
Abstract
Introduction:
There are risk factors associated with mortality in patients older than 70 years with hip fracture, including kidney function. However, indirect formulas to calculate glomerular filtration rate are not validated in patients older than 70 years. We analyzed whether the formula hematocrit, urea, and gender (HUGE) can be used as a prognostic factor.
Material and Methods:
A retrospective cohort study of 88 patients older than 70 years with a diagnosis of hip fracture. At admission, clinical and biochemical parameters were measured and glomerular filtration rate by Cockcroft-Gault, Modification Of Diet In Renal Disease (MDRD), Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI), and HUGE value. Accuracy to assess long-term mortality was analyzed with receiver–operating curve analysis. Cox regression analysis was performed to identify risk factor for mortality.
Results:
Sample included 88 patients; overall mortality was 13.63%, 17.85%, 28.57%, and 75.85% at 6 months, 1, 2, and 3 years, respectively. There was no significant difference in glomerular filtration rate by different formulas, contrary to HUGE, with higher values in the mortality group (1.83 ± 6.38 vs −2.61 ± 2.70, P = .0001). Survival was lower in patients with higher HUGE values (22.7 months, 95% confidence interval [CI] 16.1-29.5 vs 32.9 months, 95% CI 30.2-35.7; P ≤ .001). In the Cox regression analysis, a negative HUGE value is associated with lower mortality (hazards ratio = 0.238; 95% CI 0.568-0.099).
Conclusion:
The HUGE formula is an independent risk factor for mortality in elderly patients with hip fracture, but not the glomerular filtration rate determined by Cockcroft-Gault, MDRD, and CKD-EPI.
Introduction
Approximately 30% of the older adults living in the community have a fall each year, with the rate being more frequent in institutionalized patients. 1 The propensity for fall-related injury in elderly persons is related to a high prevalence of clinical disease and age-related physiologic changes that make even a mild fall particularly dangerous. Although most falls produce no serious injury, between 5% and 10% of community-dwelling older persons who fall each year sustain a serious injury. 2 As the number of older adults increases, it is expected that the annual incidence of hip fracture will exceed 7 million over the next 40 to 50 years. 3 Among the geriatric population, hip fracture is associated with a mortality rate of 14% to 36% and with temporary or permanent high levels of dependence on assistance with the activities of daily living.
Several risk factors have been shown to influence mortality after surgery for hip fracture, including the presence of more than 3 comorbidities, ischemic heart disease, chronic pulmonary disease, pneumonia, duration of surgery, sex, being a nursing home resident, and a creatinine level greater than 1.69 mg/dL. Other factors include the serum levels of sodium, potassium, urea, and creatinine at admission. 4
The kidneys undergo a number of involutive changes associated with aging that maintain the balance of the internal environment, although their ability to adapt to any biological stress is limited compared to that in healthy adults. 5 The structural and functional changes that appear in the aged kidney can be classified into the following 6 categories: vascular alterations, renal tubular dysfunction, tubular fragility, medullary hypotonicity, urinary obstruction, and senile hypofiltration. 6 -8 It is known that the glomerular filtration rate (GFR) decreases with aging at a rate of 0.75 to 1 mL/year. However, this decrease does not correspond to serum creatinine levels, making it difficult to assess kidney dysfunction in this group of patients. 9,10
There are several formulas that use blood creatinine together with other factors including age, sex, weight, and height to calculate the GFR. However, validation of these is limited in people older than 70 years, and the prognostic implications of these surrogate markers of kidney function are not well determined. 11
The hematocrit, urea, and gender (HUGE) formula was designed to differentiate age-related renal changes from chronic renal failure in patients older than 70 years 12 and has been validated as a prognostic indicator in patients with diabetic nephropathy. 13
The aim of this study was to analyze whether the indirect measurement of renal function by the HUGE formula is useful as a prognostic indicator in older patients with hip fracture.
Materials and Methods
This is a retrospective cohort study of patients with diagnosis of hip fracture who were hospitalized at academic hospital in Mexico City.
All patients older than 70 years with hip fracture between January 2008 and January 2012, community dwelling or institutionalized and undergoing any therapeutic modality (conservative or surgical), were included. A telephone interview was conducted with patients or family members to determine their current health status and, in those who had died, to identify the date of death. The exclusion criteria were patients treated only in the emergency department who were hospitalized for less than 24 hours, patients with recurrence of fracture or previous hip surgery, patients with dislocation of a hip prosthesis, and patients for whom we did not have sufficient location data or who refused to provide information by telephone interview.
We assessed the hip fracture type at admission, when surgical or conservative treatment was performed, operative time, type of anesthesia, and biochemical parameters at admission including hemoglobin, hematocrit, blood urea nitrogen (BUN), and creatinine. Finally, we calculated the GFR and the HUGE values.
Indirect Assessment of Renal Function
The GFR was calculated based on demographic and biochemical variables using the following formulas: Cockcroft-Gault: ([140 − age [years] ×bodyweight [kg]/[72 × serum creatinine [mg/dL]]), ×0.85 if female 14 ; Modification Of Diet In Renal Disease (MDRD): 186 × serum creatinine−1.154 × age −0.203 (× 1.212 if African American), ×0.742 if female 15 ; Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI): 141 × min (SCr/K,1)a × max(SCr/K,1)−1.209 × 0.993Age (×1.018 if female), ×1.159 if African American 16 , where SCr is serum creatinine (mg/dL), k is 0.7 for females and 0.9 for males,a is −0.329 for females and −0.411 for males, min indicates the minimum of SCr/k or 1, and max indicates the maximum of SCr/k or 1.
Hematocrit, Urea and Gender
The HUGE is calculated as 2.505458 − (0.264418 × hematocrit) + (0.118100 ×urea), +1.383960 if male, 12 where if the result is <0, the individual is not renal insufficient and if the result is >0, the patient has a high probability of developing chronic renal failure.
Statistical Analysis
Continuous variables are described as mean and standard deviation, and categorical variables are presented as number and percentage. Continuous variables were compared using Student t test or Mann-Whitney U test; categorical variables were compared using chi-square or Fisher exact tests. Overall survival was analyzed with Kaplan-Meier curves, stratified by various indirect markers of renal function. We identified covariates associated with overall long-term mortality and adjusted for these using Cox regression. Comparative analysis of the area under the receiver–operating characteristic (ROC) curve (AUC) for the surrogate markers of renal function, for prediction of mortality, was performed. A linear regression analysis was made between the values generated from the HUGE formula and the other noninvasive markers of renal function (Cockcroft-Gault, MDRD, and CKD-EPI). A P value ≤ .05 was considered significant, and the inclusion of covariates in the Cox model was considered at a P value ≤ .1. All analyses were performed with SPSS for Windows v 16.0 (SPSS Inc, Chicago, Illinois). The study was performed in accordance with the declaration of Helsinki and was approved by the ethics committee at hospital.
Results
The study initially included 106 patients 70 years or older who were hospitalized with a diagnosis of hip fracture in the period January 2008 to January 2012. In all, 16 patients were excluded because of inadequate contact details, and 2 because of refracture/readmission, and the final study cohort consisted of 88 patients (Figure 1).
Flowchart of study design.
Demographics
The baseline characteristics of the study population are shown in Table 1. The average age was 83 with a range of 71 to 98 years and a predominance of women (75%). The average level of education was 6.8 years with a range of 0 to 20 years. Only 3 (3.40%) patients were in nursing homes. Forty percent of patients had low morbidity according to the Charlson index; it is noteworthy that 4 (4.5%) patients entered the study already diagnosed with chronic renal failure. The mean creatinine and BUN were 0.96 ± 0.77mg/dL and 21.54 ± 13.62mg/dL, respectively. The mean GFR calculated by Cockcroft-Gault, MDRD, and CKD-EPI formulas was 54.11 ± 23.39 mL/min, 78.60 ± 31.3 mL/min, and 66.41 ± 21.08 mL/min, respectively; the mean HUGE value was −1.51 ± 4.37. Most patients had a GFR between 60 and 89 mL/min, 31.8% of patients had a GFR of <60 mL/min. Of the patients with a negative HUGE, 29 (43%), 60 (89%), and 54 (81%) had a GFR >60 mL/min, and of those with positive HUGE value, 18 (86%), 14 (67%), and 15 (21%) had a GFR <60 mL/min, according to Cockcroft-Gault, MDRD, and CKD-EPI values, respectively.
Baseline Characteristics of Patients With Hip Fracture.a,b

Abbreviations: MDRD, Modification Of Diet In Renal Disease; CKD-EPI, Chronic Kidney Disease Epidemiology Collaboration; HUGE, hematocrit, urea and gender.
an = 88.
bData are expressed as mean ± standard deviation, or number (%).
Overall mortality in the study population was 13.63%, 17.85%, 28.57%, and 75.85% at 6 months, 1, 2, and 3 years, respectively. Mortality was associated with lower hemoglobin, hematocrit, and body mass index and increased BUN and creatinine. There was no significant difference between the survival status for GFR calculated by any of the different formulas (Cockcroft-Gault, MDRD, and CKD-EPI). In contrast, the average HUGE value in the nonsurvivor group was 1.83 ± 6.38 compared with −2.61 ± 2.70 for survivors, P < .001 (Table 2).
Characteristics According to Overall Survival Status.
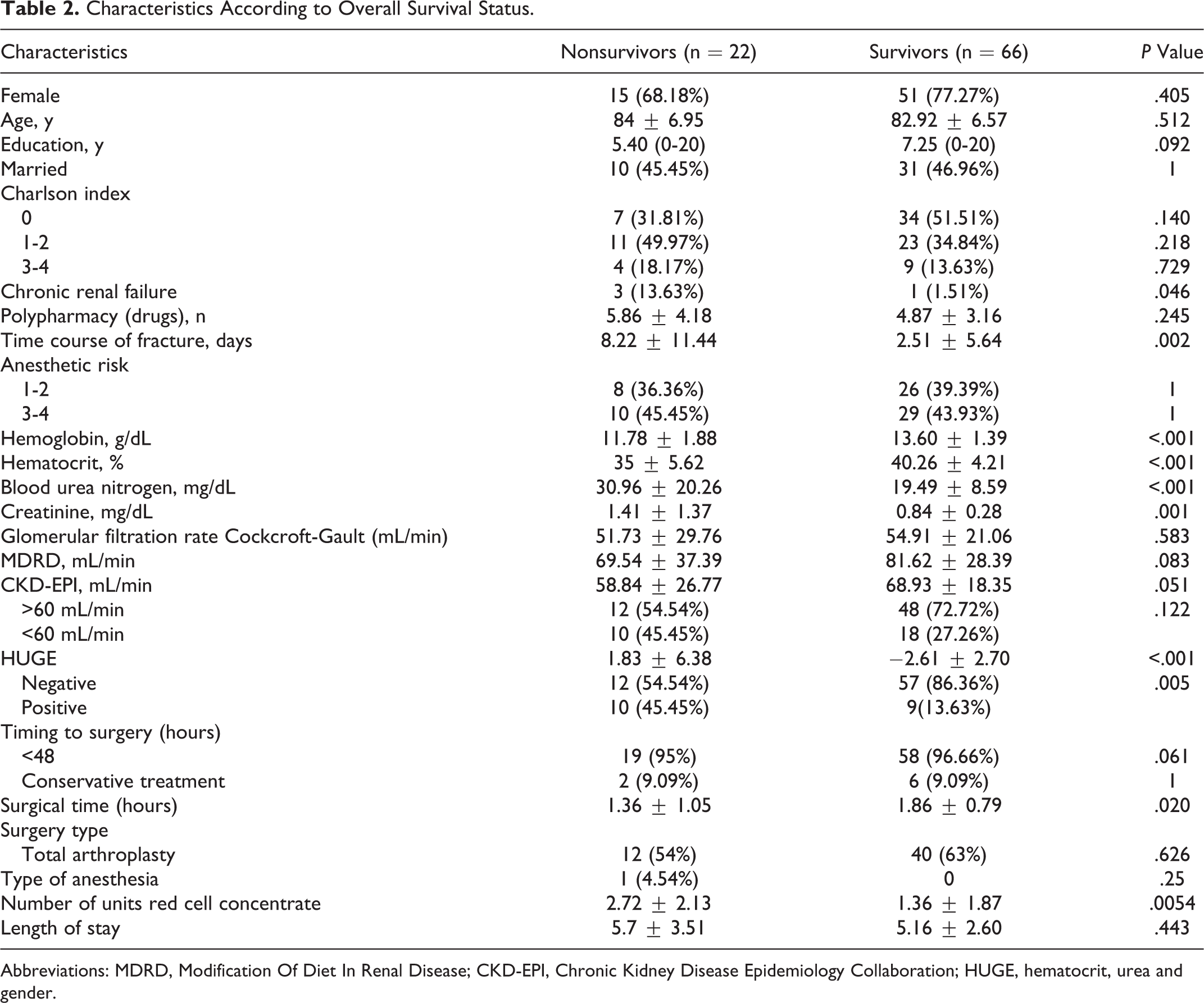
Abbreviations: MDRD, Modification Of Diet In Renal Disease; CKD-EPI, Chronic Kidney Disease Epidemiology Collaboration; HUGE, hematocrit, urea and gender.
Duration of survival differed according to the HUGE value, being 22.7 months (95% confidence interval [CI] 16.1-29.5) for positive HUGE value versus 32.9 months (95% CI30.2-35.7) for negative HUGE value, P < .001 (Figure 2). In the Cox regression analysis, a negative HUGE value was associated with lower mortality (hazard ratio [HR] = 0.238; 95% CI 0.568-0.099).

Cox regression analysis of mortality according to hematocrit, urea, and gender (HUGE) value; P < .001.
We performed the same analysis of survival using other indirect markers of renal function. The mean survival for patients with kidney dysfunction (GFR < 60 mL/min) according to the formulas was 32.1 months (95% CI 27.9-36.5) versus 30.4 months (95% CI 27.7-33.2), P = .18, for Cockcroft-Gault; 23.2 months (95% CI 16.5-29.9) versus 32.4 months (95% CI 29.7-35.2), P = .005, for MDRD; and 26 months (95% CI 20.4-31.6) versus 32 months (95% 29.0-35.0), P = .099, for CKD-EPI.
The ROC analysis to assess the accuracy for predicting mortality of each of the formulas used to indirectly measure renal function showed that HUGE has the highest AUC of 0.780 (95% CI 0.667-0.892; Figure 3).The CKD-EPI has the strongest correlation with HUGE (r = .611), followed by the MDRD (r = .547), with Cockcroft-Gault (r = .476) having the weakest correlation.
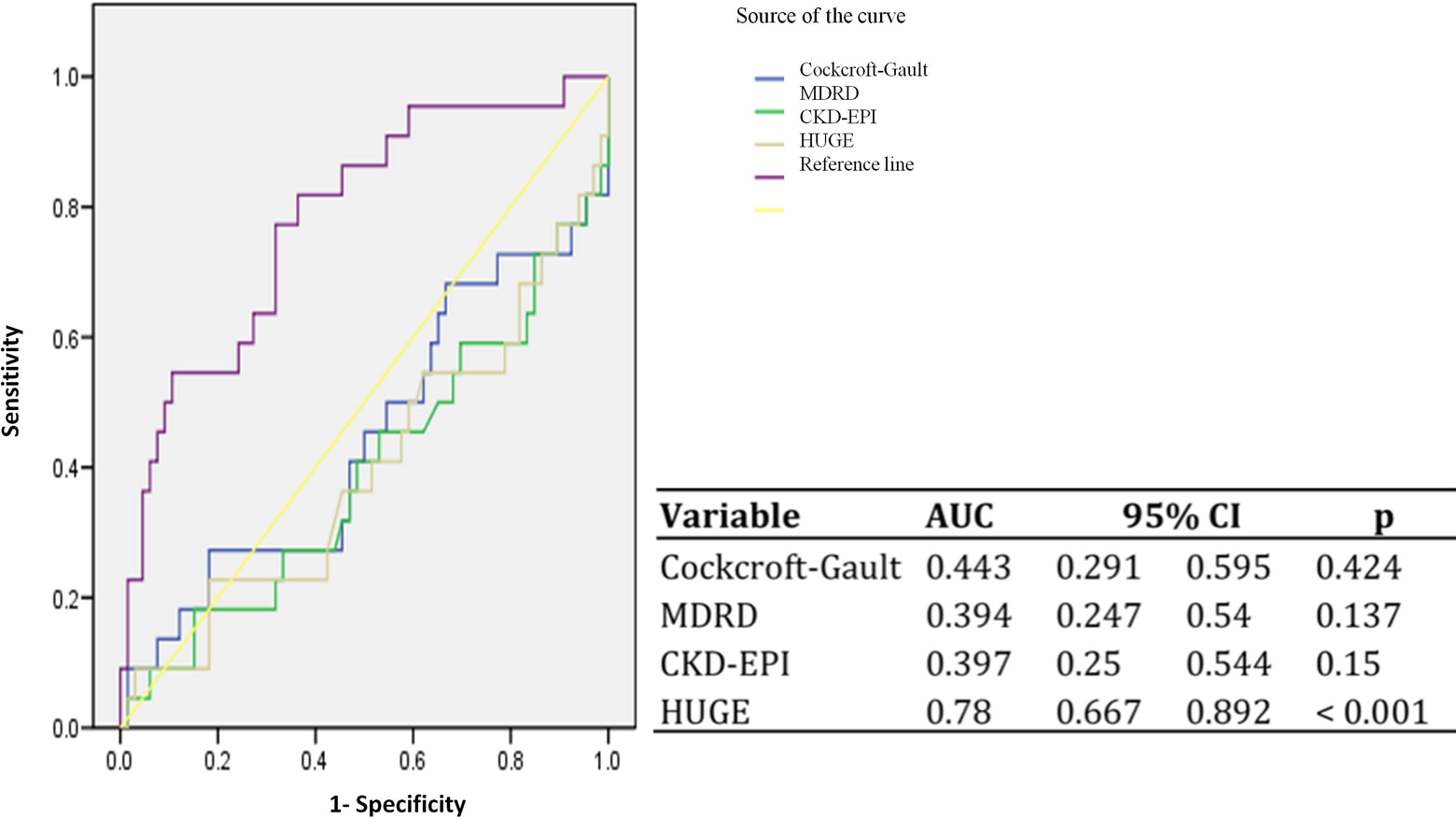
Analysis of the area under the receiver–operating characteristic (ROC) curve (AUC) to predict mortality.
Discussion
There are several indirect markers of renal function that are used to identify patients with a decreased GFR. Measurement of renal function in older adults has clinical implications related not only to drug titration or the prevention of the progression of chronic kidney disease to end-stage renal disease but also to predicting mortality in different scenarios. 17 -19 Maaravi et al. studied 455 patients aged 70 years in a community population cohort, with the intention of determining the effect of reduced GFR on mortality. Reduced GFR was associated with increased risk of death (HR 2.108, 95% CI 1.43-3.12, P < .001). Importantly, most patients with an increased risk of death had normal serum creatinine levels. 20 Similarly, Heras et al in a study that included 80 clinically stable patients 69 to 97 years old showed that diagnosis of chronic renal failure based only on the GFR may lack clinical relevance in this population group. 21
The several different formulas used to calculate the GFR are not validated for people older than 70 years. Using serum creatinine as a fundamental parameter for calculating the GFR has the drawback that its value depends on much more than just filtration by the glomeruli. 22
The HUGE is a recently developed tool to discriminate people with chronic renal failure. It was developed in a sample of individuals from the community, from a formula based on analytical values of serum urea and hematocrit with a correction factor for gender, and has proven to be particularly appropriate in the population aged older than 70 years. This formula offers a fast screening method that is safe and economical and has high sensitivity (93%), specificity (93%), positive predictive value (96%), and negative predictive value (88%). 12 However, external validation of this accuracy is needed.
This formula has been evaluated for use as a prognostic indicator. Robles et al used HUGE to analyze retrospectively a cohort of 84 patients diagnosed with type 2 diabetes mellitus and nephropathy, where the goal was to predict the progression of kidney disease. Using a HUGE cutoff of 1.5, they found that patients with an HUGE value above this cutoff showed an increase in serum creatinine levels at 1 year compared with those who were below the cutoff, and they concluded that in patients with diabetic nephropathy, the HUGE formula may be useful in detecting patients with increased susceptibility to progression to kidney failure. 13 Another study evaluated the relationship between chronic renal failure defined by HUGE value and the patient’s cardiovascular risk. The odds ratio for cardiovascular diseases using the HUGE definition of chronic renal failure was 3.25 (P = .001). 23
Because of the difficulties that currently exist in predicting renal function in the elderly patients and the impact that this has in terms of prognosis, we evaluated the usefulness of this new indirect marker (HUGE) of renal function in patients aged older 70 years with hip fracture, a highly prevalent clinical entity in this age-group that carries a high mortality. 24 -26 These patients often have multiple comorbidities which together with the fracture and subsequent surgery produce a physiological challenge that is potentially life threatening. Importantly, the risk of death in older adults (>65 years) could be assessed with a composite score that includes an indirect marker of renal dysfunction. 27
Previous studies have identified a number of risk factors that influence mortality, including having more than 3 comorbidities, previous myocardial infarction, institutionalized patients with chronic lung disease, pneumonia, duration of surgery, sex, and serum creatinine levels greater than 1.7 mg/dL. 28 However, there are conflicting data on the relationship of renal function (assessed either by creatinine level, urea, BUN, or sodium and potassium) and mortality in this scenario. It seems that depending on the study design and population studied, any of these variables can be significantly associated with postoperative mortality.
In the present study, the long-term mortality seems not to be affected by sex, age, comorbidities, Charlson index, American Association of Anesthesiologists (ASA) scale or type of surgery. However, it may be influenced by the time since fracture, body mass index, biochemical markers (hemoglobin, hematocrit, BUN, and creatinine) and the transfusion requirements in the immediate postoperative period. Analysis of indirect markers of renal function and their association with mortality showed that the HUGE value was independently associated with risk of death in this clinical scenario. This could be explained by the use of several risk factors which per se are prognostic markers. HUGE formula need a calculator, but is not complex and could be performed at the bedside. Additionally it seems to be a useful prognostic tool in other settings. 23
Other studies have tried to analyze whether anemia and blood transfusion are independent predictors of mortality, specifically in patients with hip fracture, without being able to demonstrate an association. 29 Vochteloo et al conducted a cross-sectional study that evaluated the 5-year mortality in 1262 patients aged 65 years and older who were hospitalized for surgery for hip fracture. They were divided into 2 groups according to their hemoglobin levels at admission: anemic patients tended to be older, to have a higher ASA score, and to have received more blood transfusions. In multivariate analysis, anemia was not a risk factor for mortality, but institutionalization and readmission were. 30 In our cohort, anemia, hematocrit, and transfusion requirements also appeared to be associated with increased mortality. However, in contrast to the study of Vochteloo et al, our multivariate analysis showed that neither hemoglobin nor blood transfusion requirements were independent risk factors for death, unlike the HUGE value that proved to be an independent predictor of mortality. It is likely that the inclusion of hematocrit levels in the equation for HUGE improves its prognostic efficiency. Despite the length between fracture and medical attention was not significant in multivariate analysis, we cannot exclude their influence as covariate to modify the components of HUGE values.
The present study has some limitations, as it includes only patients aged 70 years or older admitted with a diagnosis of hip fracture, so it cannot be generalized to the whole population or to geriatric patients in general. Despite a statistical power of 91%, the limitations in the design and a limited sample size could bias the primary outcome. Because this is a retrospective cohort study, comparison of HUGE was made with other surrogate markers of renal function and not with direct markers such as inulin or cysteine clearance. Finally, we were unable to collect data on prefracture functional status and cognitive status and we do not know the causes of death of participants. However, this is the first evidence suggesting that the HUGE formula has value as a marker of mortality in elderly patients with hip fracture.
Conclusion
In conclusion, the HUGE value, but not the GFR determined by Cockcroft-Gault, MDRD or CKD-EPI formulas, is an independent risk factor for mortality in elderly patients with hip fracture.
Footnotes
Acknowledgments
The authors would like to thank Eva Juarez for her support in the manuscript review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Medica Sur Clinic & Foundation sponsored cost for language editing.