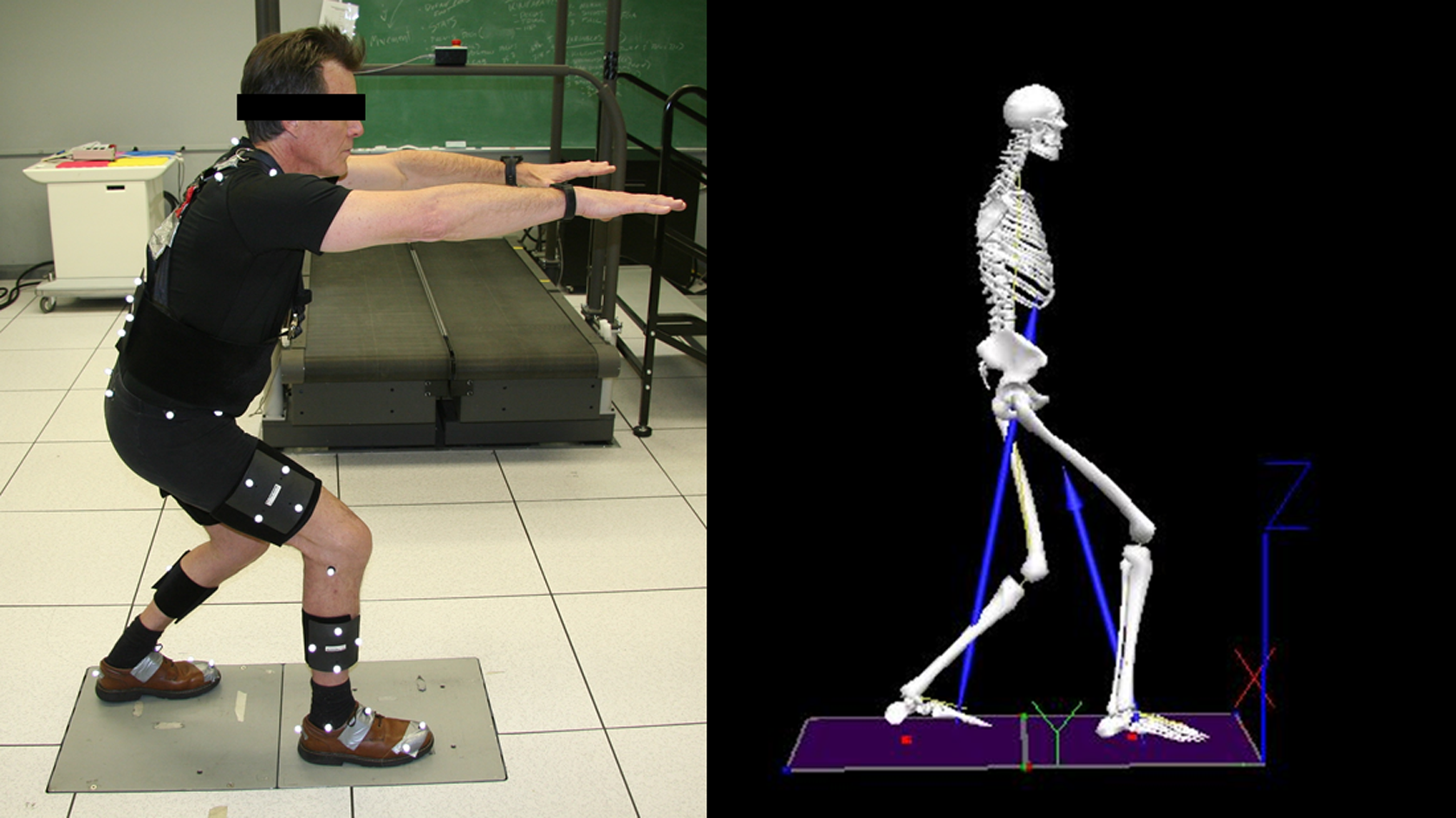
Patient with total knee arthroplasty performing the lunging movement pattern (left) and 3-dimensional (3D) motion capture model illustration (right).
Patient-Reported Measures
The National Institutes of Health’s Patient-Reported Outcomes Information System (PROMIS) was used to characterize each participant’s physical function and pain interference. 29,30 Prior to data collection, participants completed both computerized adaptive testing (CAT) domains for physical function item bank v1.2 (PF-CAT) and pain interference item bank v1.1 (PI-CAT). The PF-CAT includes a multitude of physical function items across 5 domains of physical performance: upper extremity, lower extremity, axial, central, and instrumental activities of daily living. The PI-CAT evaluates the extent pain affects participants’ engagement with social, cognitive, emotional, physical, and recreational activities. The PROMIS CAT measures use a T score metric in which 50 is the mean for the US general population and 10 is the standard deviation of that population. 31 These instruments have shown to be reliable and valid in various orthopedic patient populations. 31 -34 Following data collection, participants completed the numeric pain rating scale (NPRS). This NPRS consists of an 11-point numeric scale, with 0 meaning no knee pain and 10 meaning the worst knee pain imaginable. It has shown to be a validated instrument and used in several musculoskeletal conditions. 35,36 The UCLA activity scale is a validated instrument measuring physical activity level and has been well utilized in patients with TKA. 37 Participants indicate the most appropriate activity level on a scale ranging from 1 to 10, with 1 defined as “no physical activity, dependent on others” and 10 defined as “regular participation in impact sports.” Patient-reported measures were collected to demonstrate the subjective response of the participants and provide context for generalizability of the collected cohort.
Data Analysis
Coordinate data were recorded and digitized using Nexus 2.1.1 (Vicon; Oxford Metrics LTD). Postprocessing and extraction of kinetic and kinematic data was conducted using Visual3D v6.00.27 (C-motion, Inc, Germantown, Maryland). Marker trajectory and analog data were filtered using a fourth-order Butterworth low-pass filter at 6 and 12 Hz based on residual analysis. 38 Kinematics were calculated for all lower limb joints using a visual 3D model with a Cardan sequence (x, y, and z). Standard inverse dynamic methods were used to calculate the joint reaction forces and sagittal plane torques at each lower limb joint throughout each movement pattern. Angular impulse at each lower limb joint was calculated by taking the area under the sagittal plane torque–time curve during each movement pattern and provides a more comprehensive assessment than peak torque values. 39 Data were normalized by body mass (kg). Individual and summed joint torque curves were then calculated for the lower limb joints, negated to represent a positive torque versus time curve, and used to provide a visual description of joint mechanical output for each condition (Figures 3 and 4). The extensor angular impulse during the eccentric and concentric phases was calculated for the hip, knee, and ankle torque as the areas under the sagittal plane torque–time curves. The extensor angular impulse during the eccentric phase was calculated as a net summation from the period starting from the initial standing position to the peak knee flexion position. The extensor angular impulse during the concentric phase was calculated as a net summation from the period starting from the peak knee flexion position to the ending standing position. Outcome variables were computed as a difference score, calculated as the difference between extensor angular impulse value during the concentric phase minus the value during eccentric phase for each movement pattern. A negative value signified greater extensor angular impulse during the eccentric phase, while a positive value signified greater extensor angular impulse during the concentric phase. General assumption based on previous studies 28,40 is that joint torques during movement are primarily produced by muscle forces and therefore angular impulse from joint torques (ie, area under the joint torque–time curves) is a reasonable estimate of muscle demand.

Representative example of the summed (black solid line) and individual joint torques (hip [purple dotted line], knee [blue dashed line], ankle [red dash dotted line] for the concentric [left] and eccentric [right] condition squatting movement pattern). Joint torques were negated to represent the positive extensor output across each joint during the movement pattern. Vertical line represents the division of the eccentric and concentric components of the movement pattern.

Representative example of the summed (black solid line) and individual joint torques (hip [purple dotted line], knee [blue dashed line], ankle [red dash dotted line] for the concentric [left] and eccentric [right] condition lunging movement pattern. Joint torques were negated to represent the positive extensor output across each joint during the movement pattern. Vertical line represents the division of the eccentric and concentric components of the movement pattern.
Statistical Analysis
A Two-way analysis of covariance was conducted that examined the effect of the movement pattern (squat and lunge) and condition (concentric and eccentric) with an interaction term on lower limb extensor angular impulse after comparing contracts of clinical interest that were selected a priori using Wald posttest. P values for all pairwise comparisons were adjusted for multiplicity using Bonferroni multiple comparison procedure. 41 Effect sizes were computed as paired mean differences (Cohen d) for all outcome variables. 42 An a priori sample size calculation analysis was conducted based on previous work using peak knee extensor torque 43 and indicated 10 participants would be needed to detect within-subject differences, which provides 80% power with a 2-sided α of .05. Data were analyzed using commercially available statistical software (Stata v14.1; Statacorp, LP, College Station, Texas).
Results
Participants
Ten participants (mean age, 61.0 ± 7.7; mean BMI, 30.6 ± 3.5; 40% male) who underwent a primary unilateral TKA surgery were enrolled in the study (Table 1). Participants reported average pain (mean, 57.9 ± 7.5) and below average physical function (mean, 37.7 ± 3.6) levels compared to the national average based on the PROMIS measures. Following data collection, participants reported minimal to mild pain knee pain (mean, 3.0 ± 1.8) based on NPRS measures.
Baseline Characteristics of Study Participants.

Abbreviations: BMI, body mass index; NPRS, numeric knee pain rating scale; PF-CAT, physical function computerized adaptive testing; PI-CAT, pain interference computerized adaptive testing; UCLA, University of California, Los Angeles.
aValues represented as mean (SD) unless otherwise stated.
Joint Kinetics
Analysis of covariance revealed the eccentrically biased condition and, compared to the standard condition, displayed larger magnitude of extensor angular impulse during both the squat (P < .001; Cohen d = 6.05) and lunge (P < .001; Cohen d = 3.72) movement patterns for the support torques (Table 2). Pairwise comparisons indicate large effect sizes, in favor of the eccentric condition in increasing the extensor angular impulse of the entire limb during both squat and lunge movement patterns.
Between-Condition Comparisons of Lower Limb Extensor Angular Impulse During the Squat and Lunge Movement Patterns.

Abbreviations: CI, confidence interval; Diff, difference; M, mean, SE, standard error.
aEffect size categories (0.20 = small, 0.50 = medium, and 0.80 = large).
bAdjusted for multiplicity using the Bonferroni multiple comparison procedure.
cValues expressed as a difference score, calculated as the difference between extensor angular impulse value during the concentric phase minus the value during eccentric phase for each movement pattern. (−) value signified greater extensor angular impulse during the eccentric phase and (+) value signified greater extensor angular impulse during the concentric phase.
Our analysis revealed the eccentrically biased condition and, compared to the standard condition, displayed larger magnitude of extensor angular impulse of the hip (P < .001; Cohen d = 2.60), knee (P < .001; Cohen d = 3.45), and ankle (P < .001; Cohen d = 2.79) during the squatting movement patterns (Table 2). Additionally, our analysis revealed the eccentrically biased condition and, compared to the standard condition, displayed larger magnitude of extensor angular impulse of the hip (P < .001; Cohen d = 1.98), knee (P < .001; Cohen d = 3.33), and ankle (P < .001; Cohen d = 1.24) during the lunging movement patterns (Table 2).
Discussion
We evaluated the joint kinetic differences between 2 conditions (concentric vs eccentric) on lower limb extensor angular impulse during common functional movement patterns (squat and lunge) considered clinically feasible in a rehabilitation setting following a primary unilateral TKA. The principal findings were as follows: (1) participants during the eccentrically biased condition demonstrated significantly larger magnitude of extensor angular impulse of the support torque compared to the standard condition during both movement patterns; (2) participants during the eccentrically biased condition demonstrated larger magnitude of extensor angular impulse for each lower limb joint (hip, knee, and ankle) torques compared to the standard condition during both movement patterns; and (3) participants reported minimal to mild pain levels based on NPRS following the movement patterns, thereby supporting the notion these movement are feasible in a rehabilitation setting.
The laboratory findings from this study are significant as the benefits of eccentrically biasing resistance exercise have been repeatedly highlighted (see reviews of eccentric rehabilitation 27,44 ). These findings suggest the previous strength and mobility results of eccentrically loading the postoperative knee could be approximated when using a patient’s body mass during standard whole-body movements. The clinically pragmatic squat and lunge movement rehabilitation approach that increases the temporal component of the eccentric condition to address postoperative weakness deemphasizes the need for specialized equipment, especially during the early postoperative period. We did not compare the eccentric loads of a motorized ergometer verses body mass–induced eccentric loading. We expect the former can induce greater loading, though the latter eccentrically biased movement using body mass clearly can provide a large magnitude of extensor angular impulse through the surgical limb early after surgery. Further, incorporating whole-body movements that many patients with TKA find challenging targets the increasing joint demand requirements of the more physically active patient. Published clinical guidelines endorse eccentric resistance exercise using specialized equipment as an important rehabilitation approach following surgical reconstruction of the knee. 25 -27,44 Further, patients with TKA have responded favorably to eccentric loading on a motorized ergometer during both the early after surgery period 25 and late (1-2 years) 24 after surgery period when muscular weakness was thought to be irreversible.
Despite the evidence and recommended use of specialized ergometers, most rehabilitation settings do not have this equipment. However, our laboratory findings expose a higher extensor demand does occur at all lower limb joints, and upon the related musculature, with whole-body movements that emphasize the eccentric phase. This is not a surprising outcome as the tasks were eccentrically biased, but the joint kinetic demand has never been documented. This being a novel finding may underscore why the temporally longer eccentric phase of movement has not been regularly implemented in rehabilitation exercise programs following TKA.
Finally, patients with TKA can perform eccentrically biased movement patterns early post-TKA with mild knee pain, while enduring greater kinetic demand to the extensor musculature. These findings are clinically relevant as a major limitation early after surgery is persistent muscular weakness and atypical movement patterns that persist for years following surgery along with associated impairments in functional tasks. 15,16,45,46 Impaired walking, 46 chair rise 45 and stair climbing 47 ability are commonly reported, resulting in smaller extensor torque contributions from the surgical limb compared to the nonsurgical limb. Furthermore, functional tasks requiring eccentric control are the most challenging for patients with TKA 4,48,49 and the rehabilitation potential of eccentrically biased squats and lunges may be more readily transferrable to high-demand physical functional tasks such as negotiating stairs and obstacles that many patients would like to execute with confidence. These preliminary findings are encouraging in that these approaches could be integrated into a functional movement retraining rehabilitation program focused on retraining proper motor patterns and increased extensor musculature demand. Further research is needed to determine whether motor retraining using eccentrically biased movement patterns can be as effective as eccentric loading on a motorized ergometer at improving functional performance through a longitudinal cohort study.
This study has limitations that need to be considered when interpreting the data. First, data were acquired using conventional link segment mechanics and inverse dynamic methods to measure joint torques; however, musculoskeletal modeling or electromyography was not conducted to estimate muscle activity during the movement patterns. Our joint kinetic findings provide estimates of the extensor musculature demands, but further investigation would be needed to provide a more valid measurement. Second, the sequence of the 2 conditions were not randomized, which could have introduced potential bias in the results. Third, only 3 trials of each movement pattern were collected for statistical analysis and additional trials would need to be performed to effectively address appropriate dosage for a framework to a rehabilitation intervention. Fourth, the study design is not appropriate to determine any clinically relevant strength, movement, or performance improvements over time nor does it address the effects of differential loading that might occur when using body mass versus an eccentric ergometer. Future study is needed to determine effectiveness of this alternative mode of postoperative retraining. Fifth, multiple surgeons and implant designs were involved in this study, which could have influenced the results. Sixth, we did not track duration, type, or quality of physical therapy services provided, which could have influenced our results.
Conclusion
Eccentrically biased movements can produce higher levels of extensor angular impulse on the surgical limb in patients early after TKA. Patients in this study appeared to tolerate the higher extensor angular impulse demands and performed the eccentrically biased movement tasks (without a specialized machine); therefore, eccentrically biased movements could be beneficial in postoperative rehabilitation.
Footnotes
Authors’ Note
All authors contributed to the study design, data collection, data analysis and interpretation, drafting and revision of the article, and final approval of the article. The institutional review board of University of Utah (Salt Lake City, Utah) approved this study.
Acknowledgments
The authors would also like to recognize the patients who participated in this study; without their support, this project would not have been possible.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: One of the authors (P.C.L.) is a co-inventor on an eccentric ergometer licensed to Eccentron, BTE Technologies, Inc, Hanover, Maryland. Neither P.C.L. nor any of the other authors have received any financial incentives (e.g., reimbursements, fees, royalties, funding, or salary) from the company or stemming from the contents of this manuscript or any related published papers.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by University of Utah Education Resource Development Council.