
Abstract
Introduction:
The heath care system in the United States is in the midst of a transition, in large part to help accommodate an older and more medically complex population. Central to the current evolution is the reassessment of value based on the cost utility of a particular procedure compared to alternatives. The existing contribution of geriatric orthopedics to the societal burden of disease is substantial, and literature focusing on the economic value of treating elderly populations with musculoskeletal injuries is growing.
Materials and Methods:
A literature review of peer-reviewed publications and abstracts related to the cost-effectiveness of treating geriatric patients with orthopedic injuries was carried out.
Results:
In our review, we demonstrate that while cost-utility studies generally demonstrate net society savings for most orthopedic procedures, geriatric populations often contribute to negative net society savings due to decreased working years and lower salaries while in the workforce. However, the incremental cost-effective ratio for operative intervention has been shown to be below the financial willingness to treat threshold for common procedures including joint replacement surgery of the knee (ICER US$8551), hip (ICER US$17 115), and shoulder (CE US$957) as well as for spinal procedures and repair of torn rotator cuffs (ICER US$12 024). We also discuss the current trends directed toward improving institutional value and highlight important complementary next steps to help overcome the growing demands of an older, more active society.
Conclusion:
The geriatric population places a significant burden on the health care system. However, studies have shown that treating this demographic for orthopedic-related injuries is cost effective and profitable for providers under certain scenarios.
Introduction
In 1965, under President Johnson, the United States introduced Medicare with Title XVIII of the Social Security act in order to provide a government source of health care for people older than 65 years of age. 1 Since its introduction, health care has remained a moving target continuously evolving to new demands, insights, and stresses. Today, the United States is in the midst of an arguably equal shift in legislation with the Affordable Care Act, which has been met with similar concerns and resources. Unlike years past, technology has allowed for rapid data collection and analysis providing unprecedented insight into health care delivery. The plethora of new data has facilitated a reevaluation of health care and the concepts of increased cost consciousness, evidence-based approaches, and societal implications. This is especially true for a rapidly growing geriatric population that is living longer, stronger, and demanding more health care resources.
The Aging of America: The Silver Tsunami
In 2010, 13% of the population was older than 65 years of age. 2 This number is expected to increase to over 20% by 2040. Orthopedics as a specialty has evolved to serve a growing geriatric community. Subsequently, an influx of new technologies and scientific achievements has served to further increase surgical indications and surgical candidates beyond that of the population growth alone.
As shown in a report published by the American Heart Association in 2011, direct costs on health-related spending in the United States for osteoarthritis (US$42B) and back pain (US$30.5B) in combination are greater than that of diabetes (US$41.2B), hypertension (US$40.7B), and cerebrovascular disease (US$25.2B), areas usually considered the most threatening health issues facing the United States today. 3 Table 1 shows the cost and volume of some common orthopedic procedures. As the population ages, the number of orthopedic procedures is expected to increase at an alarming rate. 9
Costs and Volume of Common Orthopedic Procedures.

a 2011 Agency for Healthcare Research and Quality (AHRQ) data. 4
The role of orthopedics in health care requires careful consideration, study, and recalculation. Historically considered a field of simply repairing broken bones and replacing arthritic joints, the implications of today’s orthopedic practice carry too large an economic and societal cost to remain stagnant. As stated eloquently by Dr John Tongue, president of the American Academy of Orthopaedic Surgeons (AAOS), “For everyone’s sake, the definition of value must not be dictated by the sticker price of the orthopedic procedure or treatment. We also need to consider patients’ ability to remain independent and productively employed, as well as the reduction or elimination of payments for disability or long-term care.” 10 Stated differently, leading researchers identify the triple aim approach as the forefront of health system change: innovations must improve the patient experience of care, improve the health of the population, and reduce per capita cost. 11
Cost-Effectiveness, Cost-Utility Analysis, Quality-Adjusted Life Years
Cost-effective (CE) analysis at the highest level is a form of economic analysis that weighs the relative costs and outcomes of 2 or more options. This concept has been applied to many types of organizations and activities. This idea as it pertains to health care today was really defined by Gold and Weinstein in the 1990s. 12 In their model, the decision to invest in a health care intervention was determined by the calculation of an anticipated health benefit that exceeded the total costs. For example, the denominator is a gain in health (years of life, improved functional score, and improved reproductive success) and the numerator is the cost required to obtain the gain. Gold and Weinstein also recognized that any health-related decision must be weighed against other social investments such as education and government, among others. Moreover, the perspective of the beneficiary, provider, and payee must also be considered. For example, in the context of geriatric orthopedics, resources dedicated to older individuals absorb funds from children with birth defects, adults with acute athletic injuries, or other areas of health in general (cardiology, endocrine, etc). Similarly, although an outcome of increased life years may play an important role in decision making for an older patient, it has little impact on a young college athlete wishing to return to competition following an acute injury.
A subset of CE analysis is the idea of cost-utility analysis, which was designed to encompass the diverse effects of a single intervention and to compare interventions with different kinds of outcomes, in turn addressing in some respect the idea of perspective. Cost utility is grounded on a ratio between the cost of a health-related intervention and the value it produces in terms of the number of years lived in full health by the beneficiaries. A summary measure of health in the form of quality-adjusted life years (QALYs) has become the crux for cost-utility analysis. 13 Despite a long-standing role in health care literature since the 1950s, the idea of utilizing QALYs for assessing the economics of orthopedic practice has only more recently penetrated orthopedic forums. 14
Quality-adjusted life years in simplest terms is the measure of disease burden that takes into account the quality of life as well as the quantity of life following an intervention.
13
Values are assigned to quality of life based on the theoretical utility of a person. For example, a year lived in perfect health is given an index value of 1. Thus, postintervention, the quality of life is multiplied by the expected number of life years to obtain the QALY.
Quality-adjusted life yearshas been used by several authors recently to compare utilization of resources for various procedures and patient populations.
15
Moreover, by considering the cost (direct and indirect) of a particular procedure, comparisons can be made between the ratio of cost to QALY, often expressed as incremental cost-effectiveness ratio (ICER). For example, if 2 procedures net a QALY of 2, but procedure A costs 50% less than procedure B, the ICER will be half, suggesting a better investment, given fixed resources. Alternatively, the CE ratio can be calculated, which is the cost for each QALY gained, although this ratio does not compare across 2 alternatives.
where i = intervention state and c = control state.
Cost Utility for Orthopedic Procedures in the Geriatric Population
Historically, the ratio involving costs and effectiveness is compared to a willingness to pay threshold (WTP) in order to standardize whether an intervention is worthy of societal resources. 16 In 1982, Kaplan and Bush proposed a US$50 000/QALY threshold for determining cost-effectiveness. 17 Since its introduction, WTP has undergone many iterations and proposals, including the debate over the necessity for a dynamic threshold that includes variables such as inflation. 18 Nevertheless, especially given the costs associated with elderly health care, the geriatric community has been a focus of cost-effectiveness analysis with WTP as a common guideline. A number of studies have reviewed orthopedic interventions and the impact of such procedures on societal and institutional value. We performed a literature search including only articles that noted a specific focus on geriatric populations exclusively, commented on geriatric populations separately from the larger population, or studied a total sample population that averaged over 65 years of age. Overall, the findings cast geriatric orthopedics in a similar class to more traditional life-saving procedures in terms of societal value, however, also recognize a number of factors that impact institutional compensation.
Societal Value
A landmark study completed by Losina et al on total knee arthroplasty (TKA) established a useful model for cost-utility analysis 19 (Table 2). Using a Markov model, Medicare-aged patients were assessed for the cost-effectiveness of TKA as related to patient’s risk and hospital volume. Overall, TKA increased QALY by 1.1 versus nonoperative treatment, with an ICER of US$18 300. Not surprisingly, QALY for high-risk patients was reduced to 0.8; however, an ICER of US$28 000 remained under the WTP of US$50 000/QALY. It was also noted that rising costs and ICER was indirectly related to hospital volume such that a hospital performing more joints did so at a lower cost–QALY ratio.
QALY and Cost-Utility for Orthopedic Procedures Performed on Geriatric Populations.
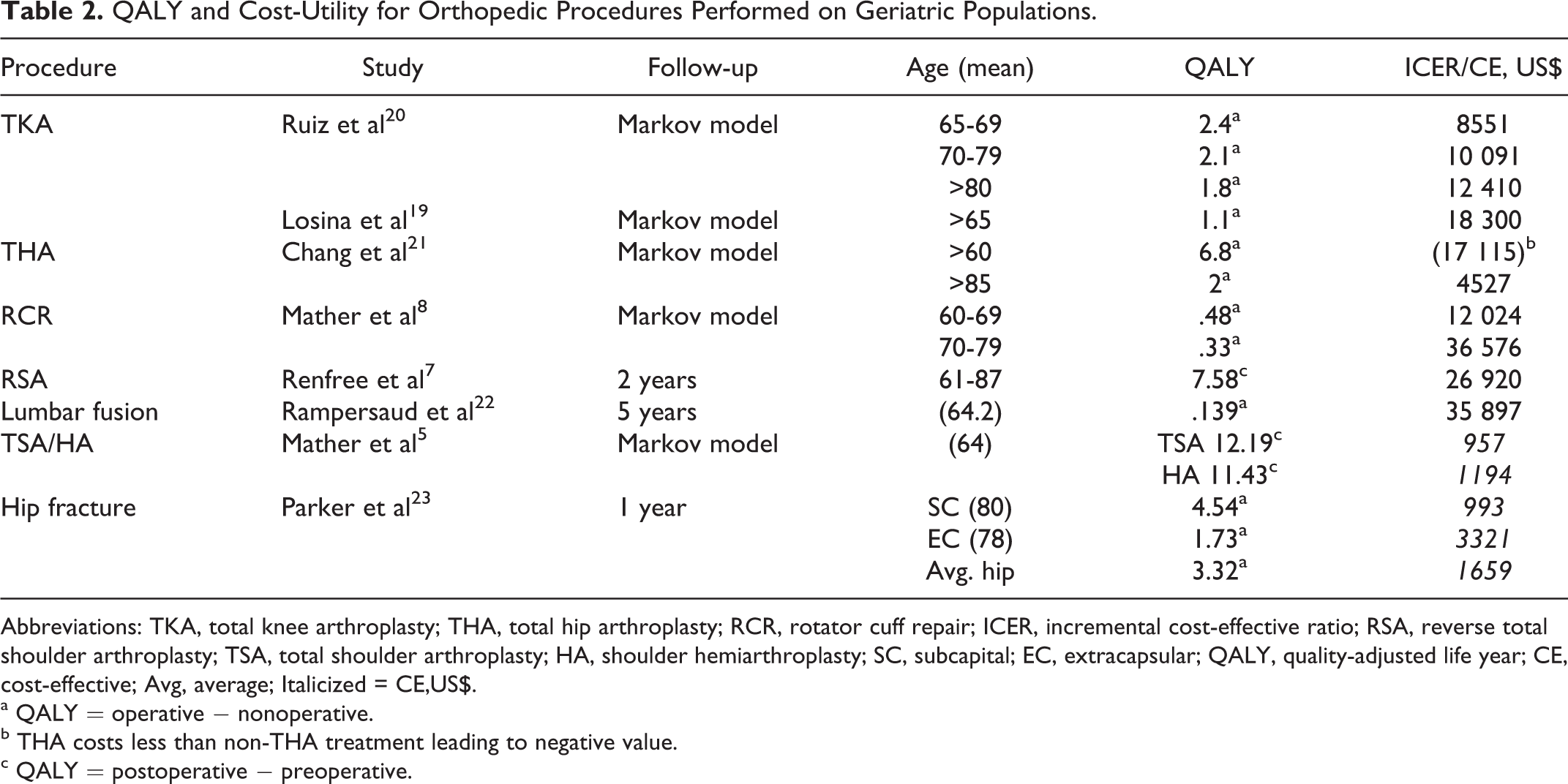
Abbreviations: TKA, total knee arthroplasty; THA, total hip arthroplasty; RCR, rotator cuff repair; ICER, incremental cost-effective ratio; RSA, reverse total shoulder arthroplasty; TSA, total shoulder arthroplasty; HA, shoulder hemiarthroplasty; SC, subcapital; EC, extracapsular; QALY, quality-adjusted life year; CE, cost-effective; Avg, average; Italicized = CE,US$.
a QALY = operative − nonoperative.
b THA costs less than non-THA treatment leading to negative value.
c QALY = postoperative − preoperative.
A similar study of TKA completed as part of an initiative supported by the AAOS drew comparable findings. Employing a Markov model, Ruiz et al showed that QALY increased for all ages compared to nonoperative treatment. 20 It was also noted that after 70 years of age, patients’ total lifetime societal savings was negative, reflective of a decrease in the accrued working years and increased salaries observed in younger cohorts. Nevertheless, consistent with earlier studies, the ICER remained below the WTP, leading the authors to propose that TKAs across all populations lessen the societal burden of disease.
Chang et al in 1996 examined elderly patients in regard to the ICER of total hip arthroplasty (THA). 21 Functional status according to the American College of Rheumatology was referenced to measure effectiveness, and direct and indirect costs were gathered from local teaching hospitals. The study reported that ICER increases with age, especially for men compared to women. In the best-case scenario as defined by a 60-year-old white women, QALY was increased 6.9 years compared to nonoperative treatment. However, a male older than 85 years gained a QALY of 2 years with an ICER of US$80 000. Despite the higher ICER, the authors highlight that at the time of publication, this value was US$4600 less than coronary bypass surgery or renal dialysis dependence, suggesting that in comparison to other life-extending procedures, THA was cost effective. Other studies have reached similar conclusions in regard to the favorable cost utility of hip and knee arthroplasty compared to nonorthopedic procedures. 24
Surgical treatment of rotator cuff tears follows the trend observed with other orthopedic procedures as being CE treatments. Mather et al, 43 using a similar model to Ruiz et al, 20 found that QALY for patients undergoing arthroscopic or open repair for rotator cuff tears exceeded that of a comparable population continuing with nonoperative treatment. However, an age-related decline in net society savings was observed with an inflection at 61 years of age favoring nonoperative treatment. The authors do point out that ICER remained under US$50 000 regardless of age, a favorable observation for continued advocacy of operative repair when indicated.
Another rapidly growing procedure in orthopedics, total shoulder arthroplasty (TSA), has also been investigated in the geriatric population. Mather et al compared TSA and hemiarthroplasty (HA) for the treatment of glenohumeral osteoarthritis in 64-year-old patients. 5 A Markov model was constructed to compare the following 2 scenarios: (1) TSA had a 5% increase in quality of life and utility over HA and (2) equal quality of life and utility between the 2 methods. In either case, TSA demonstrated to be a dominant option with higher QALY pre- and postoperatively as well as lower ICER. As an alternative option, Renfree et al found that the cost-effectiveness of reverse shoulder arthroplasty remained under the WTP and matched those of TKA and THA procedures. 7 In patients aged 61 to 87 years, it was found that in comparison to a preoperative QALY of 6.13, postoperatively at 2 years, a QALY of 8.10 was achieved. The cost per QALY was between US$26 930 and US$16 747 at 2 years, depending on the utility tool used for calculation.
Although hip fractures represent a major component of geriatric orthopedic care, a review of the literature yielded few studies exploring QALY-based economic analysis of hip fracture care. Alternatively, health-adjusted quality life years 25 in relation to costs have been utilized extensively to show that total hip replacement is more CE than internal fixation for displaced intracapsular hip fractures in healthy and cognitively intact elderly patients. 26,27 In one of the few to use QALY, Parker et al provide a comparison of operative versus conservative treatment. 23 In their study, displaced subcapital fractures (QALY 4.547, US$cost/QALY 594) were fixed with HA or reduction and internal fixation. Extracapsular fractures (QALY 1.735, US$cost/QALY 1986) were fixed with a dynamic hip screw. Based on the differences in QALY and US$cost/QALY between operative and surgical intervention, surgical fixation was recommended for displaced subcapital fractures and extracapsular fractures. However, conservative treatment was preferred for nondisplaced subcapital fracture. However, these results should be utilized with caution, as surgical fixation of hip fractures may be an important quality of life-preserving intervention for appropriately selected patients.
Studies investigating other principal procedures for the geriatric populations are available; however, such projects are generally not limited to elderly patients. For example, Rampersaud et al compared the cost utility of lumbar spinal fusion for patients with lumbar spinal stenosis in relation to hip and knee arthroplasty for the treatment of OA. 22 Across a patient population between the ages of 42 and 84 (mean 64.2), 5-year incremental cost utility was US$12 271/QALY for spinal decompression and US$35 897/QALY for spinal decompression with fusion. When predicted over a lifetime, the ICURs decreased to US$2994 and US$10 806, respectively. The authors note that even despite failure rates associated with fusion, the best- (US$3613/QALY)- and worst-case (US$39 323/QALY) scenarios were still in line with THA and TKA for the treatment of OA.
Institutional Value
At the center of the geriatric epidemic are providers tasked to care for a population that is inherently complex and costly to care for. In 2040, spending on fragility fractures is expected to exceed US$240 billion. 28,29 The specialty of geriatric medicine has successfully demonstrated that heightened acuity to elderly-specific disease states can significantly improve outcomes while reducing costs. 30,31 With these principles in mind, center-specific changes as well as new methods for sharing the burden across the community have proven fruitful. 32,33
One of the most effective center-specific changes includes comanagement teams comprising specialty-trained geriatricians, internists, and orthopedic surgeons which has been shown to reduce costs, 34,35 lessen complication rates, 36 and reduce length of stay. 37 More streamlined approaches to shorten delays in operative intervention have similarly resulted in costs reduction and improved outcomes. 38,39
Reworking how a region triages hip fractures has also demonstrated potential for reducing costs and improving outcomes. This was investigated recently by Clement et al when testing 3 different service models for treating hip fractures. 40 When comparing a typical fracture program in the United States versus a high-volume, low-cost fracture tertiary center and an urban tertiary care academic center with no formal fracture center, 3 important finding were exposed. First, it was found that profit was directly related to volume with a minimal threshold required to maintain profitability—which is essential in today’s health care economy. Second, increases in volume were more lucrative than reductions in cost. Finally, comanagement led to shorter delays to the operating room and more rapid discharges, both of which translated to increased cost-effectiveness. Such findings argue in favor of wide-sweeping changes to high-volume models, but more data are still needed before implementing large-scale changes. 41
Next Steps
Prevention of disease has long been backed as a key focus of health care reform. Within orthopedics, studies have both promoted the effectiveness and cost utility of preventative measures geared toward increasing bone mineral density among others. 42 Retrospective studies have supported that physical therapy can help reduce the burden of osteoporotic-based fragility fractures. 44 –46 However, this seems to have a greater impact on the weight-bearing skeleton. 47 Fortunately, pharmacologic therapy has shown promise for reducing fracture risk of weight-bearing and nonweight-bearing patients with low bone mineral density. 48
Resources have also been directed toward improving CE treatment with positive results. Surgical techniques have been reworked to reduce factors that lead to decreased operative time and complications. 49 Postoperatively, studies have explored rehabilitation protocols to reduce hospital length of stays as well as accelerate time to achieve preinjury levels of function. 50,51 Studies on nutritional supplementation postoperatively seem to yield positive results and potentially provide a cost-saving strategy to consider. 52,53
Limitations of Utility and CE Analysis
Despite its common implementation in the literature, QALY-based assessment is not without criticism. 54,55 Inherent to the calculation is the argument that it is a quasi-utilitarian calculus to decide which patients receive treatment. 54 Critics argue that severe illness should be prioritized over patients with less disability, and not all patients have the same potential to get better. Some studies have addressed this issue by dividing population samples into high- and low-risk groups. Others have argued that cost analysis fails to capture intangible aspects of disease such as the emotional impact of the individual as well as the family members, which may lead to secondary losses. Controversy has reached such a level that the European Consortium in Healthcare Outcomes and Cost-Benefit research (ECHOUTCOME) released its recommendation against using QALY in health care models because of too many invalid assumptions. 56,57 Nevertheless, cost-utility analysis including QALY continues to be infused into the health economic literature and remains a work in progress much like the problems its designed to help solve. 58
Conclusion
Orthopedics has a major impact on the economy due to the large prevalence of musculoskeletal disease and the associated high burden of disability. As health care reform undergoes its latest transition, direct and indirect costs are receiving greater consideration, especially in relation to corresponding changes in health. In light of these recalculations, geriatric orthopedics provides a high-yield area for investigation and reform. Although cost-utility studies have demonstrated net society savings for most orthopedic procedures across all ages, geriatric populations often contribute negatively, despite positive QALY and ICER below the WTP. However, models utilizing QALY and ICER calculations do not take into account individual patients’ characteristics and we must remember that our aging population of active patients often benefit greatly from orthopedic interventions, even well into advanced age. Recent studies have identified a number of opportunities for improved optimization and efficacy in treating this population including disease prevention, new technology, and recalibrated workflows utilizing geriatric comanagement. Further studies on economic value will help reduce the gap between today’s inefficiencies and the penultimate goal of improved outcomes at a lower cost.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.