
Abstract
Introduction:
The use of a multidisciplinary clinical pathway (MCP) for patients with hip fracture tends to be more effective than usual care (UC). The aim of this study was to evaluate the effects of an MCP approach on time to surgery, length of stay, postoperative complications, and 30-day mortality, compared to UC.
Materials and Methods:
This multicenter retrospective cohort study included patients aged 50 years or older with a proximal hip fracture who underwent surgery in one of the 6 hospitals in the Limburg trauma region of the Netherlands in 2012. Data such as demographics, process outcome measures, and clinical outcome were collected.
Results:
This study included a total of 1193 patients (665 and 528 patients in the MCP and UC groups, respectively). There were no differences in patient demographics present. Time to surgery was significantly shorter in the MCP compared to the UC group (19.2 vs 24.4 hours, P < .01). The mean length of stay was 10 versus 12 days (P < .01). In the MCP group, significantly lower rates of postoperative complications were observed and significantly more patients were institutionalized than in the UC group. Mortality within 30 days after admission was comparable between the groups (overall mortality 6%).
Conclusion:
An MCP approach is associated with reduced time to surgery, postoperative complications, and length of stay, without a significant difference in 30-day mortality. The institutionalization rate was significantly higher in the MCP group.
Introduction
Hip fracture is a common cause of hospital admission in the elderly patients. The incidence of hip fractures in the Netherlands was 20 000 in 2010 and is expected to increase to 24 000 in 2020. 1 Elderly hip fracture patients frequently present with comorbidities, which are associated with a high risk of developing postoperative complications, resulting in long-term dependency and higher mortality rates. 2 –5 Since the care for elderly patients with hip fracture can be complex and challenging, it is important to optimize medical care in order to minimize adverse outcomes. Multidisciplinary clinical pathways (MCPs) have been developed to optimize medical care in various patient groups. 6 –12 De Bleser et al 13 and Leigheb et al 14 defined MCP as a method for managing a well-defined group of patients during a well-defined period of time, with management consisting of a multidisciplinary team, and stating the goals and key elements of care based on evidence-based medicine guidelines. Using an MCP for patients with hip fracture tends to be more effective than usual care (UC) 14,15 but is presently not standard care. In addition, there are studies that have questioned the benefits of the MCP approach. 16,17
The aim of this study was to evaluate the effectiveness of an MCP approach in terms of time to surgery, length of stay, postoperative complications, and 30-day mortality, compared to UC. The hypothesis tested in this study was that using an MCP approach for hip fracture patients would be associated with an improvement in both process outcome (reducing time to surgery) and clinical outcome (reducing time to discharge and number of complications) measures.
Patients and Methods
This multicenter retrospective cohort study involved patients aged 50 years or older with a proximal hip fracture (femoral neck or pertrochanteric fracture) who underwent surgery in one of the 6 hospitals in the Limburg trauma region of the Netherlands in a 1-year time period in 2012. Patients with pathological hip fractures or polytrauma patients with a hip fracture and hip fracture patients transferred from other hospitals were excluded. Surgical treatment was performed according to Dutch guidelines. 18 The medical ethics committee approved this study, and individual informed consent was waived. All data in the survey were collected retrospectively from the electronic medical records by 2 independent researchers. Demographics of the patients included age, gender, American Society of Anesthesiologists’(ASA) classification, and type of fracture. Outcome measures included time from arrival at the emergency department until surgical procedure, length of hospital stay, postoperative complications, discharge destination, and 30-day mortality. Postoperative complication was defined as any adverse event that required intervention; these were recorded as either present or nonpresent. Data on the occurrence of postoperative delirium and stroke were collected separately. For the analysis, the patients were divided into 2 groups based on the use of an MCP. Three of the 6 hospitals used an MCP, which includes the management from arrival in the emergency department until discharge from the rehabilitation unit of the nursing home. The multidisciplinary team consisted of a standard surgeon, a geriatrician, an anesthesiologist, a physiotherapist, and other specialists, depending on the comorbidities. In addition, the aim was to perform the surgical treatment within 24 hours, and the goal is to get the length of stay to a maximal 4 days. Furthermore, agreements were in place with rehabilitation facilities to transfer the patient to a patient-centered destination as soon as possible in either a rehabilitation center or nursing home with rehabilitation facilities. Management in the other hospitals was defined as UC.
Statistical Analysis
Statistical analysis was performed with IBM SPSS Statistics, version 21.0 (Armonk, New York). Descriptive statistics were used to describe and compare the demographic data and baseline characteristics of the MCP and UC patients. Parametric t test was used for normally distributed data and χ2 test for categorical variables. Results are presented as either mean ± standard deviation (SD) or as frequencies and percentages. Time to surgery (hours from arrival at the emergency department until surgery) and length of hospital stay (days from admission to discharge) are presented as mean and SD. The χ2 test was used to compare the MCP and UC samples regarding operation within 24 hours (yes/no), discharge to rehabilitation clinic (yes/no), discharge to a nursing home (yes/no), discharge to own home (yes/no), postoperative complication (yes/no), postoperative delirium (yes/no), postoperative stroke (yes/no), and mortality within 30 days (yes/no). The level of statistical significance was set at P < .05.
Results
Baseline Characteristics
This multicenter cohort study involved 1193 patients, 665 of them in the MCP group and 528 in the UC group. Characteristics of patients in the MCP and UC hospitals are presented in Table 1. Although patients in the UC group were more likely to have a pertrochanteric fracture than those in the MCP group, no differences in age, gender, or ASA classification were found between the groups (P < .05).
Baseline Characteristics of the MCP and UC Groups.

Abbreviations: ASA, American Society of Anesthesiologists; MCP, multidisciplinary clinical pathway; NS, not significant; SD, standard deviation; UC, usual care.
Process Outcome Measures
Time to surgery was significantly shorter in the MCP group than in the UC group: 19.2 (23.5) hours versus 24.4 (22.5) hours (P < .01). The number of patients who had to wait more than 24 hours was also significantly lower in the MCP group than in the UC group: 23% versus 35% (P < .01). There was a significant difference in surgical procedure between the MCP and UC groups, with more placement of prosthesis and dynamic hip screws in the MCP group for femoral neck and pertrochanteric fractures, respectively (Table 2). The length of stay was 19% shorter in the MCP group. The mean length of hospital stay was 9.7 (8.6) for the MCP group versus 12.0 (10.7) for the UC group (P < .01). In the MCP group, significantly more patients were discharged to a rehabilitation or nursing home, while significantly fewer patients were discharged to their own home, as compared to the patients in the UC group (Table 3).
Surgical Procedures in the MCP and UC Groups.

Abbreviations: MCP, multidisciplinary clinical pathway; UC, usual care.
Discharge Destinations in the MCP and UC Groups.
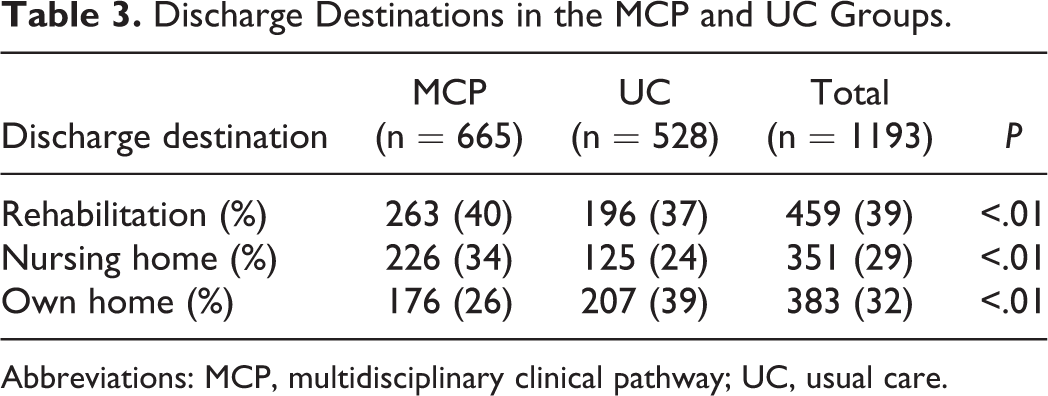
Abbreviations: MCP, multidisciplinary clinical pathway; UC, usual care.
Patient Outcome Measures
The incidence of postoperative complications was significantly lower in the MCP group (P < .01; Table 4). Postoperative delirium occurred less frequently in the MCP group than in the UC group (30% vs 37%; P = .02). No significant difference was observed in the incidence of postoperative stroke between patients in the MCP and UC groups. Mortality within 30 days after admission was not significantly different between the MCP and UC groups (overall mortality 6%).
Patient Outcome Measurements in the MCP and UC Groups.
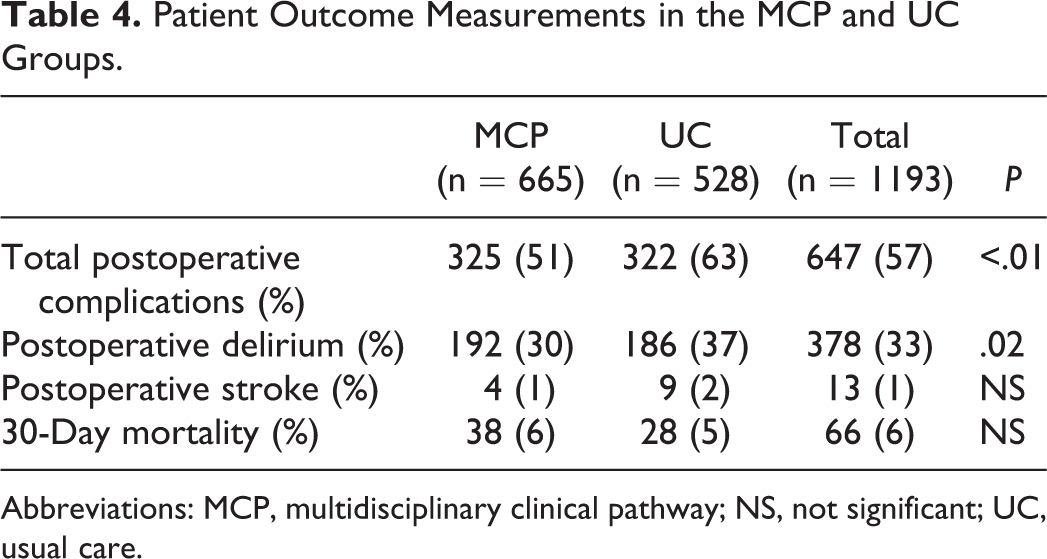
Abbreviations: MCP, multidisciplinary clinical pathway; NS, not significant; UC, usual care.
Discussion
This retrospective multicenter comparative cohort study found that the use of an MCP for patients with a hip fracture was associated with a reduced time to surgery, reduced postoperative complications, and reduced length of stay, while more patients were discharged to a nursing home compared to UC. There was no significant difference in 30-day mortality.
Recently, a number of studies have described the effect of implementing an MCP for patients with hip fractures 19 –25 (Table 5). In line with our data, these studies found that the MCP approach is associated with improved clinical outcome for these patients. Two studies found a reduced time to surgery using the MCP, 20,23 as was also found in our study, whereas 3 studies did not demonstrate such a reduction. 19,22,24 A number of factors (involvement of different specialism, shorter time to surgery, shorter length of stay, and the institutionalization) in our study could have contributed to the observed differences in the overall outcome. One of the factors in the MCP approach is the aim to limit the time to surgery, as an independent risk factor for in-hospital postoperative recovery, complications, and mortality. 26 Our study found that the use of the MCP approach was associated with a shorter time to surgery. Local inhibitory factors (eg, logistical factors inhibiting the time to surgery) probably limit the implementation of one of the main features of the MCP, which is operating on the patient within 24 hours, which means that the intended reduction in the time to operate is not achieved.
Overview of Literature on MCP Versus UC.

Abbreviations: LoS, length of hospital stay; No., number; NS, not significant; S, significant; TTS, time to surgery.
All studies 19 –21,23 –25 except one found a significantly reduced postoperative length of stay, 22 with reductions ranging from 8% to 45%. One study reported a length of stay after the implementation of MCP of 6.7 days, corresponding to a 33% reduction. An essential factor in the MCP is the logistic arrangements and agreements made to ensure early and timely discharge from the hospital to a nursing home. Indeed, our study found that more patients in the MCP group were discharged to a rehabilitation center or nursing home with rehabilitation facilities compared to the patients in the hospitals with UC.
The MCP group in our study showed a significantly lower complication rate compared to the UC group. Although 2 recent studies found similar differences, 19,22 3 other studies found no differences. 20,21,23 The main type of complication in the other studies was delirium and was therefore evaluated as a separate item. In our study, the overall rate of delirium as a complication was 33.1% of all cases. The MCP approach reduced the frequency of delirium significantly (30.3% vs 36.6%, P = .02). This could be explained by the use of preoperative consultations with a geriatrician and the standard implementation of screening and preventive measures.
There was no difference between MCP and UC as regard to the 30-day mortality rate. The mortality rates found in our study are comparable to those found in other recent studies. 19 –24,26,27 Although no significant differences in patient characteristics between the MCP and the UC groups were present in our study, the ASA classification was higher in the MCP group compared to other recent studies. 20,21 Apparently, the difference in comorbidities did not lead to a difference in mortality when comparing the different studies. In addition, we found a significant difference between the 2 groups with respect to the fracture type and operative procedure, with more femoral neck fractures in the MCP group. Although the findings of the various studies are not consistent, a considerable number of studies found no differences in outcome between patients with femoral neck fractures and those with intertrochanteric fractures, after correcting for age and comorbidities. 27,28
Our study, encompassing the largest cohort published until now, adds evidence to support the use of an MCP approach, with respect to logistic processes and clinical outcome parameters; although some comments need to be made on the interpretation of our findings, MCP is a set of measures to improve the logistics around the fragile patient with a fracture of the hip. Implementation of these measures might be different in all hospitals using MCP with varying results on the clinical outcome measures. This study was not designed as a clinical audit of differences in process parameters, so the exact underlying cause of the differences remains somewhat unclear. Further investigations on how and why the implementation of an MCP is effective are therefore warranted. In addition, no patient-reported outcome measures were taken into account nor were surgeon-oriented functional hip scores or generic health patient satisfaction scores. Whether an MCP approach results in better quality of life compared to UC remains to be investigated.
Conclusion
This retrospective multicenter comparative cohort study shows that the MCP approach for patients with a hip fracture is associated with a reduced time to surgery, reduced postoperative complications, and reduced length of stay; the institutionalization rate was significantly higher in the MCP group, without a significant difference in 30-day mortality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.