
Abstract
The elderly (age 70+) patient with orthopedic trauma is a rapidly growing subset of patients in the United States. Due to increased medical comorbidities and decreased physiological reserve, morbidity and mortality after trauma may significantly differ from those patients younger than 70 years old. A retrospective review was performed to investigate the effect of age on orthopedic trauma. A total of 870 records of patients with orthopedic trauma from 2006 to 2009 at our Level One trauma center were reviewed. A database was created to include demographics, type and number of comorbid conditions at presentation, injuries, intensive care unit (ICU) and hospital length of stay, and description of the fracture. Patients aged 70 years and older had an increased number of comorbidities per person (3.3214—P < .0001). Length of stay in patients aged 70 years and older was not significantly greater than that of the younger patients. They spent an average of 14.76 days in the hospital compared to 13.42 days for the combined younger patients (P = .45), but they spent significantly (P < .0001) more of their stay in the ICU (52.74% vs 34.9% for the younger cohorts). The number of fractures per patient was lower (1.66) in the 70 and older age-group when compared to younger populations (P < .0001). The 70 and older group was more likely to have their injury due to a fall and less likely to have solid organ injuries. As the number of elderly patients increase, continued research in the management of elderly patients with trauma can lead to protocols and practice guidelines to improve outcomes.
Introduction
The demographics of trauma are often focused on younger patients when in reality the elderly subset of this population makes up an overlooked yet important cohort. Although young adults still compose the largest proportion of patients with trauma, patients older than 65 are the fastest growing population group at trauma centers. 1 According to the National Trauma Database in the United States from literature in the 1990s, elderly patients (age 65+) with trauma account for 25% of all traumas. 2 -5 This is likely an underrepresentation of today’s population.
Previous studies have found that falls predominate the mechanism of injury for patients older than 65 years of age, 6 while motor vehicle accidents and penetrating injuries are the most common mechanisms in younger patients. 7 These results suggest that preventative methods can be targeted toward specific patient age-groups to reduce trauma occurrences. Although mortality does not differ between age-groups, time to death, if applicable, is often longer in the elderly patients. Younger patients with trauma will often die within the first 24 hours from the trauma itself, whereas elderly patients often die later due to secondary complications. Regardless of age, aggressive treatment can reduce risk of mortality by up to 50%. 8 Lehmann et al found that elderly patients were less likely to undergo rapid trauma evaluation and therefore less likely to have occult injuries identified in a timely fashion. 9
Elderly patients typically have more medical comorbidities. The presence of preexisting medical conditions independently increases mortality in patients with trauma 10 as well as length of stay (LOS). 11 By determining what comorbidities, types of injuries, complications, and outcomes that are associated with this population, a better understanding of the treatment and management of the elderly patient with trauma can be achieved. The purpose of this study is to investigate the effect of age on orthopedic trauma outcomes as it relates to LOS and proportion of stay in intensive care unit (ICU).
Methods
After approval from our institutional review board, medical records were retrospectively reviewed for patients managed by the orthopedic trauma service from 2006 to 2009. An extensive orthopedic-centered database was developed using the trauma database of a university American College of Surgeons (ACS)-certified Level One trauma center. Inclusion criteria were patients aged 18 years and older who were admitted to the inpatient general surgery trauma service after sustaining injuries that were eventually managed by the orthopedic trauma service. We excluded patients with isolated phalanx, spine, rib, facial, and skull fractures. Through this process, we identified 870 patients with complete records for review.
An extensive review of the electronic medical record was performed to create a database that included demographics, type and number of comorbid conditions at presentation, injuries, LOS in the ICU and hospital, and fracture descriptives. Demographic data collected included age, gender, height, weight, and ethnicity. Database composition was performed using FileMaker Pro Advanced (FileMaker, Inc, Santa Clara, California).
Age categories were based on the research of Caterino et al, which determines that the age of 70 is an appropriate upper limit for classification of elderly patients with trauma. 12 Ten-year cohorts were created for the rest of the ages with the exception of the youngest cohort, which included 18- to 29-year-old patients.
Statistical Analysis
Statistical significance was set as a P value less than .05. A Student t-test was used to compare the mean values for LOS, percentage of stay in the intensive care setting, and average comorbid conditions per person. The means were compared with patients aged 70 years and older with the collection of patients less than 70 years of age.
Results
Demographics and Comorbidities
Demographic data are provided in Table 1. Comorbidities and age were independently analyzed as well as LOS and percentage of the stay in intensive care. Patients aged 70 years and older had an increased number of comorbidities per person (3.3214—P < .0001) compared to younger age-groups. Hypertension, hyperlipidemia, and heart disease were far more common among patients older than 60 years as seen in Table 2.
Demographics and Outcomes Based on Age Cohorts.

Abbreviations: avg, average; ICU, intensive care unit; LOS, length of stay.
Medical Comorbidities Based on Age Cohorts.

Abbreviations: BMI, body mass index; COPD, chronic obstructive pulmonary disease.
Length of Stay and Percentage of Stay in Intensive Care
Length of stay in patients aged 70 years and older was not significantly greater than that of the younger patients. They spent an average of 14.76 days in the hospital compared to 13.42 days for the combined younger patients (P = .45). Upon further analysis, it was noted that the 60- to 69-year age-group had a significantly longer LOS than any other group with 20.3 average days in the hospital. When this group was analyzed independently, it was found that their LOS was significantly longer than all of the other groups (P < .0001).
Patients aged 70 years and older spent a significantly longer period of their time in an intensive care setting, 52.74% versus a cumulative percentage for the younger cohorts of 34.9% (P < .0001).
Mechanism of Injury
As seen in Table 3, mechanism of injury varied with age. Patients in the youngest age-group were most likely involved in motor vehicle collisions (MVAs), while most patients aged 70 and older (33%) sustained falls. The number of patients involved in a restrained MVA was similar regardless of age. In addition, patients in the 18 to 29 and 30 to 39 age-groups accounted for the greatest proportion of unrestrained MVAs (0.29 and 0.30, respectively).
Mechanism of Injury Based on Age Cohorts.
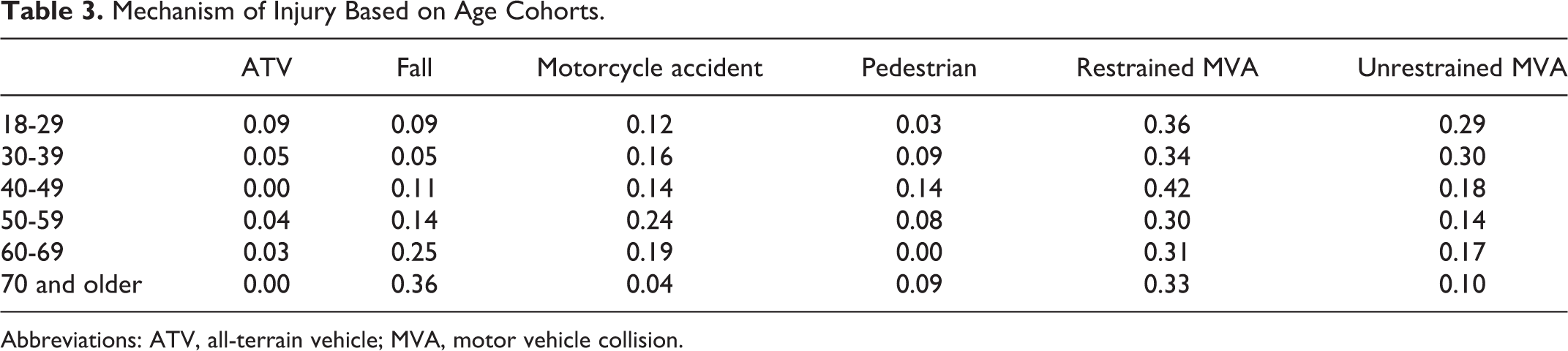
Abbreviations: ATV, all-terrain vehicle; MVA, motor vehicle collision.
Fractures
As seen in Figure 1, the number of fractures per patient was lower (1.66) in the 70 and older age-group when compared to younger populations (P < .0001).

Incidence of fractures in each age cohort.
Nonorthopedic Injuries
Figure 2 illustrates the distribution of nonorthopedic injuries among different age-groups. Solid organ injury rates are reduced in the elderly population. The other nonorthopedic injuries had no significant correlation with age.
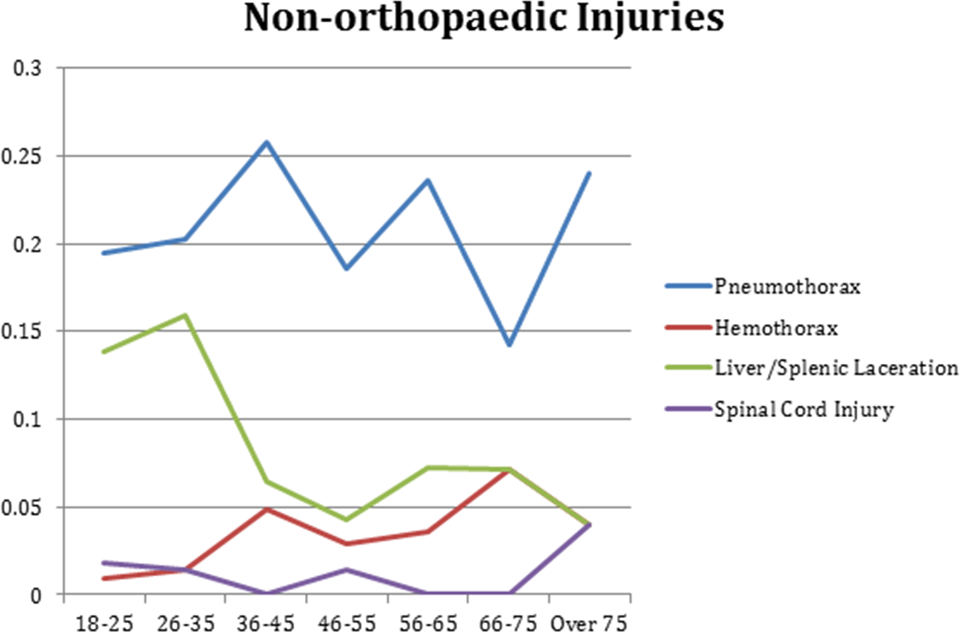
Incidence of nonorthopedic injuries in each age cohort.
Discussion
As the elderly population expands and health care spending continues to increase, it is essential for orthopedic trauma specialists to manage patients in a way to improve outcomes and minimize resource expenditures. This is especially true with the Baby Boomer population approaching their 70s. Patients older than 65 years are the fastest growing population group at trauma centers. 1
In our study, although the overall LOS did not vary significantly among age-groups—except for those aged 60 to 69—patients aged 70 years and older spent a significantly (P < .0001) higher proportion of their stay in the ICU (52%). As indicated in Table 2, this was most likely secondary to an increased rate of medical comorbidities that affects the patient’s physiological reserve. This was noted, despite the lower incidence of solid organ injuries in the elderly group. With a lower physiological reserve and medical comorbidities that make these patients more fragile, it is not surprising that these patients will take longer to stabilize to transition to a lesser level of care. Furthermore, elderly patients may have more unique social situations that lead to more complicated discharge planning like skilled nursing facility placement. This could have contributed to the overall length of hospital stay too. Perdue et al demonstrated that delayed deaths were more likely to occur in the geriatric population and that this population was more likely to have preexisiting renal, cardiovascular, and respiratory disease; the complications associated with this disease were often the reason for increased LOS and eventual mortality. 13 Since the overall mortality rate did not differ significantly, our study indicates the importance of aggressive medical management of elderly patients with orthopedic trauma and the need for protocols to address the increased risks for these patients. The management of these patients’ comorbid conditions cannot be overlooked as this is equally important as management of their orthopedic injuries.
Although the most common mechanism of injury in patients aged 70 and older was a fall (0.36), these patients had a similar incidence of restrained MVA (0.33). These patients also had a lower number of total fractures (P < .0001).
This study is limited in that it looks only at patients at 1 rural Midwest ACS Level One trauma center and may not be generalizable to urban trauma centers. Also, the selection of patients for this study was based on whether or not an orthopedic consultation was obtained and may have inadvertently overlooked the most severely injured patient. That is, patients with severe trauma who may have included orthopedic injury could have died before consultation and subsequently been omitted from the study. Continued research in the management of elderly patients with trauma can help us develop protocols and practice guidelines to improve outcomes.
Conclusion
Elderly patients, defined in this study as 70 years or older, have a larger percentage of their stay in the intensive care setting, fewer fractures and solid organ injuries, and more comorbid conditions. The LOS for patients older than 70 years of age was not significantly longer than the younger cohorts. However, in this study, the 60- to 69-year-old cohort had a significantly longer LOS compared to any of the other groups.
These data suggest that the elderly patient population with trauma is an important and expanding cohort to treat aggressively. The comorbid conditions that they possess affect their outcome and optimization of these conditions should be influential in their outcome. Continuing to refine trauma protocols that combine critical and surgical care with the input of medical services to comanage these comorbidities is necessary and offers opportunity for improved patient care and research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.