
Abstract
In posterior spinal fusion (PSF), the vertebral artery is most vulnerable to injury at C1-2. C2 pedicle screws are often placed into the dorsomedial isthmus of C2. Alternative techniques include C2 laminar screws and wiring techniques. A 67-year-old male underwent PSF for persistent severe intractable neck pain and degeneration at C1-2. The patient had an enlarged left vertebral artery with midline migration into the C2 body. This pattern was within one standard deviation of normal; however, it rendered typical placement of a C2 pedicle screw unsafe. As a salvage, a C2 laminar screw was placed on the left to avoid risk of vertebral artery injury. The operation and recovery were without complication. C2 laminar screws can be viable alternatives to C2 pedicle screws in cases of midline vertebral artery migration or other vascular anomalies preventing normal safe placement of C2 pedicle screws.
Keywords
Introduction
Failure to recognize an anomalous vertebral artery (VA) can lead to iatrogenic vertebral artery injury (VAI) and cerebrovascular accidents. 1 The incidence of VAI in degenerative cervical spine surgery is up to 1.96% and is likely underreported. 2 A review of the etiology of iatrogenic VAI found three main causes: off-midline use of high-speed burr, excessive width of bone or disc removal, and pathological softening of lateral bone of the spinal canal. 3 From a posterior approach, the VA is most vulnerable to injury at C1-2; from an anterior approach, it is most at risk at C7. 3 Therefore, a thorough appreciation for the variations in the course of the VA is vital for surgeons working from a posterior approach in the upper cervical spine.
Case Report
The patient is a 67-year-old man who presented with the complaint of a multiyear history of persistent severe neck pain with rotation. Incidentally, he had previously undergone an anterior cervical discectomy with fusion at C5-6 and C6-7.
Plain radiographs demonstrated severe multilevel cervical degeneration. He had near-ankylosis of the C1 ring to the dens anteriorly in addition to severe articular facet degeneration. A computed tomography (CT) scan was obtained, which also demonstrated severe degenerative disease as well as an anomalous course of the left VA (Figure 1A and B). Magnetic resonance angiogram (MRA) was also reviewed to further characterize the course of the left VA (Figure 1C). At C2, he had a markedly enlarged left transverse foramen due to a larger left VA. The enlarged foramen extended medially into the path through which a C2 pedicle screw would be inserted. Both the diameter of the left VA and the distance from the left VA to midline were measured by a fellowship-trained neuroradiologist.
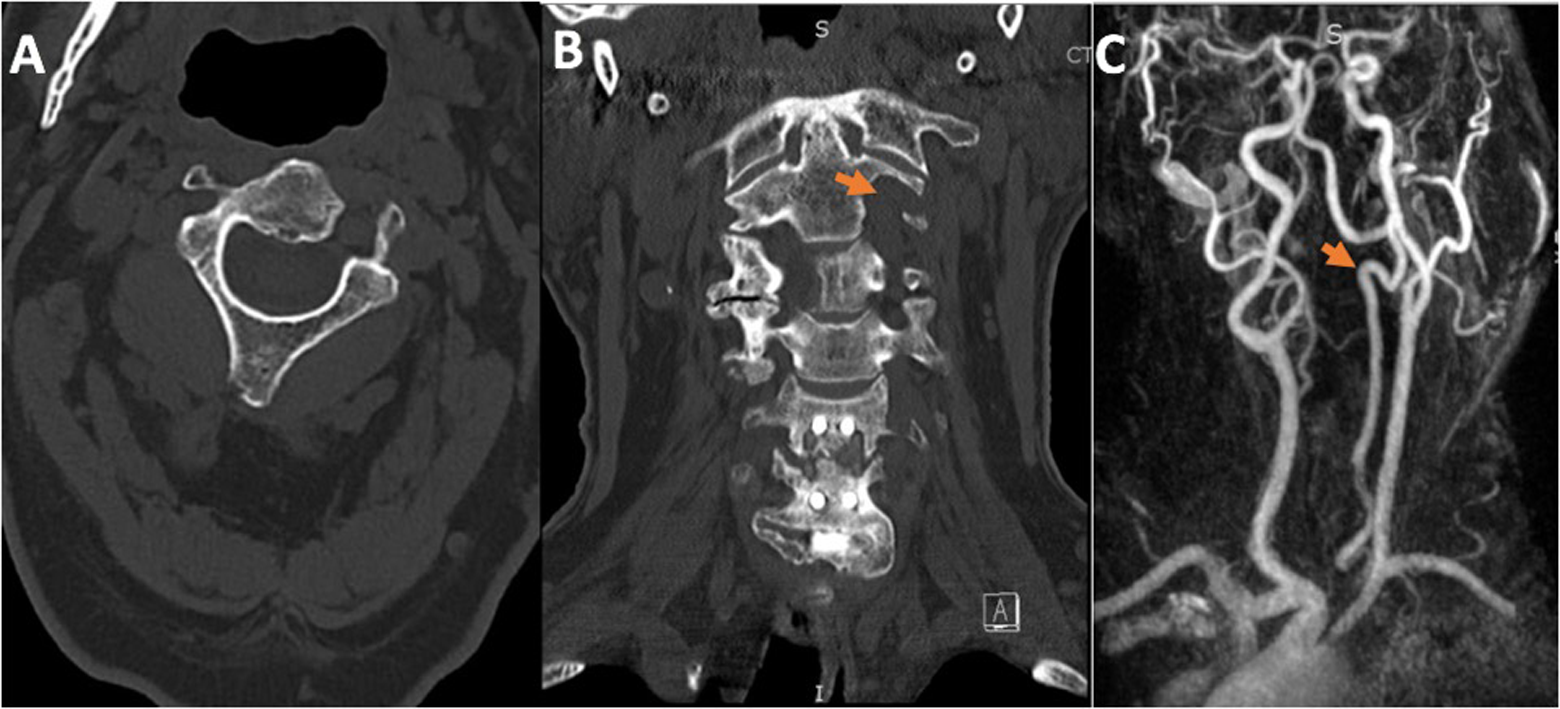
A, Preoperative axial noncontrast CT scan showing C2 and the left vertebral artery coursing through the vertebral body. B, Coronal CT with left vertebral artery shown moving medially then turning laterally before coursing cephalad. C, MRA with arrow indicating left vertebral artery at level of C2; the arrow is at the same position in the coronal CT.
He had complete relief of his rotational pain with fluoroscopically guided C1-2 injections administered by an interventional radiologist. After failure to improve with exhaustive nonsurgical interventions and treatments, we discussed the potential risks and benefits and he elected to proceed with instrumented posterior spinal fusion (PSF) at C1-2.
Our initial plan was to perform an instrumented PSF at C1-2 using the Harms technique with pedicle screws at C2 and lateral mass screws at C1. On review of the CT, we were concerned that placement of a left C2 screw was precluded by the enlarged transverse foramen. He had had an MRA 4 years prior. This study also demonstrated the course and size of the left VA.
After induction of a total intravenous anesthetic technique, with the use of neurologic monitoring services intraoperatively, patient was placed in a Mayfield head holder and positioned prone on a Jackson table with his bony prominences padded. The posterior cervical spine was prepared and draped in a sterile fashion. A longitudinal midline approach was carried out, exposing out to the lateral mass of C1 and the facets of C2. The C1 roots were retracted inferiorly once hemostasis was obtained. The C1 roots were not sacrificed. A drill hole was made in the lateral mass of C1, and a 26-mm partially threaded screw was placed on each side without difficulty.
The C2 level on the right side had normal anatomy, and a 26-mm fully threaded C2 pedicle screw was placed uneventfully using Harms technique and position was acceptable, 4 verified with anteroposterior (AP) and lateral fluoroscopic X-ray.
On the left side at C2, because of the course of the left VA in the enlarged transverse foramen, standard placement of a C2 pedicle screw was precluded (Figure 2). Standard Harms positioning of a C2 pedicle screw would have placed the VA at a high risk for perforation with the potential for a posterior fossa infarct. Decision was made to proceed with a C2 laminar screw, as first described by Wright. 5 The high-speed burr was used to open the dorsum of the lamina on the left-hand side. The gearshift probe was placed down, heading at an angle of approximately 45° to 50° from left to right, and a 30-mm screw was placed. Of note, there are male/female variations in screw length, and a more typical length would be 20 to 25 mm. 6 Acceptable position was verified with AP and lateral fluoroscopic X-ray (Figure 3). Rods of appropriate length were used to connect the screws. The C1-2 articular facet was then packed with morselized local bone graft. Irrigation was completed, and hemostasis was obtained, and the wound was closed primarily in layers. Postoperatively, the patient underwent standard treatment and pain management protocols and had a stable recovery as determined by the 6-month postoperative follow-up visit. Postoperative CT reading indicated anatomical position with no periprosthetic lucency or signs of hardware failure for the right C1-2 and left C1 pedicle screw as well as the left C2 laminar screw. There was no neurological change or injury.

Artist renditions. A, Axial view of C2 shows an enlarged transverse foramen and vertebral artery on the left side, directly in the path of a typical C2 pedicle screw. A laminar screw was placed in lieu of a pedicle screw on the affected side. B, Coronal view of C1-3 shows the tortuous path of the left vertebral artery as it migrates medially toward the lateral aspect of the dens before turning laterally and inferiorly. Note the left vertebral artery is larger in diameter than the right vertebral artery.

A and B, Intraoperative X-ray fluoroscopy images indicating location of screws. B, Previous C5-7 anterior cervical discectomy and fusion (ACDF) visible.
Discussion
A recent retrospective study of 1054 patients who underwent anterior cervical spine surgery found a 1% incidence of midline migration of the VA into the uncovertebral joint between C3 and C7. 7 Half of these cases included aberrant migration of the VA into the vertebral body—though none of these migrations were above the level of C3-4. 7 In one case study, a patient had a tortuous left VA that migrated into the C6 body. The proposed theory behind midline migration was that degenerative osteoarthritis of the cervical spine allowed the VA to develop a more tortuous path over time and erode into the posterolateral vertebral body. 8 A retrospective study of 387 patients using three-dimensional CT angiography found the following incidences of VA anomalies at C1-2: high-riding VA (10.1%), persistent first intersegmental artery (1.8%), fenestration of the VA above and below C1 (1.3%), and the posterior inferior cerebellar artery arising from C1-2 (1.3%). 9
Measurements were compared to corresponding results from a study of 250 MRIs of patients at the level of C2 (Table 1). 10 The left vertebral artery diameter (VAD) was 4.9 mm, whereas the right VAD was 3.3 mm, compared to a reported left VAD of 3.95 (0.76) mm (mean [standard deviation]) and a right VAD of 3.74 (0.79) mm (mean [standard deviation]). The left VAD was within 1.5 standard deviations of the reported mean diameter at C2. The left vertebral artery to midline distance (VAMD) was 10.1 mm compared to a reported left VAMD of 12.63 (4.50) mm (mean [standard deviation]). However, the right VAMD was 15.4 mm compared to a reported right VAMD of 14.43 (1.90) mm (mean [standard deviation]). Interestingly, both the left and right VAMD were within one standard deviation of the reported mean distance at C2. These measurements indicate that similar anomalies are more common than previously thought and warrant additional consideration during the preoperative planning phase.
Patient VA Measurements Compared to Population Data.
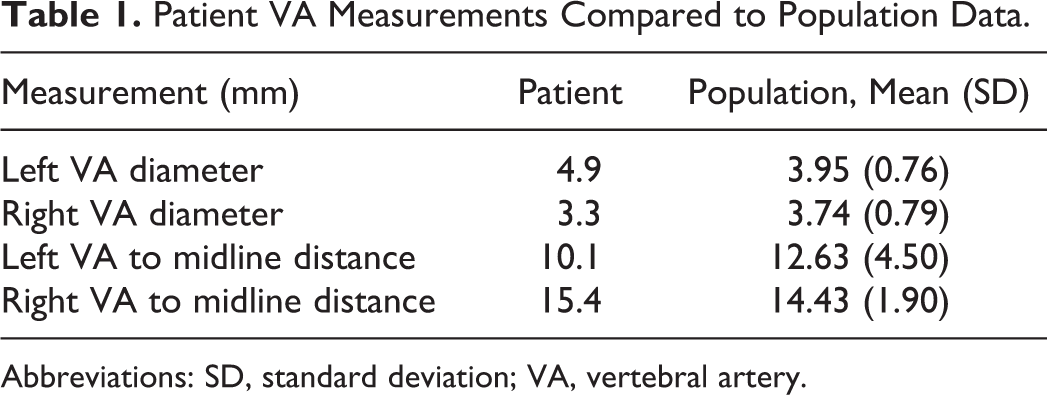
Abbreviations: SD, standard deviation; VA, vertebral artery.
If a C2 pedicle screw was placed on the left side of this patient in accordance with standard procedure for patients with normal anatomy, VAI and complications such as cerebellar and posterior cerebral artery infarcts may have occurred. The left VA was dominant in this patient, providing the majority of the blood supply to the basilar artery and posterior fossa. A left VAI would likely have been more detrimental than right VAI in this patient, potentially leading to the need for urgent neurosurgical intervention. With these considerations in mind, use of a C2 laminar screw on the affected side was implemented successfully without complication.
Since the normal course of the VA is to bend under the superior articular facet of C2, and this bending point has been shown to have individual variation, the safest recommended placement for transarticular screws was reported to be into the dorsal and medial section of the isthmus of C2. 11 -13 Transarticular screws provide adequate fixation for C1-2, but limitations include the possibility of requiring more caudal exposure to find appropriate screw trajectory—necessitating reducibility of C1-2 joints and posing increased risk of VAI in cases of aberrant anatomy. 14,15 An alternative technique, posterior C2 laminar screw fixation poses less risk to the VA in patients with a unilateral dominant VA communicating with the basilar artery. 16 C2 laminar screws have been shown to have biomechanically equivalency in terms of pullout strength in comparison to C2 pedicle screws. 17 In addition, the use of C2 pedicle screws and C2 laminar screws has both been shown to be safe and effective treatments for cervical instability. 18 In a biomechanical evaluation, wire pullout strength was comparable between unicortical and bicortical screws. 19 Another study found that pullout strength was not significantly different between bilateral C2 pedicle screws and a construct with a unilateral C2 pedicle screw and a contralateral C2 pars screw. 20
Other well-established techniques are also available to provide stabilization, which may be considered in cases of anomalous vascular anatomy. These include pin-based halo immobilization, sublaminar cerclage wires, or alternative screw patterns. Supplemental cervical stabilization at the C0-2 junction can be provided by halo vests. 21 Halo fixation, while useful in some cases, was not performed in this case due to decreased rigidity in immobilizing the cervical spine, numerous complications, and poor outcomes in the elderly. 22 -25 Improved stability in instrumentation has significantly decreased the need for postoperative halo vests. 14 Use of sublaminar cerclage wires and structural iliac autograft in C1-2 fixation have the advantage of utilizing inexpensive and readily available equipment. However, this technique requires intact laminae, poses some limited risk of spinal cord injury though rare, and is associated with reduced stability in axial rotation and lateral bending with subsequent higher reported rates of pseudarthrosis in some comparisons with screw and rod-based constructs. 14,26,27
A recent case study of pediatric subaxial cervical spine fusion, in which lateral mass fracture occurred during screw placement, found that the use of a hybrid sublaminar wire-lateral mass screw construct as a salvage technique provided stable fixation with bony fixation. 28 In cases of anomalous vertebral anatomy with more technically challenging screw placement, if intraoperative fracture occurs, then the use of a modified sublaminar wire-lateral mass screw construct may be considered. Constructs can also be extended proximally to the occiput in occipitocervical fusion. 29 However, this is a morbid and disabling procedure and use is subsequently limited to severe injury to the craniocervical junction, malignancy, or when no or limited procedural plan is viable. 30 -32
Another consideration is the use of a unilateral pedicle screw at C2 contralateral to the anomalous anatomy. This would decrease the risk of VAI on the affected side, and a case series of 12 patients who underwent C1 lateral mass screw–C2 unilateral laminar and contralateral pedicle screw fixation found this technique to be safe and effective. 33 Further long-term comparative studies are warranted to provide increased clinical evidence for instrumentation techniques in posterior cervical fusion in cases of VA anomalies.
Here, we presented a case of upper cervical fixation in a patient with an anomalous left VA course. Preoperative evaluation identified enlargement of the left VA along with midline migration into the body of C2. Angiography is indicated when concerned about VA anomaly. Posterior fixation with ipsilateral mass screw to laminar screw on the affected side was a viable safe technique. Thorough preoperative evaluation and surgeon familiarity with salvage techniques are required for care of these complex cases.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.