
Abstract
Background:
Basicervical proximal femoral fracture is a known subtype of extracapsular fracture and is mechanically unstable, especially for the rotational direction, which may lead to implant failure. A cephalomedullary nail (CMN) is widely used for the fixation of unstable extracapsular fracture; however, its application for basicervical fracture remains controversial. Helical blade CMN is proven to have more rotational stability than traditional lag screw implants and potentially advantageous in the treatment of basicervical fracture. The aim of this study is to assess the effectiveness of helical blade CMN for basicervical fracture in elderly patients.
Methods:
We conducted a retrospective review of 500 consecutive extracapsular fracture patients treated surgically between January 2005 and February 2015. Patients who had trochanteric extension or multifragment fracture were excluded. Sixteen cases of 2-part basicervical proximal femoral fracture were identified. All patients were treated with the same single helical blade CMN system (DePuy Synthes PFNA-II). Implant-related complications were recorded.
Results:
Two patients dropped out during follow-up and 14 patients were included in the analysis. The average follow-up period was 21.9 months. No major complication was observed. The patients were subcategorized into 2 groups: nondisplaced (displacement <2 mm at any point of the fracture line) or displaced. Excessive telescoping was observed in 2 patients, both of whom were in the displaced fracture group. The overall implant-related complication rate was 14.2% (2/16).
Conclusion:
Internal fixation with the helical blade CMN system can be considered as a treatment option for 2-part basicervical proximal femoral fracture in elderly patients.
Keywords
Introduction
Implant-related complication is one of the biggest issues in elderly patients with hip fracture. It often leads to reoperation and is associated with increased mortality, increased length of hospital stay, higher rate of failure to return preinjury residence, and higher cost. 1,2 In peritrochanteric fracture, some fracture subtypes, such as complex unstable fracture, reverse oblique fracture, and basicervical fracture, 3 are associated with higher biomechanical complication rate.
For decades, basicervical fracture of the proximal femur had been known as a borderline category between intracapsular and extracapsular fractures. In 1994, Blair et al 4 explicitly described it as a proximal femoral fracture through the base of the femoral neck at its junction with the intertrochanteric region, and it accounts for 1.8% to 3.5% of all hip fractures. 5,6 Basicervical fracture is managed as a subtype of extracapsular intertrochanteric fracture because the blood supply to the femoral head is usually preserved in this type of fracture, and previous clinical and biomechanical studies showed that treatment with multiple cancellous screws, which is a common procedure for internal fixation of intracapsular femoral neck fracture, was associated with higher failure rate than the fixation methods used for extracapsular fracture. 5,7,8 This fracture also has greater rotational instability, which may lead to more mechanical failure than other trochanteric fractures. In general, 2 different methods have been widely used for the treatment of extracapsular fracture: sliding hip screw (SHS) and cephalomedullary nail (CMN). Sliding hip screw has been used as the first-line treatment device for stable trochanteric fracture and yielded good results. Meanwhile, CMN has advantage in the treatment of unstable trochanteric and subtrochanteric fractures 9,10 and became more commonly used regardless of fracture subtype. However, despite the unstable nature of basicervical fracture, the indication of CMN for basicervical fracture remains controversial. Some authors reported good results, 11,12 but others showed higher treatment failure rate. 13
Currently, dozens of CMN systems for trochanteric fracture are commercially available, which have different characteristics. Most CMNs have a lag screw with or without an antirotation screw; however, the lag screw has potential disadvantages in the treatment of basicervical fracture, which has rotational instability. Some studies showed that a single lag screw alone can provide less rotational stability compared with other modern CMN alternatives. 14 Another potential risk is worsening rotational displacement during screw insertion. Proximal femoral nail antirotation (PFNA; DePuy Synthes, Raynham, Massachusetts) is equipped with a helical blade instead of a traditional lag screw (Figure 1). The blade impacts the surrounding cancellous bone without cavity formation while the blade advances into the femoral head fragment, providing better implant anchoring and rotational stability. 15 This system has another advantage because the helical blade is inserted with impacting at the end of the grip handle and thus can be placed without rotational movement of the device. The helical blade CMN system can be a more suitable implant for the treatment of basicervical fracture in elderly patients than traditional lag screw CMNs.

Helical blade of proximal femoral nail antirotation.
In this study, we retrospectively evaluated the clinical outcomes and incidence of implant-related complications in geriatric basicervical fracture patients treated with the single helical blade CMN system.
Methods
We conducted a retrospective radiographic and electronic chart review of 500 consecutive cases of surgically treated extracapsular hip fracture between January 2005 and February 2015 at our institute. Patients who were younger than 60 years at the time of diagnosis, sustained high-energy trauma, or had any suspicion of pathological fracture were excluded. The diagnostic criteria of basicervical fracture involve (1) a 2-part fracture; (2) the proximal fracture line located medial to the intertrochanteric line and did not exceed the midpoint of the intertrochanteric line and the base of the femoral head; and (3) the distal fracture line located along the intertrochanteric line and the lesser trochanter was intact (Figure 2). The diagnosis was made by 2 independent board-certified orthopedic surgeons based on preoperative and postoperative X-ray images. If any disagreement occurred, another orthopedic surgeon made the final decision. Sixteen cases of 500 extracapsular proximal femoral fracture patients met the definition (3.2% of all extracapsular fractures). All those patients were treated surgically with the same single helical blade CMN system (DePuy Synthes PFNA Asian). All patients were allowed weight bearing as tolerated from the first postoperative day.

Radiograph of a basicervical fracture fulfilling the 3 diagnostic criteria. The proximal fracture line is located medial to the intertrochanteric line and does not exceed the midpoint of the intertrochanteric line and the base of the femoral head (arrowhead); the distal fracture line is located along the intertrochanteric line and the lesser trochanter is intact (arrow). The fracture line should be in the shaded area.
Reduction quality was graded as good (<5° varus/valgus and/or anteversion/retroversion), acceptable (5°-10°), or poor (>10°). 16 The blade was directed to the center–center position. To assess blade position, the tip–apex distance (TAD) of all helical blades was measured on the first postoperative X-ray images, as Baumgaertner et al 17 described, replacing the lag screw with the helical blade.
We defined implant-related complications as cut-out/cut-through, nonunion (lack of radiographic healing over 6 months), loosening of the helical blade, hardware-related femoral fracture, any hardware breakage, any movement of the position of the helical blade within the proximal fragment, and “excessive” telescoping/fracture collapse over 10 mm. The first 4 complications (cut-out/cut-through, nonunion, femoral fracture, and hardware breakage) and all complications that required reoperation were classified as “major complications.”
Abiding with our institutional protocol, patients were instructed to visit our outpatient clinic for radiographic follow-up at least every 6 weeks in the first 3 months, then every 3 months for 12 months, once a year after 1 year as far as the patients’ medical condition allows, or more frequently based on the patients’ complaint or discretion of the treating physicians. The minimum follow-up requirement for study inclusion was until confirmation of radiographic and clinical union of fracture by the treating physician. Institutional review board approval was obtained for this study.
Results
Sixteen patients met the criteria of basicervical fracture. No disagreement in diagnosis occurred among evaluating physicians. Two patients, a 107-year-old woman and a 90-year-old woman, dropped out from follow-up before bony union was confirmed because of aggravation of medical comorbidity. Fourteen patients were included in this study. None died before bony fusion. The average follow-up period was 21.9 months (range, 79 days to 70.2 months). All fractures were caused by fall from standing. The average age at diagnosis was 86.9 years (range, 72-90 years). Twelve were women and 2 were men. Six and 8 patients had right and left hip fractures, respectively. We subcategorized the patients into 2 groups: nondisplaced (displacement <2 mm at any point of the fracture line; n = 7) or displaced (n = 7; Figure 3). All but 1 patient could walk before injury (7 patients could walk without any equipment, 4 patients could walk with a cane, and 2 patients could walk with a walker). The physical status was defined using the American Society of Anesthesiologist grading (grade 2, n = 1; grade 3, n = 10; grade 4, n = 3). The patients’ demographics are shown in Table 1.

Representative images of “nondisplaced” and “displaced” fractures. The displacement must be <2 mm at any point of the fracture line in nondisplaced fracture. A, Nondisplaced. No displacement >2 mm is observed along the fracture line (arrowhead). B, Displaced. The radiograph shows >2 mm displacement between fracture lines of fragments. Solid line: fracture line of the proximal fragment; dashed line: fracture line of the distal fragment.
Patient Demographics.
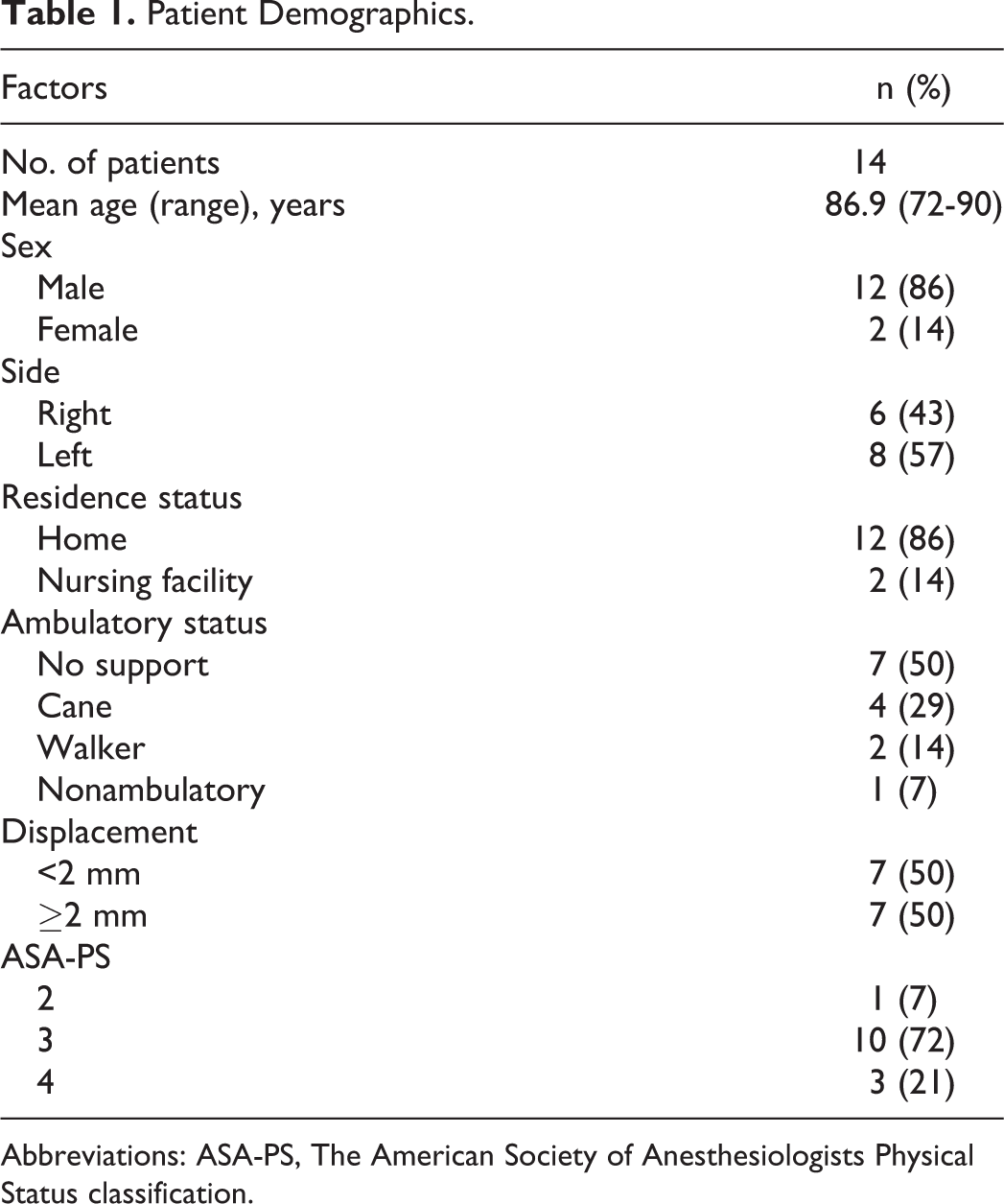
Abbreviations: ASA-PS, The American Society of Anesthesiologists Physical Status classification.
The mean surgical delay was 1.9 days (range, 8 hours to 7 days). The mean operative time defined as time from incision to closure was 23.1 minutes (range, 14-43 minutes), and the mean intraoperative bleeding amount was 39.3 mL (range, 10-120 mL). No intraoperative complication such as loss of reduction, any displacement of the fragments during implant insertion, or intraoperative fracture was observed.
Reduction was achieved using the indirect closed method with fluoroscopy in all 7 patients in the displaced group, with good reduction quality in 6 patients and acceptable reduction (7° anteversion) in 1 patient. The mean TAD of immediate postoperative imaging was 19.2 mm (range, 13.2-29.9 mm); only 1 patient had TAD >25 mm (29.9 mm), which uneventfully healed.
Three patients experienced medical complications (pneumonia, urinary tract infection, delirium) after surgery. Twelve patients regained their preinjury ambulatory status within 3 months, and 13 patients were able to return their preinjury residential status.
Bony union was confirmed in all fractures within 6 months, but excessive telescoping was observed in 2 patients: 11.3 mm in a 65-year-old woman and 12.2 mm in a 90-year-old woman (Figure 4). Both were categorized in the displaced fracture group. One had slight persistent pain possibly due to prominent implant, but the patient was able to walk with a cane and declined implant removal. No cut-out, cut-thorough, or other major implant failure was observed. There was no revision surgery case. The overall implant-related complication rate was 14.2% (2/16). The TADs of collapsed cases were 18.5 and 17.2 mm, respectively, and both were graded as having good reduction on postoperative radiograph.

Radiographic images of a collapsed case (90-year-old woman). A, Preoperative anteroposterior image. B, Postoperative image. C, Image at 6 months postoperatively, showing 12.2 mm of telescoping.
Discussion
Our result showed that the treatment of geriatric basicervical fracture with helical blade CMN was acceptable. There were only 2 cases of relatively minor mechanical complications, and no devastating failure was observed.
Although it varies based on study populations and definition of failure, the overall major implant failure rate of trochanteric fracture is generally around 5% even with any implant, 2% to 10% with SHS, 2% to 12% with lag screw CMN, and 1% to 8% with blade CMN. 3,18 -26 Meanwhile, the implant-related complication rate of basicervical fracture in previous studies showed considerable variations. 3,5 -7,11 -13,27,28 One possible reason is the multiformity of the definition and inclusion criteria of basicervical fracture 5 (Table 2). In the original definition by Blair et al, 4 they did not directly mention whether the fracture was 2-part or not, but their documentation of biomechanical experiments implied that their fracture model was meant to represent a 2-part fracture without trochanteric extension. Patients with multifragment fracture or fracture with trochanteric extensions were included in some studies. These fractures have different biomechanical characteristics compared with the originally described 2-part basicervical fracture model and should be analyzed separately. We set our diagnostic criteria based on the anatomical structure of the synovial capsule to exclude intracapsular fracture 29 and on feasibility in clinical setting. No disagreement occurred about the diagnosis using our criteria. Although the reliability should be evaluated, we believe our criteria are feasible in identifying a “true” basicervical fracture in the clinical setting.
Definitions of Basicervical Fracture in Previous Studies Since Blair’s Report.

Abbreviations: AO/OTA, Arbeitsgemeinschaft für osteosynthesefragen/Orthopaedic Trauma Association classification; N/A, not applicable.
The treatment results of previous studies are shown in Table 3. Although the number of comparable studies is limited, some authors reported the outcome of basicervical fracture with strict inclusion criteria, excluding multifragment fracture and trochanteric extension. Mallick and Parker 7 reported a good outcome of surgically treated basicervical fracture with SHS, with only 1 of 79 patients showing cut-out. They concluded that osteosynthesis with SHS can be recommended and they emphasized correct reduction and lag screw positioning. Although we agree with their opinion regarding the importance of reduction and screw positioning, we question the applicability of their result to patients with osteoporotic low-energy basicervical fracture such as our study population. Although the mean age of their study population was similar to our study (79.7 years), the patients’ age ranged from 28 to 96 years and 4 nonoperative and 6 arthroplasty (hemiarthroplasty or total hip replacement) cases were included in the calculation of mean age. 7 We believe their excellent result with SHS might have been due to the younger age in the osteosynthesis group because old patients might have been more likely allocated to the nonoperative or arthroplasty group. Watson et al 13 reported a very high failure rate with CMN for basicervical fracture, with 6 (54.5%) of 11 cases having a major complication, such as nonunion, requiring revision surgery or cut-out, even with acceptable screw positioning, and the authors concluded that basicervical fracture may be treated better with an SHS and plate device rather than CMN. Their study population and definition of basicervical fracture were similar to our study, but the outcome was different. Regarding the cause of the failure, they proposed a hypothesis that the nail acted like an intramedullary buttress, preventing further collapse, and this led to nonunion or rotational and angular failure. In our study, the 2 collapsed case showed that the cortex of the femoral neck seemed to contact the nail eventually, but cut-out did not occur. We believe the result of Watson et al 13 cannot be applied to all CMN systems, and the failure in their study was more likely to have been caused by an implant-specific problem of the nail they used or a technical issue. To prevent fracture collapse, we believe anatomical reduction is the key, as many surgeons mentioned. Among the strictly defined 2-part fractures, telescoping would not occur if anatomical contact of the fracture line is obtained. During surgery, it is sometimes difficult to evaluate the reduction of rotational displacement in basicervical fracture with image intensifier because of the symmetrical figure of the fracture line. Both of our collapsed cases were in the displaced group. There might have been some residual rotational displacement in these cases and the acceptable margin for malreduction may be very small in basicervical fracture, even if it is a 2-part fracture, due to its unstable nature.
Outcomes of Previous Studies.

Abbreviations: CMN, cephalomedullary nail; N/A, not applicable; PFNA, proximal femoral nail antirotation; SHS, sliding hip screw; THA, total hip arthroplasty.
In this study, we used helical blade CMN system (PFNA II). Biomechanical studies showed that the helical blade had higher rotational stability compared with lag screws. 15,30 -32 In clinical studies of extracapsular fracture in general, treatment with helical blade CMN and lag screw CMN showed similar results and no superiority of the helical blade to lag screw systems has been confirmed. However, according to our result, the helical blade might be advantageous for this selected subgroup because of its better antirotation effect.
The TAD was first described by Baumgaertner et al, 17 and they found that patients with TAD >25 mm were more likely to have cut-out. Although the fixation device they used was SHS, the TAD has been applied for almost all devices including CMNs, and in our study, the case with TAD >25 mm (29.9 mm) uneventfully healed. In their biomechanical study, Lenich et al 31 reported that a center–center position in the femoral head was the recommended optimal position of the blade to minimize rotation and prevent failure in the helical blade. Nikoloski et al 33 reported that the TAD in PFNA-treated patients with cut-out showed a bimodal distribution, with TAD >30 mm and TAD <20 mm. They concluded that the helical blade should not be placed too close to the subchondral bone. Furthermore, cut-through or central migration of the helical blade was reported as a notable complication of PFNA. 34,35 Although the pathophysiology of cut-through has not been fully understood, placing a blade too close to the joint would also be a risk factor for this complication. Considering all these information, we recommend that a helical blade should be placed at the center–center position in the femoral head and 10 to 12.5 mm from the subchondral bone.
The cost of the helical blade CMN we used was similar to the average cost of currently available CMNs, but approximately 3 times as high as SHS. 36 Osteoporotic hip fracture patients with revision surgery due to fixation failure were reported to have approximately 2-fold higher total cost than those who had no fixation failure. 2 Swart et al 37 also mentioned that CMN would be a clinically better and more cost-effective implant if the incremental failure rate of SHS exceeds 5%. Considering the high failure rate of basicervical fracture treated with conventional implants, cost reduction by lowering the complication rate may outweigh the higher implant cost.
Our study has several limitations. First and most important, the study has a small sample size. This is partly due to our strict inclusion criteria. Second, this is a single-center retrospective study with no control group. Third, our study population included only East Asians, who tend to have smaller body habitus, which may affect the mechanical complication rate after internal fixation. Finally, 2 of 16 cases dropped out from follow-up. We believe further prospective randomized multicenter studies with sufficient sample size directly comparing helical blade CMN and other devices are needed to determine the best treatment for basicervical fracture; however, a uniform definition of the fracture should be strictly used to reach an agreeable conclusion.
Conclusion
Our study showed good treatment outcome with the helical blade CMN system for 2-part basicervical proximal femoral fracture in elderly patients. We believe the helical blade CMN should be considered as an option for the treatment of this highly unstable fracture subtype.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.