
Abstract
Associated fractures of the atlas and axis are frequent, particularly in the elderly patients following a simple low-energy fall. This injury can be easily misdiagnosed on initial plain radiographs, and therefore computed tomography scan is a useful adjunct in patients with a degenerative spine. There is still no consensus as to the optimal treatment of combined axis–atlas fractures, and the majority of authors propose a therapeutic strategy dependent on the odontoid fracture pattern. We describe a combined atlas and axis fracture in a 92-year-old patient who was managed with nonoperative treatment in a rigid collar. The association of C1 anterior arch with a C2 type II odontoid fracture is a rare combination, which to our knowledge has never been reported following nonoperative treatment. There was a good functional outcome at 1-year follow-up with the fracture progressing to a fibrous nonunion of the odontoid process.
Introduction
Associated fractures of atlas and axis, although frequent, are rarely discussed in the literature. The most common fracture pattern is a dens fracture associated with a C1 posterior arch fracture. These are more common in the elderly patients, in whom simple falls are the primary cause. Neurological impairment is a frequent finding with increased morbidity and requires emergent treatment. 1 Several authors have described missed diagnoses on initial radiographs, and therefore if in any doubt, additional studies are necessary. 1 -5 Computed tomography (CT) scan is very useful when investigating subtle, nondisplaced fractures or diagnosing associated fractures.
Case Report
A 92-year-old female patient attended the emergency department after sustaining a simple fall from standing, striking her face and forehead. On arrival to the hospital, she was hemodynamically stable and her Glasgow Core Score was 15, which was maintained throughout her stay. There was no loss of consciousness, and her major complaint was posterior neck pain accompanied with face and forehead pain. On examination, there was evidence of bruising over the forehead and nose. There was paraspinal tenderness on palpation over the cervical spine. There were no motor or sensory deficits on examination of the peripheral nervous system (upper and lower limbs). The patient had a past medical history of osteoporosis, hypertension with secondary myocardiopathy, cerebrovascular accident with ad integrum recovery, and bilateral total knee replacements.
Advanced Trauma Life Support (ATLS) protocols were followed, and a set of plain radiographs was taken, including cervical anteroposterior (AP) and lateral views. An AP open-mouth view was not possible to obtain due to concomitant facial trauma and difficulty in patient cooperation. The radiographs revealed a C2 type II fracture of the odontoid process according to Anderson and D’Alonzo classification 6 (Figure 1). The patient was admitted under the care of the medical team for further clinical evaluation following her traumatic head injury.

Lateral cervical radiograph taken at accident and emergency (A&E) at the time of presentation. C2 type II fracture is noted.
Orthopedic treatment was implemented with rigid immobilization using a cervical collar with occipital, sternal, and chin support (Figure 2).
As an inpatient, she underwent a CT scan of the cervical spine which revealed a fracture of the anterior arch of the atlas combined with the odontoid process fracture (Figures 3 and 4). A neurosurgical opinion was obtained and nonoperative treatment was advised, as the patient was considered not to be a surgical candidate due to her age and comorbidities. She was fully counseled with regard to her diagnosis, management options, and risks, including nonunion. She was keen to proceed with nonoperative management.

Picture of the patient with a rigid collar. Bruises noted over the face as a sign of the typical mechanism of injury: fall from standing with hyperextension.

Axial computed tomography (CT) image showing the anterior arch of the atlas fracture line.
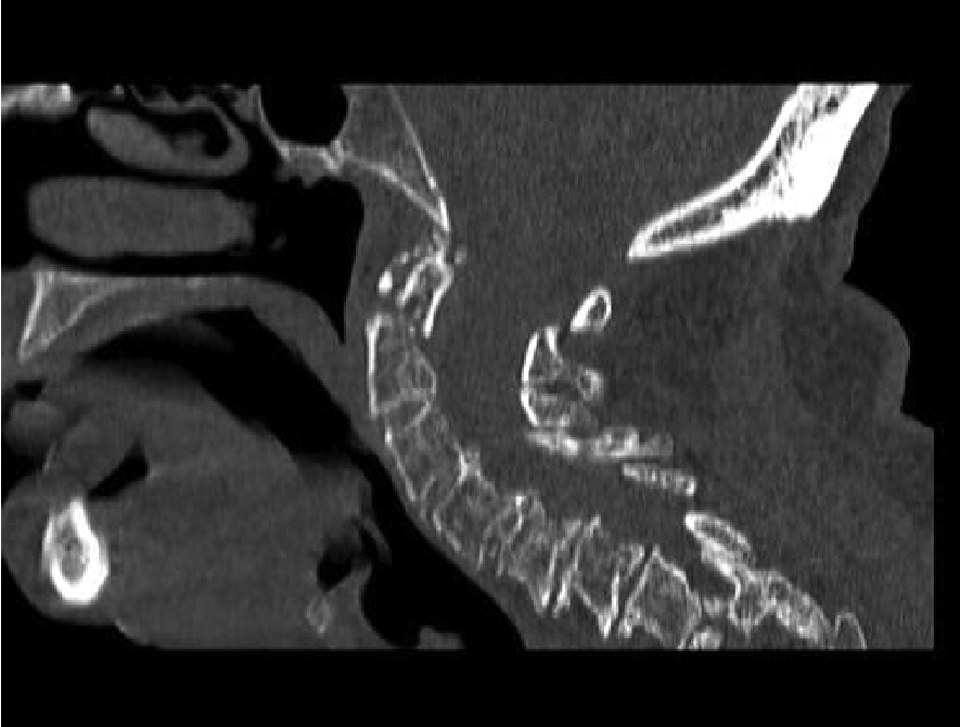
Sagittal computed tomography (CT) reconstruction showing the type II axis fracture.
The patient was discharged 2 days following her admission and was instructed to wear the collar for 10 weeks. At 6-week follow-up, she remained clinically stable with no neurological symptoms. She was complaining of moderate neck pain. Radiographs at this stage showed no further displacement of the fracture and no clear evidence of consolidation (Figure 5). Conservative treatment with continuation of the rigid collar for another 6 weeks was recommended. At further review, 15 weeks following the injury, there was evidence of axis dens nonunion (Figure 6), and she started physiotherapy under the care of the Rehabilitation team. At 1-year follow-up, the patient only described occasional mild pain and discomfort, similar to the chronic symptoms she had prior to her fall. Her range of movement was limited but also in a similar pattern. None of the symptoms were limiting her functionally, in particular for activities of daily living. She had no neurological deficits. Northwick park neck questionnaire undertaken a year from the fracture was 31.25% (100% as the worse result). 7
Institutional review board approval and patient’s consent were obtained for publication of this case report.

Lateral cervical radiograph 6 weeks following the fracture. No evidence of consolidation noted.

Lateral cervical radiograph taken at 15 weeks following the injury. Evidence of nonunion with sclerotic margins at both fracture ends.
Discussion
Combined fractures of atlas and axis vertebrae account for 3% of all acute cervical spine lesions, 12% of upper cervical lesions, 1 43% of atlas fractures, and 16% of axis fractures. 8 They most frequently occur in elderly patients resulting from a simple low-energy fall at home. An evaluation of odontoid fractures in the elderly patients found that with aging, severe degenerative changes develop in the atlanto-odontoid joint. These eventually obliterate the joint space and fix the odontoid to the anterior arch of the atlas. 9 Compared to isolated C1 or C2 fractures, a combined injury is more frequently associated with neurological impairment and increased morbidity, with a reported mortality of 80% to 85% at 1.5 months. 2,3 The mechanism of injury is usually spinal hyperextension with the most frequent lesion being an atlas fracture combined with type II odontoid fracture as was the finding in our patient. 10,11
The unique characteristics of this case are the fracture pattern involving the anterior arch of the atlas combined with the type II odontoid fracture, and its nonoperative management with good functional outcome at 1 year. Only 2 similar reports have been found in the literature. Guiot and Fessler reported 2 cases of anterior arch and type II odontoid fracture combination but in younger patients (51 years of age) treated operatively. 12 Korres et al reported a case of a double fracture of the odontoid process and anterior arch of the atlas in an elderly patient, but no follow-up was possible as the patient died of unrelated cardiopulmonary insufficiency after 10 days. 13
There are no high-level evidence studies evaluating the management of this combined fracture pattern. On the basis of a systematic review with level III evidence, recommendations for the treatment of combination atlas–axis fractures have been suggested to be based primarily on the specific characteristics of the axis fracture. Thus, external immobilization of most C1 to C2 combination fractures is recommended. Surgical stabilization and fusion should be considered for these cases with C1–type II odontoid combination fractures with an atlanto–dental ratio of ≥5 mm and C1–Hangman combination fractures with C2 to C3 angulation of ≥11. 14
Chapman et al in a retrospective review suggested a significant 30-day survival advantage for operatively treated over nonoperatively treated patients. The data also reported a trend toward the same results when longer term survival was analyzed. 15
The progression to nonunion of type II odontoid fractures has been extensively reported in the literature. 16,17 Therefore, surgical intervention is considered in young patients or elderly patients who are surgical candidates. Furthermore, the elderly population tolerate nonunion relatively well, and a fibrous union should provide sufficient stability, particularly in cases with minor trauma. 16,18 In a prospective study, Smith et al reported on the outcome among elderly patients with type II odontoid nonunion after nonoperative management of the acute fracture. They concluded that nonoperative treatment for type II odontoid fractures in the elderly patients has high rates of nonunion and mortality, although patients with nonunion did not report worse outcomes compared with those who achieved union at 12-month follow-up. However, 73% of patients with nonunion required delayed surgical treatment. 19 Our understanding is that in this reported case with a rare fracture pattern, the implications of nonunion were minimal for an elderly patient who had a premorbid baseline cervical functional limitation. Surgical treatment could be advocated in the elderly patients on the basis of recent studies, particularly because of better results with regard to short-term mortality and nonunion rates. 14,15,19 However, surgical treatment of type II odontoid fractures in these often medically compromised patients is also associated with adverse outcomes and major complication rate. 20 For these reasons, the optimal management of elderly patients with type II odontoid fractures in isolation or combined remains controversial. 21,22
The association of C1 anterior arch with a C2 type II odontoid fracture is a rare combination, which to our knowledge has not been reported following nonoperative management. We believe that the degenerative process visualized in the spine and a possible fusion between the dens and the anterior arch of the atlas may have played a role in the pathogenesis of this combined fracture as well as in the progression to nonunion.
Conclusion
Associated atlas–axis fractures are relatively frequent. The high association with neurological impairment and mortality places them as an emergency situation. They can be easily misdiagnosed on plain radiographs, and a CT scan is recommended if the diagnosis is in doubt, particularly in the elderly patients who sustain low-energy injuries. In this cohort of patients, the clinical significance of a chronic odontoid fracture nonunion appears to be limited.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.