
Abstract
Purpose:
The aim of this study was to ascertain trends in the incidence of hip fracture in southeastern Norway by comparing the hip fracture incidence for the years 2008 to 2010 to that of a study from 1998 to 2003 in the same area.
Methods:
We determined the number of hip fractures for the geographical area of Ostfold county, and the age- and gender-specific incidence per 100 000, with 95% confidence intervals, was calculated. Use of bisphosphonates was determined by extracting data from public databases.
Results:
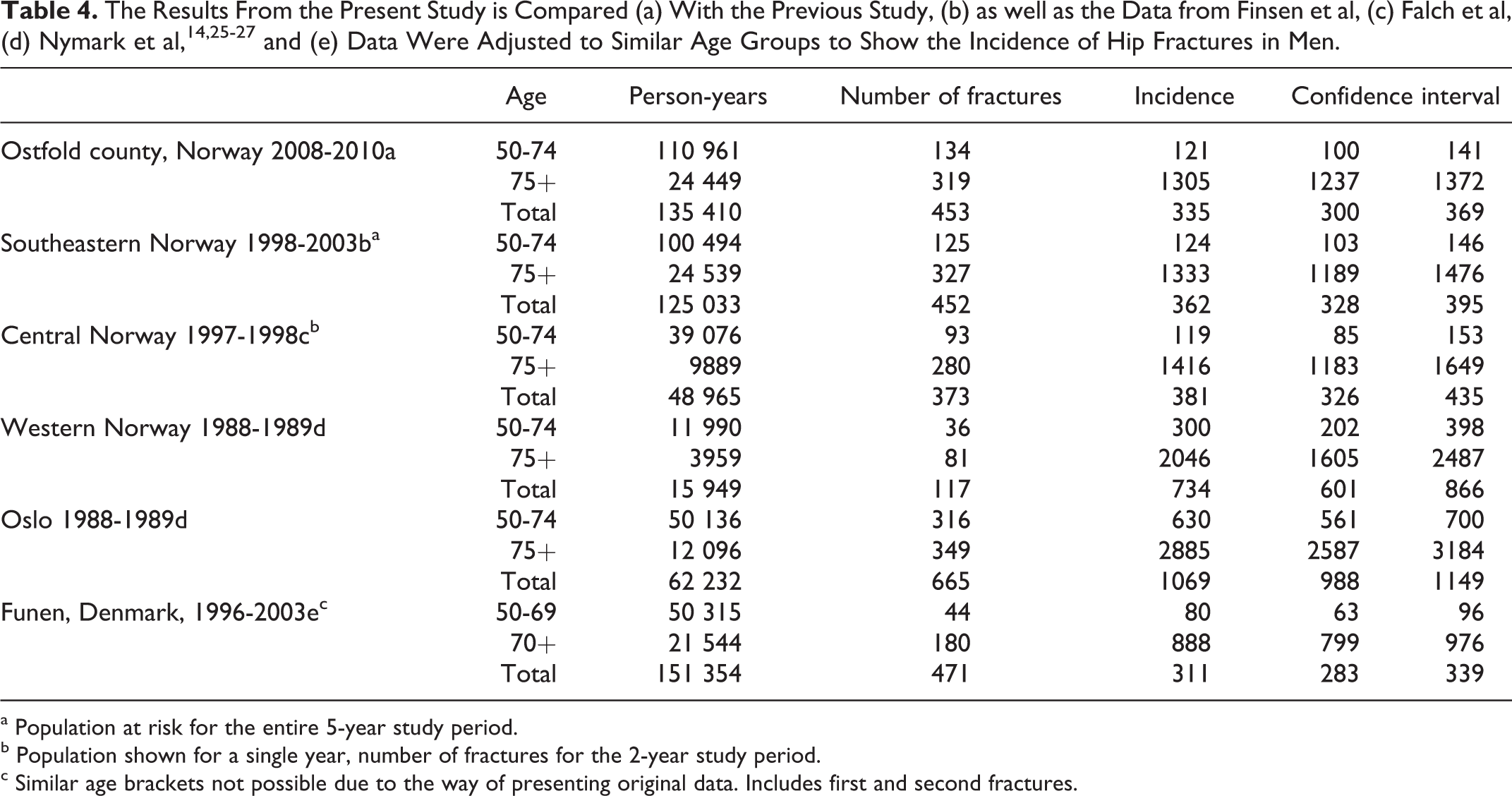
The hip fracture incidence for men aged 50 to 74 and older than 75 years was 120 (100-141) and 1305 (1237-1372) in the latest time period, 1998-2003, whereas the incidence for the previous period, 2008-2010, was 124 (103-146) for men aged 50 to 75 and 1333 (1189-1476) for men older than 75 years. For women of 50 to 74 years, the incidence was 184 (158-209), and for women older than 75 years, it was 2523 (2428-2618). In the first time period, the corresponding incidence was 228 (200-257) for women aged 50 to 74 and 2330 (2189-2471) for women older than 75 years. As the 95% confidence intervals overlap in all the comparisons, it indicates the the incidence did not significantly differ between the time periods. Bisphosphonate use did not exceed 2% in any age group for men. For women, the highest rate of bisphosphonate use was 12.6% in the 85- to 89-year groups.
Conclusion:
We cannot confirm reports of decreasing incidence of hip fracture
Introduction
The incidence of hip fracture has been determined in multiple studies, and while some recent reports suggest a decrease, 1 –7 others report an unchanged or increased incidence. 8 –12 In a recent study, Norway was found to have the third highest incidence of hip fracture in the world, 13 which makes it interesting to follow the incidence of hip fracture in this country. We have previously determined that the incidence of hip fracture in southeastern Norway in 1998 to 2003 was comparable to that in other Scandinavian countries 14 in a study encompassing 100 000 people from 6 municipalities treated at 1 hospital. This hospital subsequently enlarged its catchment area to 270 000 inhabitants by including 12 more municipalities. The new and larger population is similar in demographic composition and provides an opportunity to study hip fractures in a larger population, yielding more reliable results.
Several factors, such as changing demographics, activity modification, and medical treatment, may cause changes in the incidence. In this study, we determined the age- and gender-specific incidence of hip fracture in a well-defined population in Norway and compared the findings to those in the previous study in the same geographic area and also investigated bisphosphonate use in the same time period.
Methods
In this study, we included all patients who were treated at our institution from January 2008 to December 2010. Our institution is the sole provider of hip fracture care for the Ostfold county which is comprised of 18 municipalities and a population of 270 000 people.
We included patients aged 40 years and older with a fracture of the proximal femur, including subtrochanteric fractures. Using the electronic patient record search engine, we obtained the records of all patients discharged under the diagnosis of the International Classification of Diseases, Tenth Revision (ICD-10) subcategory S72-fracture of the femur. The records were then individually evaluated, and all fractures not pertaining to this study were excluded. We then analyzed the operative notes to validate the injury classification, and radiographs were examined in cases where notes were inconclusive. We excluded patients residing outside our area as well as patients with periprosthetic or pathologic fracture. Isolated fractures of the greater trochanter were also excluded. The fractures were subclassified as intracapsular or extracapsular fractures, and lateral cervical fractures were classified as extracapsular fractures since these fractures most often were treated with intramedullary nailing. Three patients with both intracapsular and extracapsular fractures in the same hip were classified as intracapsular fractures. Patients with previous contralateral hip fractures were included, and patients who sustained 2 fractures during the study period were counted as such.
The incidence was then calculated by dividing the number of fractures in each age bracket for each gender by the number of persons at risk and multiplied by 100,000. In order to estimate the degree of uncertainty, we calculated the 95% confidence interval for the age- and gender-specific incidence. 15
Population data were obtained from the Statistics Norway Web pages 16 and bisphosphonate prescription data for the county population were extracted from the Norwegian Prescription Database at the Norwegian Institute of Public Health. 17 The data were aggregated for 2008 to 2010 in order to comply with the fracture data and presented as users as a percentage of the population at risk including confidence intervals for ease of comparison with other studies. When the confidence intervals of 2 estimates do not overlap, this finding indicated that there was a statistically significant difference between the estimates. 15
We then compared the data from the current study to that from a previous study in order to detect significant changes in the incidence as evidenced by nonoverlapping confidence intervals. Lastly, we calculated the proportion of intracapsular and extracapsular fractures.
The research was conducted in accordance with the principles of the Helsinki declaration, and the study was approved by the Hospital Research board and financed by the Department of Orthopedic Surgery. Since no data on individual patients were collected, informed consent was not necessary.
Results
A total of 1,673 fractures occurred during the 3-year study period, of which 460 occurred in men and 1213 in women. The incidence for men aged 50 to 74 and older than 75 years was 120 (100-141) and 1305 (1237-1372) fractures, respectively, per 100 000 persons per year. For women of 50 to 74 years, the incidence was 184 (158-209) fractures per 100 000 persons per year, and for women older than 75 years, it was 2523 (2428-2618). The incidence increased exponentially after the age of 65 to 69 for men and 60 to 64 for women, and there is a significant difference in the incidence between men and women after the age of 70 to 74 (Figure 1). The number of fractures in each age bracket and incidence per 100 000 per year is shown in Table 1.

The incidence of hip fracture rises exponentially in men and women.
Number of Fractures and Population at Risk With Incidence Rate Per 100 000 Persons and 95% CI for Each Gender and Age Group.

Abbreviations: CI, confidence interval; T, trochanteric; I, intracapsular.
Bisphosphonate use is presented in Table 2. For men, bisphosphonate use was generally low, not exceeding 2% in any age group. For women, the highest rates of bisphosphonate use were found in the age groups between 75 and 89 years, reaching 12.6% in the 85- to 89-year groups. There were no significant differences in hip fracture incidence between the previous study and the present study (Tables 3 and 4).
Percentage of Bisphosphonate Users as Well as Persons at Risk and Users in 2008 to 2010, Including 95% Confidence Intervals.

Abbreviation: CI, confidence interval.

a Population at risk for the entire 5-year study period.
b Population shown for a single year, number of fractures for the 2-year study period.
c Similar age brackets not possible due to the way the original data were presented. Includes first and second fractures 1996-1999 and 2000-2003.
a Population at risk for the entire 5-year study period.
b Population shown for a single year, number of fractures for the 2-year study period.
c Similar age brackets not possible due to the way of presenting original data. Includes first and second fractures.
The proportion of trochanteric fractures was 37% in men and 42% in women, and this proportion remained unaltered when calculating the proportions in the age groups with the highest incidence of hip fracture.
Discussion
Although the number of hip fractures that occur annually is expected to rise as the number of old people increases, no consensus is established as to whether the age- and gender-adjusted incidence of hip fracture will increase. Reports from several countries indicate that the incidence might be declining, 21,2 but this trend is not universal. 3 In a report from Denmark, Abrahamsen and Vestergaard claim that the incidence of hip fracture is declining. 6 The authors found a 20% decline in hip fracture incidence in Denmark from 1997 to 2006, which was partly explained by use of bisphosphonates and partly due to other reasons. Also, Kannus et al have reported a nationwide decline in hip fracture rates in Finland since 1997, 22 without being able to pinpoint 1 single cause for the decline. The role of bisphosphonates was considered unlikely by these authors 23 because of the low prevalence of these drugs in the late 1990s. On the other hand, in a report from Sweden in which the prevalence of osteoporosis and incidence of hip fracture were compared in 3 populations from 1970 to 1974, 1987 to 1993, and 1998 to 1999, the authors found a steady increase in the incidence of hip fracture but no difference in the incidence of osteoporosis, 24 which is confusing since osteoporosis is considered a prime cause of hip fracture. In our study of a Norwegian population in 1998 to 2003, we did not find significant differences from the other Scandinavian countries or trends toward lower incidence compared to previous Norwegian studies. 14 Although the relationship between hip fracture and osteoporosis is complicated, the use of bisphosphonate drugs by the population may influence the incidence of hip fracture through modulation of the incidence of osteoporosis. In this study, we found that the percentage of the population who uses bisphosphonates is comparable to that in the Danish study. The Danish study period (1997-2006) preceded ours, which precludes direct comparisons, but at no time did Danish use of antiosteoporotic drugs exceed the use in our population in any of the age groups studied. This may indicate that we might see a decline in the incidence of hip fracture later than in Denmark, but it may also imply that different mechanisms are at play in the 2 countries.
A recent study that was conducted in southern Norway in the period between our first study and the present study found hip fracture incidence rates equivalent to ours, which supports the notion that hip fracture rates are stable in Norway. 11 In a recent report from northern Norway, hip fracture rates were found to be stable over the last 15 years, and these authors found an unexplained lower rate of hip fractures in female patients. However, in this report, the annual incidence was low, the total number of fractures being only 604 over a 15-year period, which make the estimates vulnerable to natural fluctuations. 12
In Australia, a clear relationship was found between prescription rates of bisphosphonates and incidence of hip fracture although the authors concede that many unknown factors may also influence the fluctuations in hip fracture rates. 25
Unfortunately, we do not have complete and detailed information about the use of antiresorptive drugs in our population prior to the current study period. However, the drugs have been prevalent since the late 1990s and readily available once a diagnosis of osteoporosis was made. Our finding of no obvious decline in the incidence of hip fracture does not indicate that these drugs have been effective in reducing the incidence of hip fracture, although one might argue that incidence might have been even higher without the use of antiosteoporotic medication.
The strengths of this study include a rigorous search algorithm, which ensured that all fractures that were treated at our hospital were included in the study and the ability to compare the present findings to that in our previous study. Since the catchment area of the hospital was enlarged between the study periods, we were able to include approximately the same number of fractures in a 3-year study period as we included in a 5-year study period in the first study. The study periods are separated by 5 years, which means that the 2 periods span 12 years, during which we have not seen any change in the incidence of hip fracture.
The weakness of the study relates to the fact that we did not have complete control of fractures sustained and treated outside the Ostfold county by inhabitants of the county. However, this number is thought to be very small and not likely to affect the conclusion. Also, we have not addressed the question of first versus second hip fracture. At the start of the study period, a certain number of patients were likely to have sustained a hip fracture on 1 side. Although it is known that this increases the likelihood of sustaining another fracture, this also reduces the pool of hips at risk in the population. Moreover, the prevalence of patients with 2 previously fractured hips is not accounted for. Furthermore, the prevalence of hip arthroplasty is unknown and could thus not be accounted for, which is unfortunate as this obviously also reduces the number of persons at risk. However, these factors are very hard to control and adjust for and it is unknown to which extent they could influence the main findings in the study, but all these factors would decrease the patient pool at risk and thus our estimates may be regarded as too low.
In conclusion, this study does not confirm the other reports that the age- and gender-specific incidence of hip fracture in Norway is changing.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.