
Abstract
Our goal was to determine whether there were age-related differences in pain, opiate use, and opiate side effects after total hip or knee arthroplasty in patients 60 years old or older. We hypothesized that there would be no significant differences between age groups in (1) mean pain score, (2) opiate use after adjusting for pain, or (3) opiate side effects after adjusting for opiate use and pain score. We retrospectively reviewed the electronic and paper charts of all patients undergoing total joint replacements at our institution over 3 years who met the following criteria: (1) 60 years old or older, (2) primary single total knee or total hip replacement, and (3) no preoperative dementia. Preoperative, intraoperative, and postoperative course data were collected using a customized data entry process and database. We divided the patients into 2 age groups, those 60 to 79 years old and those 80 years old or older. Using a marginal model with the panel variable of postoperative day, we investigated the associations between age group and pain, age group and pain adjusting for opiate use, and age group and complications (respiratory depression, naloxone usage as a measure of respiratory arrest, delirium, constipation, and urinary retention) adjusting for opiate use (Xtgee, Stata10, Stata Corp. LP, College Station, Texas). Significance was set at P < .05. We found no significant difference in pain scores between groups, but the older group had significantly fewer opiates prescribed yet significantly more side effects, including delirium (odds ratio 4.2), than did the younger group, even after adjusting for opiate dose and pain score.
Introduction
Pain control after total hip or knee arthroplasty remains a major clinical problem. 1 Although there is a common perception that risks of treating pain with opioid analgesics increase with age, little information exists to substantiate this concept; for instance, the risk of acute respiratory complications after surgery shows little age difference. 2 Given that the incidence of osteoarthritis increases with age and that there will be a 300% increase in the number of persons 85 years old and older in the United States by the year 2050,3 the number of octogenarians and nonagenarians receiving total joint arthroplasties also is expected to increase in the coming decades. 4 –6 It is important to understand how such individuals tolerate pain postoperatively and what the risk is, if any, of side effects associated with their prescribed pain medications.
A few studies have assessed the outcomes associated with total joint arthroplasty in the 80 to 90 years old and older populations. 7 –9 Although such studies have shown that the rate of surgical complications in this population was comparable to that of younger patient populations, the rate of medical complications in the older population was higher. In particular, delirium is common, with estimated incidence rates of 5% to 100% after hip surgery, especially in the patients with fractures. 9 –20
The motivation of the current study was to investigate whether elderly patients need a separate set of pain orders with lower doses to avoid complications associated with opiate use. Our goal was to determine whether there were age-related differences in pain, opiate use, and opiate side effects after total hip or knee arthroplasty in patients 60 years old or older. We hypothesized that there would be no significant differences between age groups in (1) mean pain score, (2) opiate use after adjusting for pain, or (3) opiate-related side effects after adjusting for opiate use and pain score.
Materials and Methods
Institutional review board approval was obtained for this study. We conducted a retrospective review of our institution’s database for patients aged 60 years or more who underwent elective primary hip replacement (Current Procedural Terminology code 27130) or knee replacement (Current Procedural Terminology code 27447) between January 1, 2005 and December 31, 2008. Using these selection criteria, 352 surgeries were identified.
Demographics
Demographic information was extracted from the electronic patient records and written hospital records. Charlson scores were calculated using an online score calculator. 21,22 We divided the patients into 2 age groups: those 60 to 79 years old and those 80 years old or older. The 150 patients in the younger group underwent 161 procedures, and the 172 patients in the older group underwent 191 procedures. We recorded the following information: gender, weight, American Society of Anesthesiologists score, anesthesia type, intraoperative transfusions, estimated blood loss, surgery time, the use of cement, postanesthesia care unit hemoglobin, and length of stay. The only significant differences between groups were age and patient weight (Table 1).
Demographics

Abbreviations: ASA, American Society of Anesthesiologists, PRBC, packed red blood cells, PACU, postanesthesia care unit; CI, confidence interval.
Medication Dosing
Medication dosing was extracted from the electronic medication administration records and the patients’ charts. All opiate dosages were converted to the equivalent dose of intravenous morphine using the standard equal-analgesic tables. 23 All naloxone given was recorded and summarized for each day. All patients were placed on patient-controlled analgesia of hydromorphone or morphine immediately after surgery per a standard total joint order set. All patients were then transitioned to oral opiates and nonopiate analgesics starting on postoperative day 1. The oral opiate administration was on an as needed basis determined by the patient and nurse and the dose was adjusted only if the patient’s pain level required it. In the dosing during that time period, pain scale rating did not trigger a certain prescribed dose; it was based on nursing and patient judgment. We did not have any patients with preoperative dementia who were unable to use the patient-controlled analgesia device.
Hospital Course
The inpatient medical records were reviewed using the standardized data extraction and entry form to review the hospital course and examine the record for all complications. We identified complications that could be related to opiate usage as respiratory depression (defined as any documented oxygen saturation less than 92% that was not related to primary respiratory causes such as pneumonia or pulmonary embolus), respiratory arrest (as indicated by naloxone usage), delirium (defined as any documented change in mental status by a doctor or nurse or a documented diagnosis of delirium), constipation (defined as documented difficulty in bowel movements requiring medical treatment), and urinary retention (any documented urinary retention that required catheter insertion). In addition, intensive care unit transfer information was extracted from the inpatient record.
Pain Scores
Pain scores were reported by patients on a 0 to 10 visual analog scale, with 0 being no pain and 10 being intense pain, and recorded by the nursing staff on all patients during the collection of routine vital signs every 4 hours for the first 24 hours and then every 8 hours. An average pain score was calculated per day.
Data Analysis
We investigated the association between pain and age groups via a marginal model with the panel variable of postoperative day (Xtgee, Stata10, Stata Corp LP, College Station, Texas). Only data from the first 5 postoperative days were analyzed. We then investigated the association between opiate use and age group, adjusting for pain. All summary data are presented as mean values with 95% confidence intervals (CIs). By definition, if the CIs do not overlap, then the mean values are significantly different. Finally, we investigated the potential association between complications (respiratory depression, naloxone usage as a measure of respiratory arrest, delirium, constipation, and urinary retention) and age group, adjusting for opiate use. Complications data are presented as odd ratios; that is, the odds of a given complication in the older group relative to the younger group. Significance was set at P < .05.
Results
No significant difference was found in mean pain score over the first 5 postoperative days between the younger group (4.6 points; 95% Cl, 4.4-4.8) and the older group (4.5 points; 95% CI, 4.2-4.8; Figure 1A). After adjusting for pain, the younger group (60-79 years old) had a significantly higher mean daily morphine intake than did the older group (80 years old and older): 16.4 mg (95% CI, 12.6-20.2) and 8.2 mg (95% CI, 4.6-11.8), respectively. For each unit of increase in the reported pain score, the average morphine intake increased by 1.5 mg (95% CI, 0.8-2.1), controlling for age group (Figure 1B).

Average postoperative pain score (A) (0-10 points, 0 being no pain) and average intravenous morphine equivalent opiate dosing (B) by postoperative day in the younger (60-79 years) old and older (80 years old and older) cohorts. Error bars represent 95% confidence intervals.
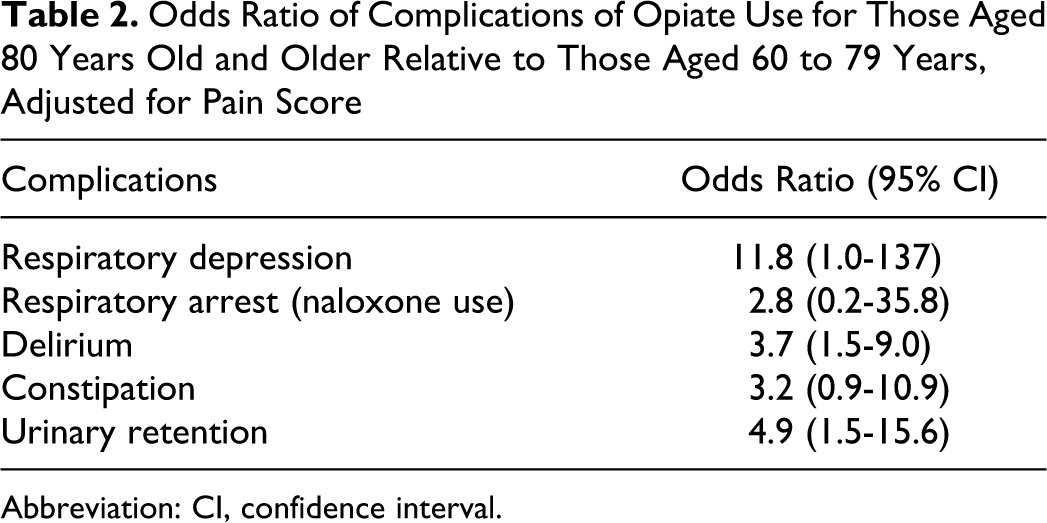
Overall, the older group experienced more opiate-related complications than did the younger group (Table 2). Respiratory depression occurred 11.8 times (95% CI, 1.0-136) more often in the older than the younger group after adjusting for pain and opiate use (P < .05). Although just shy of statistical significance, each milligram of increase in morphine accompanied a 2% (odds ratio 1.02, 95% CI, 0.99-1.04) increased odds of respiratory depression. There was no significant difference between age groups in naloxone use, even after adjusting for pain score and opiate use. The occurrence of delirium was 3.7 times (95% CI, 1.5-9.0) higher in the older than in the younger group, after adjusting for pain and opiate use. Four patients became delirious on postoperative day 0 and were not given patient-controlled anesthesia opiates. Increasing the opiate intake did not significantly change the occurrence of delirium. An increase in pain score was not significantly associated with the incidence of delirium. The occurrence of constipation was 3.2 times (95% CI, 0.9-10.9) higher in the older than in the younger group, after adjusting for pain and opiate use, although the difference was not significant. The occurrence of urinary retention was adjusted for pain and opiate use. For every milligram of increase in opiate use, there was a significant (1.5%) increase in the occurrence of urinary retention.
Odds Ratio of Complications of Opiate Use for Those Aged 80 Years Old and Older Relative to Those Aged 60 to 79 Years, Adjusted for Pain Score
Abbreviation: CI, confidence interval.
Discussion
Our data support our first hypothesis that there is no difference in pain reporting between the younger and older age groups. Other investigators have shown no difference in pain reporting but indicated that older patients used fewer opiates than younger patients. 24 –27 It may be that the elderly population has a lower pain sensation than the younger population. 28 –31 However, little information exists in the literature regarding pain in patients more than 80 years old. Harkins and Chapman 25 and Harkins et al 26 showed a tendency for older individuals to have a higher threshold for heat-generated pain and less ability to sense intense pain in the tooth pulp than did a younger cohort.
Our data refute our second hypothesis that there is no difference between opiate use in the 2 groups. We found that the older group used fewer opiates than did the younger group. It is possible that older patients required less opiates to achieve the same pain relief as younger patients. It is also possible that nursing staff gave less pain medicine to older patients; however, this possibility was not reflected in their pain scores. Gagliese et al 29 have shown a similar result in that older patients (average age, 67.8 years) received less pain medication than younger patients (average age, 47.1 years) despite the same pain scores even with patient-controlled analgesia techniques. Our patients had patient-controlled analgesia dosing during postoperative days 0 and 1.
There have been multiple studies that report age as a risk factor for postoperative opiate-related complications, however, to our knowledge, there is no other study that compares multiple complications of opiates in octogenarian and older patients compared with younger patients. Hix 32 suggests that elderly patients (those aged 65 years and more) are more sensitive to complications early in the postoperative period, although they return to baseline at 3 to 4 days for everything except constipation. Age but not opiate dosing was an independent risk factor for developing postoperative ileus in patients undergoing total joint arthroplasty, 33 for opiate-related respiratory complications in postoperative general surgery patients, 34 and for the development of postoperative urinary retention in general surgery. 35 Age has been shown to be a predictor of the development of delirium in the perioperative period for the elderly patients (those aged 65 years and older). 36 Our data support our third hypothesis that older patients have more opiate-related complications than younger patients. The opiate-related side effects we followed did not increase with opiate dosing except for respiratory depression, which was directly correlated. Naloxone use was not correlated with dose or age. However, urinary retention, constipation, delirium, and respiratory depression were all significantly higher in the older than the younger cohort, even after accounting for the difference in opiate dosing. This finding conflicts with a report that delirium is associated with the underdosing of opiates. 37 It should be noted that the report addressed patients with hip fracture, whereas in our study, the patients underwent elective hip and knee replacements. This finding suggests that octogenarian and older individuals are far more likely to develop these complications with any opiates, regardless of dosing. Our initial concern was that opiate use after elective joint arthroplasty in the elderly patients would result in increased opiate-related side effects and would necessitate a modification of our standard pain orders. The results of the current study suggest that such a modification for patients 80 years old and older is not needed. In fact, the elderly patients’ pain was managed with less opiate dosing, yet they still had a higher incidence of opiate-related side effects. It is possible that the opiate-related side effects are a consequence of the patients’ age and comorbidities and not of the opiates consumed. If the side effects are caused by opiate use, there may be some value in considering other pain management strategies that are not opiate based.
Our study has several limitations. The data were obtained through retrospective review. Although standardized orders were given through a pathway for care, bias could exist in prescribing patterns of practitioners and dosing patterns of nurses. Patients controlled their opiate dosing on the first postoperative day but later oral regimens may have been influenced by nursing habits and bias. Because our data were collected retrospectively, it is possible that we did not record complications that were not documented adequately in the notes. It is known that delirium in particular is underestimated using nursing notes. Future prospective work using a Confusion Assessment Method score 38 would help to lessen this possible error. Previous research has validated a number-based scale, whereas a visual-based scale does not work well with elderly patients. 29 Another limitation of the current study is the mean age for the over-80 group was only 83 years, although ages ranged from 80 to 93 and the mean was still 13 years older than the mean age of the younger group.
In conclusion, in patients undergoing joint replacements, pain scores seemed to be the same for patients aged 60 to 79 years and those who were older. However, the amount of opiates needed to achieve these pain scores was significantly less in the older group. Despite using less opiates, the older group was at higher risk of the complications associated with opiates. Additional study is needed to determine better ways of controlling pain, that is, without the use of opiates, in older patients after joint replacement.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.