
Abstract
Introduction:
Total knee arthroplasty (TKA) is an effective treatment for knee osteoarthritis. Patient-reported outcome after TKA is influenced by multiple patient-related factors. The aim of this study was to prospectively evaluate preoperative patient-related factors and to compare the self-reported outcomes 1 year after TKA among groups differing by age, sex, body mass index (BMI), education, and social support level.
Methods:
314 patients, who underwent TKA in Vilnius Republican University Hospital between the end of 2012 and the middle of 2014, were included in a study. The preoperative and 12-month follow-up measurements were obtained using Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and Short Form-12 (SF-12). Differences between patient groups according to gender, age, BMI, level of education, and level of social support were analyzed.
Results:
At 12-month follow-up men demonstrated better results than women in WOMAC (P = .003) and SF-12 both domains (P < .05). Patients with a higher social support demonstrated higher scores in physical function according to SF-12 (P = .008). Better preoperative WOMAC and SF-12 scores were a predictor of better outcome 1 year after surgery. There was no difference in postoperative scores in different age, BMI, and education groups according to WOMAC and SF-12.
Conclusion:
There is no difference in self-reported functional outcome between patient groups differing in age, BMI, and education. Men and socially supported patients demonstrate better postoperative functional results 12 months after TKA. Better preoperative knee function and overall physical and mental function are predictors of better outcome 1 year after TKA. Age and obesity should not be limiting factors when considering who should receive this surgery.
Keywords
Introduction
Osteoarthritis (OA) is one of the most common diseases affecting the musculoskeletal system in elderly people and has a substantial impact on patient’s quality of life. 1 A primary total knee arthroplasty (TKA) is an effective treatment for an end-stage knee OA. 2,3 Total knee arthroplasty provides a long-lasting joint that relieves pain and improves patient’s physical function. 4 Since the introduction of modern TKA in 1970s, the surgical techniques, the instrumentation, and the implant technologies have changed dramatically and those improvements greatly benefited to postoperative outcomes. However, a significant patient population (10%-20%) is still experiencing unsatisfactory results regardless of technological advancements. 5 Therefore, a traditional indicator of surgical success, such as implant survival, may not mirror the patient’s postoperative experience, which these days are assessed with patient-reported outcome measures (PROMs). 6 The PROMs have become a cornerstone of outcome assessment after joint surgery. 7 Numerous PROMs are used to measure the outcome. Western Ontario and McMaster Universities Arthritis Index (WOMAC) and the Short Form-12 (SF-12) are the most commonly used. The WOMAC is a joint-specific instrument for measuring clinical outcome in patients treated for knee OA. 8 The SF-12 score is a generic health measure of patient’s overall physical and mental well-being. 9
Various patient-related factors can be associated with poor outcome after TKA, including, age, gender, obesity, education, and social support level. 6,10 -13 It’s important to identify those preoperative risk factors in order to understand why some people fail to benefit from TKA.
The aim of this study was to prospectively evaluate preoperative patient-related factors and to compare the self-reported outcomes 1 year after TKA between groups differing by age, sex, body mass index (BMI), education, and social support level.
Materials and Methods
The data presented in this article is from single center in Republican Vilnius University Hospital in Lithuania. 314 patients who underwent TKA between the end of 2012 and the middle of 2014 were involved in a prospective study. Patients included in the study met the following criteria—They had knee OA, were scheduled to undergo primary TKA, spoke native language, and agreed to participate in the study. A written consent was obtained and no monetary compensation was provided to study participants. Ethical approval was obtained from Lithuanian Committee of Bioethics.
The baseline measurements were obtained the day before surgery and postoperative follow-up 12 months after surgery. Sociodemographic information was obtained from questionnaire administered to participants at the day of their preoperative evaluation. Questionnaire included sex, age, education, social support, height, and weight (from which BMI was calculated). Patient’s education was coded as either lower (secondary school or vocational training) or higher (University). Social support was determined by their marital and living status (lived alone or with somebody). Two validated and originally authorized Lithuanian translations of questionnaires were used—WOMAC and SF-12.
The WOMAC is a disease-specific instrument with 3 dimensions that measure pain, joint stiffness, and physical function. It consists of 24 items (5 for pain, 2 for stiffness, and 17 for function). Point values from 0 to 4 are assigned to each response and scores are totaled for each category. The maximum score is 20 points for pain, 8 for stiffness, and 68 points for physical function. Higher scores indicate greater difficulty [16]-[18].
The SF-12 score is a generic health measure of a patient’s overall physical and mental well-being. Physical health composite score (PCS) and mental health composite score (MCS) are calculated using the scores of 12 questions and range from 0 to 100, where a 0 score indicates the lowest level and 100 indicates the highest level of health. 4
Statistical Analysis
The independent variables were age, sex, BMI (<30.0, 30.0-34.9, 35.0-39.9, ≥40.0), level of education (lower and higher), and social support (married/living with someone and otherwise). The effect of each independent variable was analyzed separately for WOMAC and SF-12. For statistical analysis, we used SPSS V20.0 and “The R project for statistical computing” version 3.2.2. To compare 2 parametric groups, we used Student t test, for multiple comparisons—analysis of variance, with Bonferonni post hoc test and to compare nonparametric groups we used Mann-Whitney test for 2 groups and Kruskal-Wallis test for multiple groups. Multiple regression was used to estimate the influence of preoperative factors on the outcomes according to WOMAC and SF-12. A P value of <.05 was considered to be statistically significant.
Results
Of the 314 patients enrolled, 294 completed the study. There were 20 participants who failed to show up for postoperative follow-up and were excluded from the study. There were 243 (82.7%) females and 51 (17.3%) males. The mean age at surgery was 70.86 ± 8.28. The mean BMI was 33 ± 6.19 (range 19.27-55.53). 191 (65%) patients were with lower education. 200 (68%) patients were socially supported.
According to BMI, patients were split into 4 groups—less than 30 (102 patients, 34.7%), from 30 to 35 (94 patients, 32.0%), from 35 to 40 (63 patients, 21.4%), and more than 40 (35 patients, 11.9%).
At the time of surgery, women mean age were 1 year younger compared to men, but reported statistically significant lower physical function (P = .002), more pain (P = .001), and more stiffness (P = .004) as measured by WOMAC. Also, women scored lower on MCS (P = .025). The baseline characteristics by gender are presented in Table 1.
Preoperative WOMAC and SF-12 Scores According to Patient’s Gender.

Abbreviations: CI, 95% confidence interval; MCS, mental health composite score; Md, median; SD, standard deviation; SF-12, Short Form-12; PCS, physical health composite score; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
There were significant differences in WOMAC pain domain (P = .035) and SF-12 MCS (P = .023) between different age groups. Older group showed better preoperative results (Table 2).
Preoperative WOMAC and SF-12 Scores According to Patient’s Age.

Abbreviations: CI, 95% confidence interval; MCS, mental health composite score; Md, median; SD, standard deviation; SF-12, Short Form-12; PCS, physical health composite score; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Patients with higher education experienced less pain (P = .010) and demonstrated better knee function (P < .001) preoperatively according to WOMAC (Table 3). There were no differences in WOMAC stiffness (P = .854) domain and SF-12 physical (P = .246) and mental (P = .703) function domains between these groups.
Preoperative WOMAC According to Patients’ Level of Education.

Abbreviations: CI, 95% confidence interval; Md, median; SD, standard deviation; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
The cohort’s preoperative WOMAC scores according to BMI are presented in Table 4. Patients with BMI ≥40 kg/m2 (group IV) had significantly worse preoperative WOMAC pain and stiffness scores compared to patients with BMI <30 kg/m2 (group I) and BMI = 30-35 kg/m2 (group II) and worse function score compared to patients with BMI <30 kg/m2 (group I; Table 4). There were no differences between 4 groups according to SF-12.
Preoperative WOMAC Scores According to Patients’ BMI.
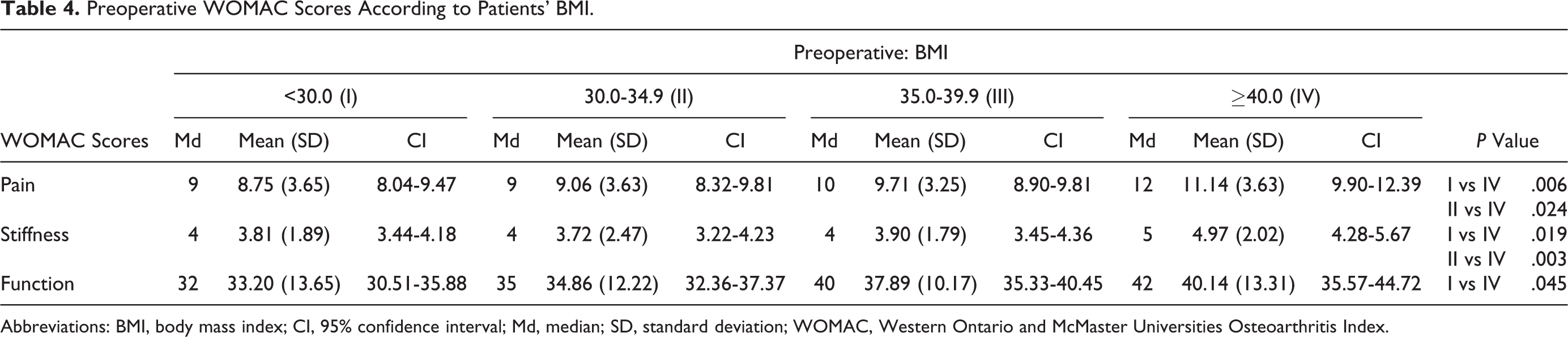
Abbreviations: BMI, body mass index; CI, 95% confidence interval; Md, median; SD, standard deviation; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
There were no statistically significant differences in baseline WOMAC or SF-12 across social support categories.
Despite overall improvement of knee function after TKA in all patient groups based on WOMAC and SF-12 assessments, we found some statistically significant differences. The women compared to the men showed significantly inferior results only in WOMAC pain (P = .023) and function (P = .005) domains. Despite significant difference in stiffness domain before surgery, there were no difference 12-month postoperatively (P = .061). Also, men showed better results according to SF-12 PCS (P = .049) and MCS (P = .020) domains 12 months after surgery (Tables 1 and 5).
Postoperative WOMAC and SF-12 Scores According to Patient’s Gender.
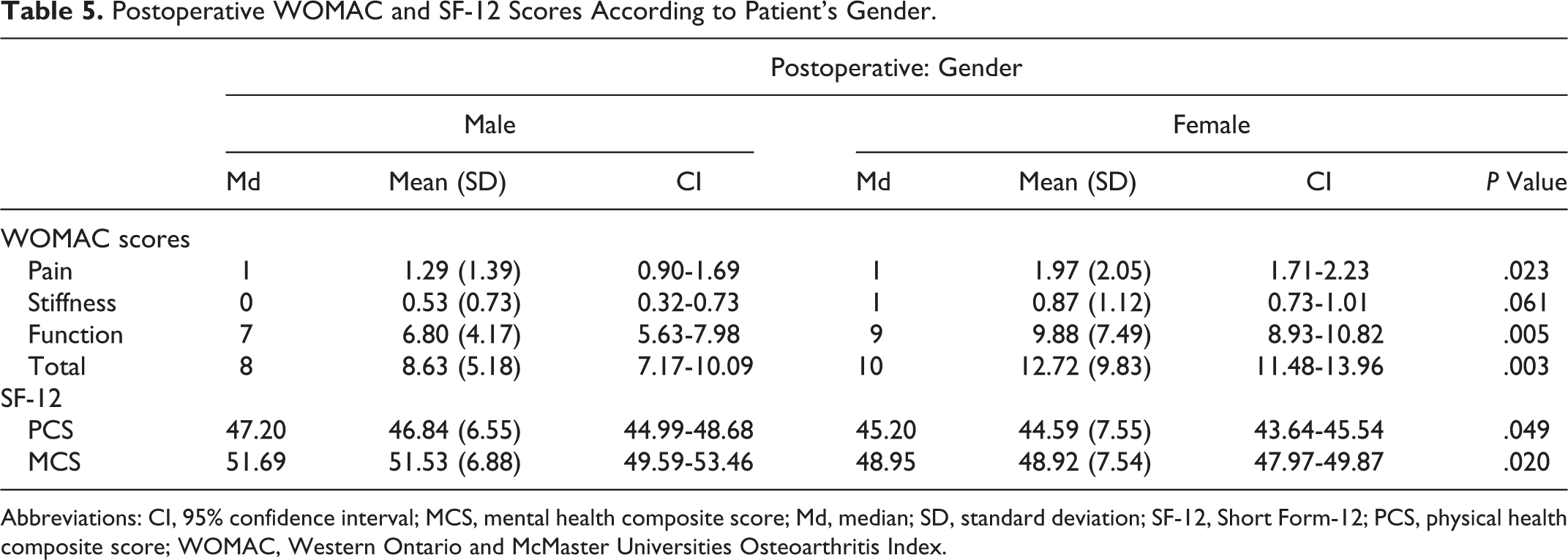
Abbreviations: CI, 95% confidence interval; MCS, mental health composite score; Md, median; SD, standard deviation; SF-12, Short Form-12; PCS, physical health composite score; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
There were no differences in pain (P = .592), stiffness (P = .729), and function (P = .082) according to WOMAC and SF-12 physical (P = .082) and mental (P = .559) health score between younger and older patient groups 1 year after TKA.
Despite differences in WOMAC pain and function scores before surgery, there were no differences in pain (P = .168), stiffness (P = .059), and function (.225) WOMAC domains and in SF-12 physical (P = .461) and mental (P = .594) health scores between patient groups with different level of education 1 year after TKA.
The study results showed no differences in pain (P = .547), stiffness (P = .081), and function (P = .664) according to WOMAC and SF-12 physical (P = .933) and mental (P = .510) health scores between groups differing by BMI 1 year after surgery.
There were no differences in pain (P = .874), stiffness (P = .601), and function (P = .160) according to WOMAC12 months after surgery between patient groups with different social support. Patients with social support showed significantly superior postoperative overall physical function according to SF-12 (PCS; P = .008) and no difference in mental function according to MCS domain (P = .833).
Multiple regression was used to estimate the influence of preoperative factors on the outcomes according to WOMAC and SF-12. The study results showed that women sex, poor preoperative knee function, poor overall physical and mental health, and absence of social support were predictors of worse outcome 12-month after TKA according to WOMAC and SF-12.
Discussion
The TKA has been shown to lead to dramatic improvements in the functioning and quality of life of patient with OA. Unfortunately, not all patients do well and are satisfied with the results. 14 The incidence of dissatisfaction or suboptimal outcome after TKA varies in the literature. Variations in reporting may be due to the wide range of questionnaires used and lack of consensus among physicians how to use them. 15,16 In our study, we prospectively evaluated the effect of patient’s factors such as age, gender, educational level, social support, and BMI on the outcome after TKA.
The influence of patient’s gender on self-reported results after TKA remains an important issue. Our study presents significant differences in knee and overall function between genders before and 12 months after TKA. The WOMAC scores were significantly worse in women as preoperative and at 1 year follow-up. Our review of recent literature reveals that women demonstrate lower knee function and have more severe pain preoperatively. 4,17 -20 There are some differences in postoperative scores favoring men 17,21,22 and showing no difference in functional outcome between men and women. 4 The degree of improvement in postoperative scores generally favor women. 17 -19,23 However, women don’t reach the same final functional level as men. 17,18,24,25 The same findings are in SF-12 scoring system. Women begin and end with lower scores than men. 17 According to preoperative WOMAC and SF-12 scores, men are more likely to choose surgery earlier in the disease, which allows them to achieve better functional results.
Due to increasing life expectancy and general health improvement, age of patients who would benefit from TKA is growing. Still much clinical controversy exists with respect to age and the risk of surgery. Family physicians, rheumatologists, and surgeons are confronted with weighing the risks and benefits of TKA for older patients. We compared pre- and postoperative results in 2 groups differing by age. Age cutoff was 75 years. The difference was significant in preoperative WOMAC pain and in SF-12 mental function domains. The patient group ≤75 years demonstrated lower mental function and had more pain in their knee. Possible explanation for this could be that older people may tolerate higher pain level. We don’t see any statistical differences between groups 12 months after surgery. 6,13,26 -28 It means that age should not be a barrier in considering surgery.
Obesity is becoming a worldwide health problem. More and more surgical candidates are overweight or morbidly obese, therefore we feel importance to assess weight impact as a risks factor on the outcome after TKA. According to the literature, the effect of obesity on the outcome of TKA is unclear. Some studies report no adverse association between obesity and TKA functional outcome, 23,29,30 others report a poorer TKA outcome in obese patients. 31 We compared functional status of our patients before and after surgery using WOMAC and SF-12 scores in 4 groups based on BMI score (<30.0, 30.0-34.9, 35.0-39.9, ≥40.0). In preoperative WOMAC assessment morbidly obese group (BMI ≥40) showed significantly poorer function results. There were no statistically significant differences in postoperative scores between groups. Similar results are reported by Ayyar et al. 3
Review of literature reveals limited assessment of socioeconomic impact on outcomes after TKA surgery. In our study, we grouped patients based on their educational status. Our data demonstrated that patients with lower education had significantly worse preoperative WOMAC scores, but after 12 months this difference was not significant. It’s clear that less educated patients appeared to have a greater need for TKA but educational status didn’t affect the final outcome. Less educated people appeared to be able to compensate for their worse preoperative scores and obtain similar outcomes. There are controversial data in the literature, concerning the impact of socioeconomic factors on results of TKA. Some studies report that patients with lower income and education demonstrate lower functional outcome results. 12,32 Murray et al 33 found no correlation between socioeconomic status and preoperative disease severity or the outcome after TKA. We got very similar results as Davis et al 34 in prospective observational study performed in 13 centers in 4 countries (4 in the United States, 6 in the United Kingdom, 2 in Australia, and 1 in Canada). Their results demonstrated that patients with lower income had significantly worse preoperative WOMAC. However, this did not translate to worse postoperative outcome at final follow-up. In the Republic of Lithuania, lower income status is not a barrier to access TKA as National Health System provides equal access to care, irrespective to income. The reason of lower preoperative functional scores in lower educated patient group could be unwillingness and lack of desire to receive treatment. Maybe preoperative expectations between patient groups differ. Postoperatively, the fulfillment of these expectations appears to be an important determinant of patient-reported outcome.
Some studies demonstrate that social support level may play an important role in moderating the effects of pain and physical disability in patients with OA. 27,35 -37 In our study, socially supported patients (living together with family members) demonstrated significantly better physical function according to SF-12 1 year after surgery. It means that social support plays a great role in achieving better physical function in postoperative period.
Our results show that poor preoperative knee function, poor overall physical, and mental health are predictors of worse outcome 12 months after TKA according to WOMAC and SF-12. It means that baseline symptom severity is a predictor of outcome after TKA. Similar results are published by Lingard et al. 4 They presented data from large study involving 860 recipients of primary TKA from 3 different countries.
This study has a limitation that our socioeconomic assessment is limited only to educational level, as data in regards of income status was not recorded.
The strengths of our study are its prospective design, the high rate of return to follow-up, and all patients involved in this study were operated in a single institution with the same postoperative and rehabilitation protocol.
Conclusion
There is no difference in self-reported functional outcome between patient groups differing in age, BMI, and education. Men and socially supported patients demonstrate better postoperative functional results 12 months after TKA. Male sex, better preoperative knee function, and overall physical and mental function are predictors of better outcome 1 year after TKA. Age and obesity should not be limiting factors when considering who should receive this surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.