
Abstract
Background:
Life-threatening arterial bleeding from fragility fractures of the pelvis are very rare but associated with significant mortality, especially in anticoagulated patients.
Case Description:
We report the successful interdisciplinary management of a 78-year-old woman under anticoagulation and antiplatelet therapy who had life-threatening arterial hemorrhage from the pubic rami following a fragility fracture of the pelvis. Our management strategy included early hemorrhage control by means of selective arterial embolization followed by surgical fracture stabilization and surgical hematoma evacuation.
Literature Review:
We identified 6 cases within the English literature, all involving females older than 70 years. All patients under anticoagulation developed hemorrhagic shock, and in 2 cases selective embolization contributed to survival of the patient. However, a combined management including fracture stabilization and hematoma evacuation has not been reported, allowing an excellent clinical outcome and discharge to geriatric rehabilitation.
Clinical Relevance:
This case illustrates that elderly patients with apparently benign pelvic fragility fractures might develop severe hemorrhage due to arterial injury, especially when under dual anticoagulation, and stresses the importance of a high index of suspicion. If bleeding is suspected, detailed imaging studies are necessary to determine the source of bleeding and immediate angiographic or surgical interventions in combination with volume resuscitation and coagulation therapy should be readily available.
Case Presentation
A 78-year-old female sustained blunt low-energy trauma in a ground-level fall on the right pelvic girdle. She presented to the emergency department of a local trauma center and was complaining of pain in the right groin and inability to weight bear. There was a past medical history of coronary heart disease, atrial fibrillation, chronic heart failure (New York Heart Association IV), diabetes, and obesity. She was taking coumadin and acetylsalicylic acid on a daily basis. The hemodynamic status deteriorated during radiographic workup, which revealed a simple pubic rami fracture. In contrast to the apparently benign fracture pattern, the Focused Assessment with Sonography for Trauma (FAST) scan was positive for free fluid in the lower peritoneum. Active bleeding was suspected and transfer to a Level I trauma center was coordinated. Before transfer, volume resuscitation (1000 mL) was combined with 6 mg vitamin K and 500 I.E. of human prothrombin complex concentrate administration, containing factors II, VII, IX, and X and protein C and S. One hour after injury, the international normalized ratio was measured: 1.8 (Table 1). After admission to the level I trauma center, emergent multiple contrast computed tomography (CT) angiography (CTA) confirmed active arterial hemorrhage from the corona mortis close to the fractured right iliopubic rami. An osteoporotic right sacral fracture (Denis type 1) was also identified in the CT scan. In consequence, the pelvic ring injury was classified as a partially unstable fragility fracture of the pelvis type IIC. 1,2
List of Therapeutic Interventions.

Abbreviation: BP, blood pressure; Hb, hemoglobin; INR, international normalized ratio; HR, heart rate.
Right after imaging the patient developed hemorrhagic shock. Arterial blood pressure was 90/55 mm Hg and heart rate (HR) was 122 bpm. Hemoglobin (Hb) levels dropped from 13.9 g/dL to as low as 7.5 g/dL within the emergency department phase. Immediate angiography and coil embolization (Hilal Microcoils, Cook Medical, Bloomington, IN, USA) was performed in crossover technique (Figures 1 and 2). Simultaneously, she was transfused urgently, receiving a total of 4 units of blood. Following successful embolization, the patient was transferred hemodynamically stable (121/76 mm Hg, HR 92 bpm, Hb 9.7 g/dL) to the intensive care unit. In order to avoid recurrent bleeding due to mobile fracture fragments and to allow early mobilization, surgical stabilization of the posterior pelvic ring with a percutaneous fully threaded sacroiliac (SI)-screw (Figure 3) and external fixation of the anterior pelvic ring was scheduled for the following day. Due to persistent oliguria with hydronephrosis from the significant and compromising intrapelvic hematoma formation (Figures 4 and 5), surgical stabilization was combined with hematoma evacuation over a modified Pfannenstiel approach. In the postsurgical course, the obese patient was successfully mobilized with partial weight bearing (20 kg) on the affected right side. She was discharged to geriatric rehabilitation 15 days after sustaining the injury. No complications were observed in the hospital course, and the external fixation was removed 4 weeks after surgery.

Angiographic confirmation of active bleeding from corona mortis.

Angiographic intervention: coil-embolization of corona mortis.
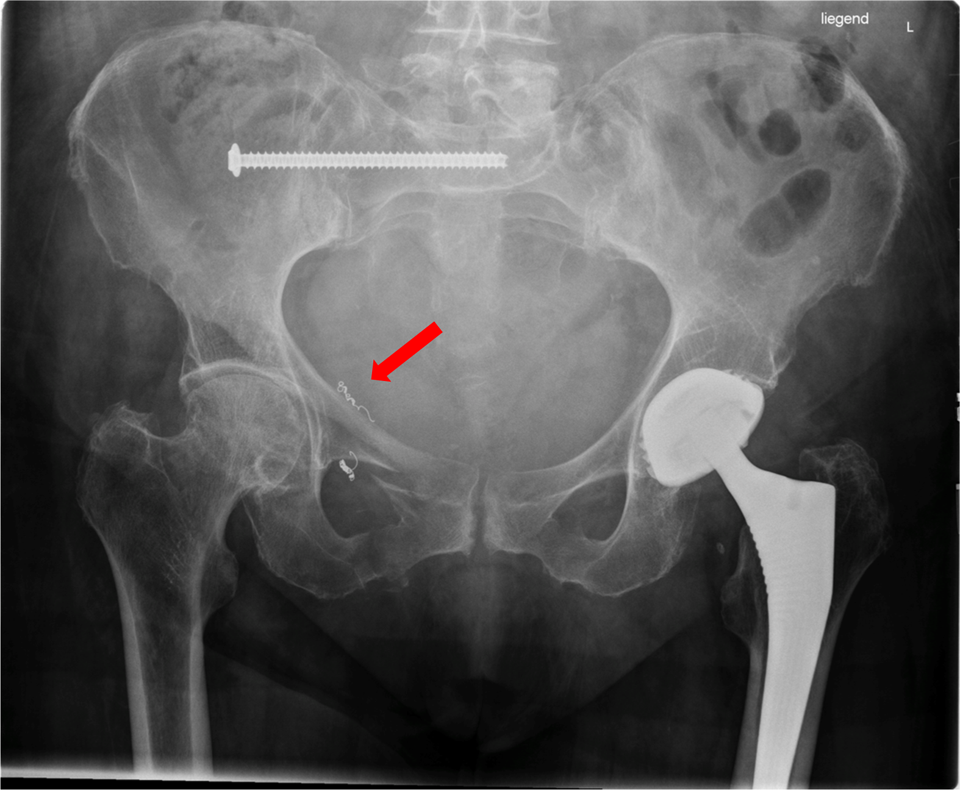
Follow-up plain X-ray of pelvis (anteroposterior) after removal of external fixator.

Computed tomography angiography (CTA; coronal view) confirmation of active bleeding near pubic ramus.

Computed tomography (CT) angiography (sagittal view): Dimensions of intrapelvic hematoma.
Discussion
After obtaining informed consent, we report a case of the interdisciplinary successful management of a life-threatening arterial hemorrhage from the corona mortis following an osteoporotic fragility fracture of the pelvis. Low-energy pelvic trauma typically occurs in elderly osteoporotic females and is frequently associated with fractures of the pubic ramus. However, life-threatening arterial hemorrhage is rarely associated with these fragility fractures and is mostly reported for elderly patients receiving anticoagulant and/or antiplatelet therapy. 3 –6,7 –10
Reported treatment algorithms included solely transfusion protocols or the combination of embolization and transfusion. In general, it appears that self-tamponade cannot be expected by arterial bleeding in pelvic trauma; thus management protocols with solely transfusion appear questionable. Accordingly, the patient reported by Coupe et al died. 11 This patient was in shock only 6 hours after admission (Hb 3.3g/dL), was resuscitated twice, but died from cardiorespiratory arrest. In postmortem examination, 3L of blood were found in the lower abdomen.
Angiographic Embolization
Selective embolization appears to be the treatment of choice; however, embolization requires a high-quality interventional radiology service 24/7 and the ability to ready these resources within 30 to 60 minutes. The timing of embolization is the crucial factor in the management of these patients and can be seen in the review of published patient outcomes. From a total of 6 patients found in the literature (Table 2), all individuals had hemorrhagic shock, 4 were under dual anticoagulation therapy, and half of the affected patients (n = 3 of 6) died in the early hospital course. 7,9,11 Differences in timing may be responsible for different outcomes in the reported cases with similar treatment protocols (embolization + transfusion).
Review of Cases With Arterial Bleeding in Fragility Fractures of the Pelvis.
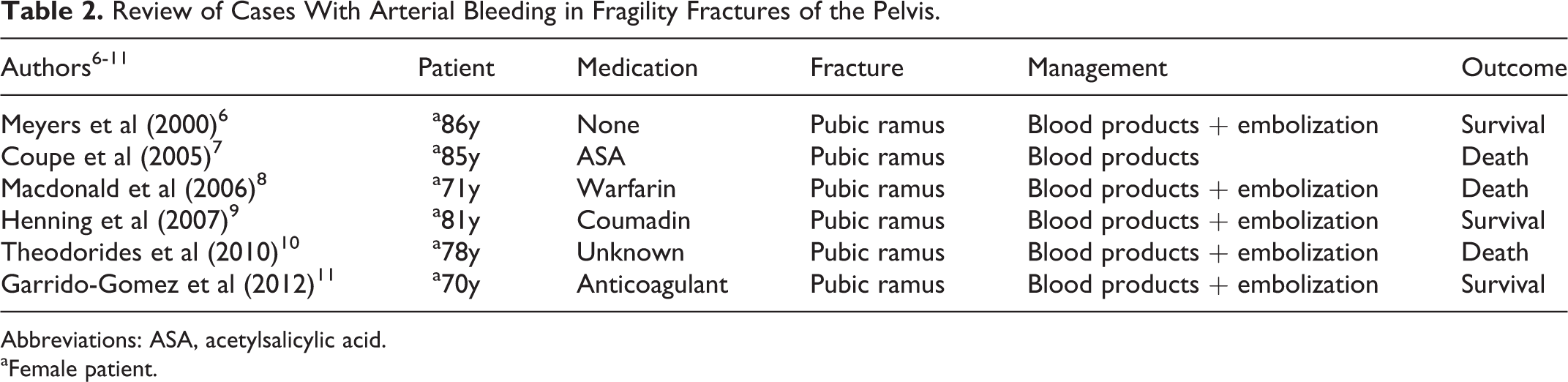
Abbreviations: ASA, acetylsalicylic acid.
aFemale patient.
Pelvic Packing
Open surgery and packing of the bleeding site might be considered as alternative approach 12 if angiographic interventions are not feasible (eg, availability of resources, allergies to contrast medium, accessibility to major arteries). However, pelvic packing appears to be more efficient in venous than in arterial pelvic bleeding; thus, selective embolization should be considered as treatment of choice in case an arterial bleeding has been identified. 7,8,10
Surgical Fixation Under Anticoagulant Therapy
In our case, the patient received both, anticoagulation and antiplatelet medication; thus, the patient is at high risk of prolonged and excessive hemorrhage. As initial step (Figure 6), resuscitation and coagulation management was initiated prior to transfer to our institution. Following the identification of the source of bleeding by emergent multiple contrast CTA, our primary objective was to stop the ongoing hemorrhage and to perform the life-saving embolization immediately. Accordingly, the patient stabilized following this intervention. In type IIc fractures, the risk of instability and nonunion might increase with early mobilization according to Rommens et al; 1 therefore, surgical fixation of the pelvic ring should be considered. Our rationale for minimally invasive surgical fixation of the pelvic ring was to allow early mobilization and to protect the embolized vessel from moving fracture fragments causing recurrent bleeding. Due to massive hematoma formation resulting in urinary obstruction and oliguria, staged fracture fixation was combined with surgical evacuation of the hematoma. In contrast to the existing literature, 6 –11 and despite aggressive surgical management in our algorithm, the patient experienced an excellent outcome, returning to independent life in the domestic environment 8 weeks postinjury.
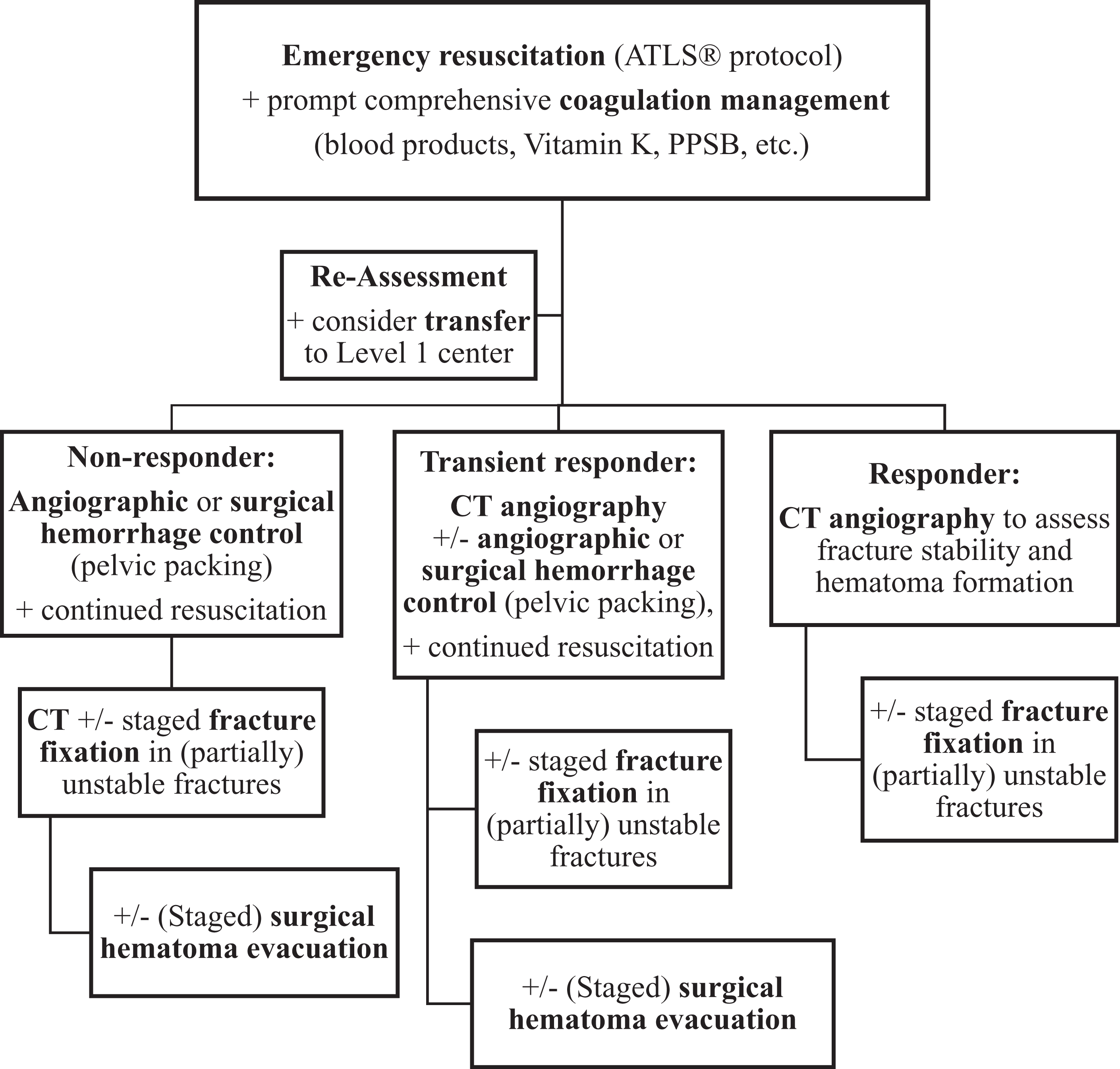
Algorithm for anticoagulated patients with pelvic fragility fracture.
Conclusion
This case illustrates that elderly patients with pelvic fragility fractures might develop severe hemorrhage due to arterial injury, especially when under dual anticoagulation, and stresses the importance of a high index of suspicion. If bleeding is suspected, detailed imaging studies are necessary to determine the source of bleeding and immediate angiographic or surgical interventions in combination with volume resuscitation, and coagulation therapy should be readily available. The lack of evidence-based recommendations concerning the optimal screening and management of the bleeding elderly patients with pelvic fractures needs to be addressed by future studies.
Footnotes
Authors’ Note
Informed consent was obtained from the patient for publication of this case report and any accompanying imaging studies and photographs.
All authors (C.D.W., C.H., T.D., F.H., S.K., H.C.P., P.K.) have made substantial contributions to all of the following: (1) the conception and design of the study, or acquisition of case related data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.