
Abstract
Objectives:
To assess the effect of insurance type (Medicaid, Medicare, and private insurance) on fragility fracture patients’ access to endocrinology specialists in the postoperative period.
Materials and Methods:
The research team called 247 board-certified endocrinologists in 8 representative states. The caller requested an appointment for her fictitious mother to be evaluated for osteoporosis after suffering a hip fracture that required surgery. The caller stated that her mother had an abnormal level of parathyroid hormone and her mother’s orthopedic surgeon believed she needed to see an endocrinologist. Each office was called 3 times to assess the responses for each insurance type. For each call, we documented whether the patient was able to receive an appointment and the barriers the patient confronted to receiving an appointment.
Results:
About 15.8% of offices scheduled an appointment for a patient with Medicaid, compared to 48.6% for Medicare and 54.3% for BlueCross (P < .0001). Medicaid patients confronted more barriers to receiving appointments. There was no statistically significant difference in access for Medicaid patients in states that had expanded Medicaid versus states that had not expanded Medicaid. Medicaid reimbursement for a new level 3 patient visit did not significantly correlate with appointment success rates or wait times.
Conclusion:
Despite the passage of the Affordable Care Act, Medicaid patients have reduced access to endocrinologists and more complex barriers to receiving appointments. A more robust strategy for increasing access to care for Medicaid patients would be more equitable.
Keywords
Introduction
Approximately 10 million Americans suffer from osteoporosis, a disease that places patients at an increased risk of suffering a fracture to the hip, pelvis, vertebrae, and wrist. 1,2 Patients with fragility fractures incur increased health-care costs, have a higher risk of mortality, and are at an increased risk of a subsequent fracture. 1,2
Medical management of osteoporosis can reduce the number of future fractures and therefore the morbidity, mortality, and cost associated with those fractures. 3 -5 Orthopedic surgeons are regularly the first medical professionals to treat patients presenting with fragility fractures. 6 However, while patients are being surgically managed, orthopedic surgeons rarely initiate an osteoporosis workup despite evidence demonstrating that patients would benefit. 7 -10 In addition, patients with recent fragility fractures are unlikely to be seen by their primary care physician in a timely fashion for medical management of osteoporosis or referred to an endocrinologist. The orthopedic surgeon has been recognized as being in the ideal position to identify patients who may benefit from medical management of osteoporosis for secondary prevention of fractures. 11
The orthopedic clinics are ill equipped to medically manage osteoporosis, and orthopedic surgeons primarily depend on the patient’s primary care physician or endocrinologist. 12 Multiple studies have demonstrated that the involvement of the endocrinology service during the patient’s initial hospitalization or upon discharge has improved outpatient medical management of osteoporosis. 13,14
Anecdotally, patients with recent fragility fractures have struggled to obtain access to endocrinologists. This study was designed to identify barriers that fragility fracture patients experience when seeking endocrinologists for assistance with osteoporosis. The purpose of this study was to evaluate whether the insurance status (Medicaid, Medicare, and private insurance) of patients with fragility fractures affected their access to endocrinologists in the setting of the Patient Protection and Affordable Care Act (PPACA). We hypothesize that despite the passage of the PPACA, Medicaid patients will have increased difficulty obtaining access compared to patients with other types of insurance and that the Medicaid reimbursement rate for office visits will remain an important determinant of timely care.
Since the passage of the PPACA, Medicaid eligibility expanded from covering those with incomes 61% of the federal poverty level or below to anyone with incomes up to 138% of the poverty level. 15 However, a Supreme Court ruling allowed each state to decide whether to expand Medicaid. Currently, 31 states and the District of Columbia have done so. While this has left patients residing in states without expanded Medicaid eligibility with a significant coverage gap, there are many more patients who are now eligible for Medicaid in states that have expanded the eligibility requirements. 15 We designed our study to identify whether there are any differences in access for patients in states with expanded Medicaid eligibility versus those without.
Materials and Methods
The study was submitted to and approved by the institutional review board office, HIC# 13637. The study population included board-certified endocrinologists who treat patients with osteoporosis in 8 representative states: California, Florida, Georgia, Massachusetts, New York, North Carolina, Ohio, and Texas. These states were selected because of their diverse geographic areas and health-care marketplaces. The American Board of Medical Specialties’ Certification Matters website 16 was used to create an alphabetized list of physicians specializing in either “endocrinology and metabolism” or “endocrinology, diabetes, and metabolism” for each state. A random number was assigned to each physician, dictating the order in which offices were called. If a physician’s office phone number was inaccurate and the correct number could not be found with a Google search, the physician was excluded from the calling list, and the next number was selected. To avoid the possibility of revealing the nature of the study by repeating an identical script to the same receptionist, physicians were also excluded if a successful call had previously been made to a different physician in the same office.
Each office was called to make an appointment for the caller’s fictitious mother who had recently suffered a fragility fracture of the hip. Following orthopedic management of the fracture, blood work revealed an elevated parathyroid hormone level. The caller had a standardized script (see Appendix A) to limit intra- and interoffice variation. The caller first verified whether the physician treated patients with osteoporosis. If this was not the case, the physician was removed from the data set and the next number was called. The caller then verified whether the physician was accepting new patients. If not, the physician was removed from the data set. Approximately 30 physicians were called per state. Three separate calls were made to each office stating that the patient had Medicaid, Medicare (with supplemental insurance), or BlueCross health insurance. The status of having Medicare supplemental insurance was only clarified if the office requested. Phone calls for each insurance type were made in the same order for each office with over a week separating each call. No actual appointment was scheduled to avoid disadvantaging patients who needed care.
For each attempt at making an appointment, the date of the call and the date of appointment, if offered, were recorded. If an appointment was denied due to Medicaid insurance status, we recorded whether the office made a referral to another office that accepted Medicaid. If an office required a referral from a primary care physician before granting an appointment, we considered this as an unsuccessful attempt at making an appointment, as obtaining a referral is an additional barrier to gaining an appointment. The waiting period for an appointment was calculated by determining the time between the date of the call and the date of the appointment. For both appointment success rates and waiting periods, the data were stratified into 2 groups: states with expanded Medicaid eligibility (California, Massachusetts, New York, and Ohio) and states without expanded Medicaid eligibility (Florida, North Carolina, Georgia, and Texas).
The Medicaid reimbursement rates for a level 3 new patient evaluation and management code were obtained by querying each state’s reimbursement rate using Current Procedural Terminology code 99203.
Statistical analysis was performed using SPSS version 21 (SPSS, Inc, Chicago, Illinois). Chi-square test or Fisher exact test was used to analyze differences in acceptance rate based on the type of insurance. To compare the time period to an appointment, an independent samples t test was used after applying natural log transformation, as the data were not normally distributed. Univariate regression analysis was performed to detect whether Medicaid reimbursement was a significant predictor for successfully making an appointment for Medicaid patients. Unless otherwise stated, all statistical testing was performed 2 tailed at an α-level of 0.05.
Results
Our query from the American Board of Medical Specialties website resulted in a total of 247 endocrinologists across 8 states (4 states with expanded Medicaid eligibility [California, 32; Massachusetts, 31; New York, 31; and Ohio, 30] and 4 states without expanded Medicaid eligibility [Florida, 32; Georgia, 30; North Carolina, 31; and Texas, 30]).
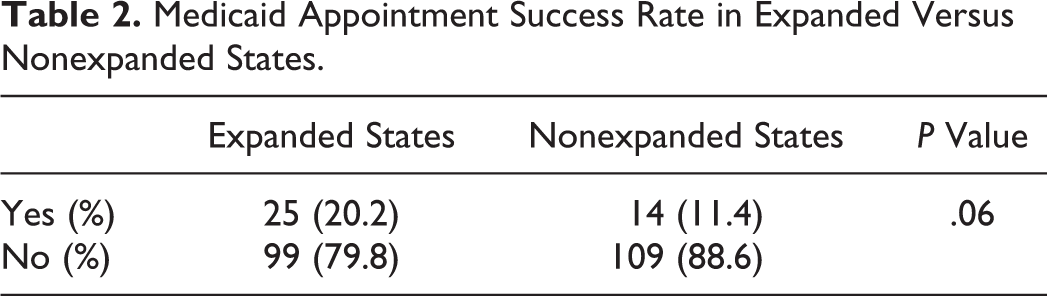
The overall success rate for obtaining an endocrinology appointment was 15.8% for Medicaid, 48.6% for Medicare, and 54.3% for BlueCross (Table 1). For states with expanded Medicaid eligibility, the success rate for obtaining an appointment was 20.2% for Medicaid, 50.0% for Medicare, and 50.8% for BlueCross. For states without expanded Medicaid eligibility, the success rate for obtaining an appointment was 11.4% for Medicaid, 47.2% for Medicare, and 57.7% for BlueCross. In all cases, the success rate was significantly lower for Medicaid compared to either Medicare (P < .0001) or BlueCross (P < .0001). There was no statistically significant difference between the success rates of Medicaid patients obtaining appointments in states with expanded Medicaid versus states without expanded Medicaid eligibility (Table 2).
Appointment Success Rate.

aComparison with Medicaid.
Medicaid Appointment Success Rate in Expanded Versus Nonexpanded States.
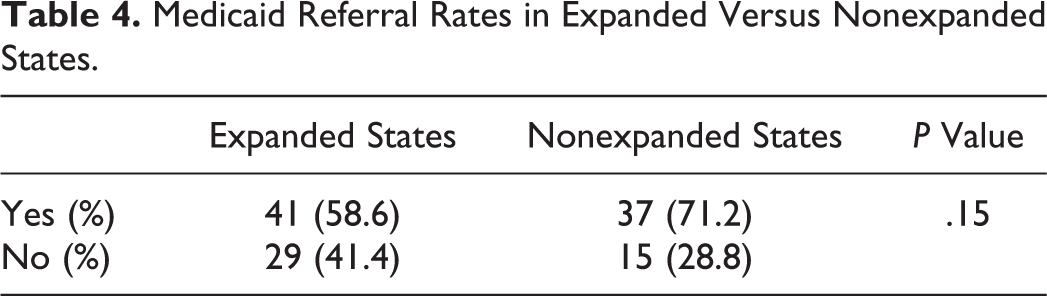
For Medicaid patients, insurance status was the most common reason for the inability to make an appointment (51.4% not accepted compared to 2.8% for Medicare and 2.8% for BlueCross). The second most common reason was the need for a referral from a primary care physician (Table 3). Overall, more Medicaid patients were required to have a referral compared to Medicare (63.9% vs 49.0%, P < .007) and BlueCross (63.9% vs 42.4%, P < .0001). This relationship is also significant when comparing Medicaid to Medicare (71.2% vs 50.4%, P < .012) and BlueCross (71.2% vs 40.5%, P < 0.0001) patients in states without expanded Medicaid eligibility but is not statistically significant when comparing Medicaid to Medicare (58.6% vs 47.6%, P < .14) and BlueCross (58.6% vs 44.3%, P < .056) in states with expanded Medicaid eligibility. Medicaid referral rates were not statistically significant between expanded versus nonexpanded states (Table 4). A total of 120 (95%) of the 126 offices that did not accept Medicaid were not able to refer Medicaid patients to another endocrinologist who would accept Medicaid.
Required Referral Rate.

aComparison with Medicaid.
Medicaid Referral Rates in Expanded Versus Nonexpanded States.
Reimbursements for a level 3 visit varied across states (Table 5). For Medicaid, North Carolina paid the highest reimbursement (US$80.86) and Florida paid the lowest (US$48.68). For Medicare, California paid the highest reimbursement (US$112.75) and Georgia paid the lowest (US$103.01). The average difference in reimbursements between the 2 insurance types was US$64.68. Logistic and linear regression analysis did not predict a significant relationship between reimbursement and appointment success rate or waiting periods.
Medicaid Reimbursements for a Level 3 Appointment Current Procedural Terminology code 99203 in 2014.

Abbreviation: CPT, Current Procedural Terminology.
aStates with expanded Medicaid eligibility.
Overall, waiting periods were statistically longer for Medicaid patients when compared to Medicare (44.3 vs 40.1 days, P < .048) but not BlueCross (Table 6). Medicaid patients in states without expanded Medicaid had longer wait times than Medicare patients (47.5 days vs 40.0 days) but not BlueCross patients. Medicaid patients in states with expanded Medicaid eligibility had shorter wait times than Medicaid patients in states without expanded Medicaid eligibility (42.5 vs 47.5 days, P < .0001), and BlueCross patients in states with expanded Medicaid eligibility waited longer than BlueCross patients in states without expanded Medicaid eligibility (43.6 vs 42.8 days, P < .005; Table 6).
Waiting Period (Days) Organized by the Insurance Type.

aComparison with Medicaid.
Discussion
This study assessed the effect of insurance type (Medicaid, Medicare, and BlueCross) on patient access to endocrinologists in 8 geographically representative states. Our scenario involved a patient with a recent fragility fracture seeking an evaluation for osteoporosis. We chose this scenario as previous literature has demonstrated the value of having endocrinologists working up patients with fragility fractures. 13,14 Our hypothesis was that Medicaid patients would have reduced access to care. Given the extent that the PPACA has expanded Medicaid coverage, it is important to assess whether increased coverage equates to increased access.
Our national sample of endocrinologists demonstrated that Medicaid patients have the lowest rate of successfully obtaining an appointment (15.8% vs 48.6% for Medicare, P < .0001 and 54.3% for BlueCross, P < .0001). While the appointment success rate was higher in Medicaid expanded states (20.2% vs 11.4%, P < .06), the difference was not statistically significant.
The requirement for patients to have a referral in order to receive an appointment was a particular barrier that primarily affected Medicaid patients (Table 2). A suspected reason for why more Medicaid patients are required to have primary care physician (PCP) referrals may be due to the perceived extra workload and lower reimbursement. Previous studies have demonstrated that Medicaid patients typically require more resources due to their increased complexity and lower safety net and the associated burdensome paperwork requirements and longer waiting periods before payment. 17,18 In addition, the requirement to have a referral is viewed as a barrier to many patients in underserved communities who lack the life skills and resources to coordinate the referral.
Of note, the Medicaid policies for 4 states included in our study (Massachusetts, North Carolina, Texas, and New York) required a PCP referral in order to see a specialist. However, we found that many practices in these states scheduled appointments for Medicaid patients without a PCP referral, suggesting that the decision depended on individual policy. In addition, the majority of offices in these states cited that they simply do not accept Medicaid as an insurance policy, not that they require a referral, which is consistent with results from previous studies. 19 -21
Given their limited availability, endocrinologists may require referrals to select more complex patients for their practice. The medical community refers to them only their most complex patients who cannot be adequately managed by general internal medicine physicians.
Our regression analysis did not predict a significant relationship between appointment success for a level 3 visit and reimbursement rates for Medicaid. Although studies have stressed the importance of reimbursements on physician participation, this result is consistent with previous works on patient access to carpal tunnel release and total ankle replacement. 22,23 Long 18 suggested that although reimbursements may help, additional strategies for promoting Medicaid acceptance may be needed, such as lowering the costs of participating in Medicaid by simplifying administrative processes, speeding up reimbursement, and reducing the costs associated with caring for those patients.
When comparing wait times, while the overall wait times were statistically significantly longer for Medicaid patients, the absolute wait times were not overwhelmingly different. This is likely due to office scheduling policies, which rely less on insurance type and more on the acuity of the appointment request.
The literature has identified the health-care professional as being responsible for failing to initiate treatment for osteoporosis. 8 In particular, the orthopedic surgeon is likely to be 1 of the first medical providers to treat the fractures of the patient and diagnose the patient with osteoporosis. 6 The literature has demonstrated that surgeons rarely initiate osteoporosis workups after a fragility fracture. 7 It is unclear whether poor endocrinology access is a reason for this.
The goal of the PPACA was to increase access to care. However, patients still face challenges when attempting to access care. It is well published that osteoporosis treatment reduces morbidity 8 and mortality. 3 Bisphosphonates are the standard of care for secondary prevention after a fragility hip fracture. 2 It has been shown that bisphosphonates given within 90 days after surgical stabilization of a fragility hip fracture reduces the rate of new fractures and improves survival. 24 Interventions in the health-care system, including an osteoporosis workup during hospitalization, 25 a hip fracture admission order set that includes an endocrinology consult, 14,26 and the addition of a dedicated health-care provider who specifically treats osteoporosis in the orthopedic clinics, 25,27 serve to increase the number of patients who are screened and ultimately treated for osteoporosis. However, patients have demonstrated difficulty in seeing their primary care physician for osteoporosis workup and management following referral by their orthopedic surgeon, 9 and our study demonstrates that the same holds true for endocrinologists. This is further complicated by the inability of hospitals to be reimbursed for bone density evaluations on sentinel hip fracture admission and the lack of reimbursement for osteoporosis medications in the subacute rehabilitation facility.
There are several studies that demonstrate that coordination between the orthopedic and endocrinology services, especially with outpatient management, leads to improved outcomes. 8,13,28 -31 One system that has shown success has been the Kaiser Southern California Healthy Bones Program. The deployment of an aggressive bone health program that facilitated the management of osteoporosis in patients with recent fragility fractures with the referral of complex patients to endocrinology was able to reduce the number of hip fractures by 37%. 8 In a separate study, Piziak and Rajab demonstrated that an outpatient endocrinology discharge order for all hip fracture patients increased the number of patients managed by endocrinology as an outpatient, as well as the use of calcium and vitamin D supplementation and bisphosphonates. 13 Multiple studies have demonstrated that case managers or nurses assigned to patients with recent fragility fractures while in the hospital for their fracture care have increased the percentage of patients treated for osteoporosis and decreased the percentage of fragility fractures. 28 -31 These studies suggest fracture liaison services are effective in facilitating osteoporosis evaluations for patients who may have otherwise received no further treatment following orthopedic management.
Given the challenge our patient had in accessing endocrinologists, it is likely that there is a specialist shortage. Vigersky et al created a model to evaluate the current endocrinology workforce and calculated that there is a current shortage of approximately 1500 endocrinologists. 32 Increasing the number of physicians training to be endocrinologists may improve access as well.
Our study has several limitations. We wanted to simulate the experience that a patient would have when trying to schedule an appointment, so our scenario did not control for the relative seniority of the endocrinologists. It is likely that younger physicians with newer practices would have fewer barriers to scheduling an appointment. On the other hand, it is unlikely that physician seniority is a major influence for patients seeking appointments. For cost and time efficiencies, our study concentrated on 8 states that were selected from diverse regions across the nation. A complete national survey would likely yield a more representative analysis. Furthermore, some of the results that are very close to being statistically significant might have become significant with a larger sample size. The power analysis was for a combined study of 8 states. The prospective power analysis determined that our sample size needed to consist of 241 endocrinologists to detect an effect size of at least 0.2 between the acceptance rate of Medicaid versus other insurance types at a power of 80%. We did call at least 30 offices per state but that was not the intent of the original study, as we were not planning on doing a state-by-state comparison. A state-by-state comparison was not included in the limited scope of this project and would not have been adequately powered with the given data set. This would be an important next step for future study. In addition, this study did not control for other factors, such as lack of transportation, difficulty with getting time off from work, or inadequate education about insurance coverage, that can be barriers to access. Such issues are especially relevant for Medicaid patients as their primary insurance and should be further analyzed in future studies.
Conclusion
Despite the passage of the Affordable Care Act, Medicaid patients have reduced access to care for osteoporosis. A more robust strategy for increasing access to care for Medicaid patients is required. Such a strategy may need to go beyond increasing reimbursements, as our study demonstrated that higher reimbursements do not necessarily increase acceptance of Medicaid. Other actions, such as simplifying and accelerating the administrative steps for Medicaid reimbursements, may be necessary. In addition, either the treating orthopedic surgeon or a fracture liaison service may need to coordinate referrals to endocrinologists, given the barriers patients face when they attempt to schedule their own appointments. Reduced access to endocrinology care may unfortunately affect the utilization of bisphosphonates, which is a standard of care for secondary prevention of fractures.
Footnotes
Appendix A
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.