
Abstract
The differential diagnosis of respiratory distress in term neonates is broad and includes infectious, cardiac, parenchymal, airway, metabolic, and genetic etiologies. We present the case of a full-term, 10-day-old infant with tachypnea, feeding difficulties, and progressive right-sided lung opacification, initially presumed to be infectious in origin. A systematic diagnostic evaluation ultimately revealed a large patent ductus arteriosus (PDA) associated with airway compression due to the large PDA. Multimodal assessment using chest radiography, echocardiography, computed tomography, bronchoscopy, and electrical impedance tomography was critical in establishing the diagnosis and guiding the initiate and definitive management. The infant underwent successful surgical ligation and division of the PDA, with complete clinical recovery and discharge on room air. This case highlights the importance of a structured diagnostic approach in term neonates with persistent respiratory distress and emphasizes the need to consider vascular-mediated airway compression in the differential diagnosis.
Respiratory distress is a common indication for evaluation in term neonates and is most often attributed to pulmonary or infectious causes. 1 Persistent or worsening respiratory symptoms despite appropriate medical therapy warrant consideration of cardiovascular etiologies, including uncommon mechanisms such as vascular-mediated airway involvement.2,3 Compression of the trachea or main bronchi by adjacent cardiovascular structures can occur and may result in nonspecific respiratory manifestations. Failure to recognize this process in a timely manner can prolong morbidity. Accurate diagnosis depends on a systematic imaging strategy and close multidisciplinary collaboration. Serial chest radiography and echocardiography are central to initial evaluation, while advanced cross-sectional imaging and airway assessment may be required to define anatomic relationships and guide operative planning. Airway compromise from cardiovascular structures most often involves vascular rings, pulmonary artery anomalies, or enlarged pulmonary arteries from significant shunts. 4 While ductal stents have recently been implicated, 5 isolated compression of the left main bronchus by a patent ductus arteriosus (PDA) remains rare.2,3 We present a case of clinically significant airway compression from a large PDA in a term infant, where multimodal imaging directly guided initial management and the decision for surgical ligation.
Case Presentation
A full-term, 10-day-old female infant presented with progressive respiratory distress characterized by worsening work of breathing, poor feeding, and emesis. She was born via cesarean delivery following an uncomplicated pregnancy and discharged home on day of life three. On presentation, physical examination revealed tachypnea with subcostal retractions, abdominal distention, and mildly decreased oxygen saturations without a significant pre- and postductal gradient. Serial chest radiographs demonstrated progressive right-sided pulmonary opacification with associated hyperinflation (Figure 1). An infectious evaluation was unrevealing; however, empiric antibiotics were initiated due to clinical deterioration. The infant was admitted to the neonatal intensive care unit and supported with continuous positive airway pressure (CPAP). Despite noninvasive respiratory support, she developed worsening respiratory acidosis, prompting intubation.
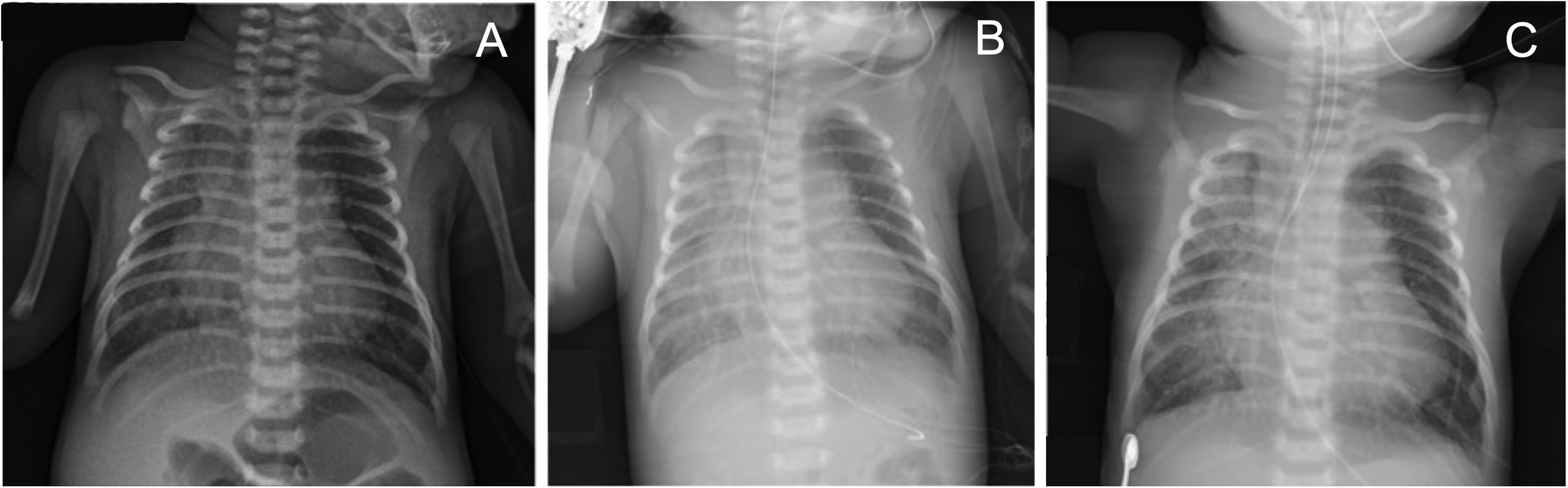
Radiographic series of chest X-rays (CXR) demonstrating the persistent opacification of the right side of the chest. (A) Admission imaging with no respiratory support. (B) Follow-up radiograph imaging while on continuous positive airway pressure. (C) Confirmatory X-ray after intubation due to worsening respiratory status.
The infant began to exhibit signs of worsening cardiovascular compromise, including poor peripheral perfusion, hyperdynamic pulses, and hepatomegaly. Chest radiography revealed cardiomegaly and pulmonary vascular congestion, raising concern for congestive heart failure. Initiation of diuretic therapy resulted in clinical improvement, allowing extubation to CPAP. Transthoracic echocardiography demonstrated a large PDA, measuring approximately 6 × 3 mm, with bidirectional shunting. Computed tomography (CT) of the chest identified a window-type PDA, a bovine aortic arch with rightward deviation of the descending aorta, and extrinsic compression of the left mainstem bronchus between the right pulmonary artery and the aorta. The left bronchial lumen measured approximately half the diameter of the right bronchus (Figures 2 to 3).
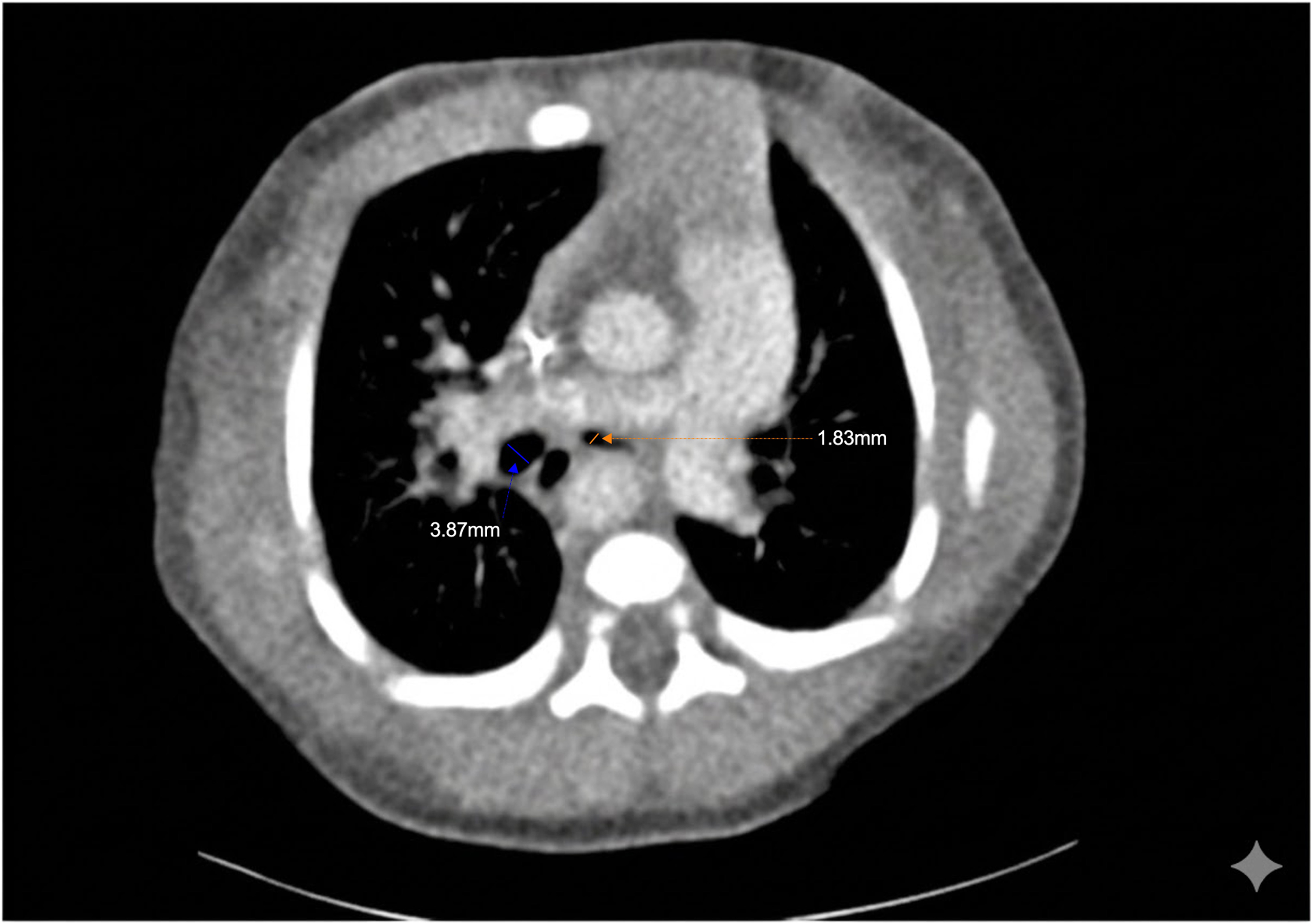
Computed tomography of the chest demonstrating narrowing of the left mainstem bronchus (1.8 mm) by the right pulmonary artery, in comparison with the right mainstem bronchus (3.8 mm).

Computed tomography three-dimensional (3D) reconstruction demonstrating the close anatomic relationships of the trachea, bronchial tree, and great arteries. The left posteromedial view (right) shows a window-type PDA between the aorta and the pulmonary artery. Abbreviation: PDA, patent ductus arteriosus.
The infant remained persistently tachypneic on CPAP without hypoxemia, prompting further physiologic assessment. Bedside electrical impedance tomography (EIT), a noninvasive imaging technique that provides real-time, radiation-free visualization of regional lung ventilation by measuring changes in electrical impedance across the chest, 6 demonstrated asymmetric ventilation favoring the right lung that worsened during sleep and at lower airway pressures (Figure 4). EIT uses electrodes placed equidistantly around the chest to measure impedance as small alternating currents pass through the thorax. Because air conducts electricity less effectively than tissue, impedance differences allow identification of air-filled lung regions and enable real-time assessment of ventilation distribution between the right and left lungs. 7 In our patient, EIT demonstrated reduced ventilation to the left lung in the supine position, with improvement during left lateral positioning (Figure 4), supporting dynamic extrinsic airway compression. Continuous positive airway pressure settings were subsequently adjusted to optimize left lung recruitment and minimize atelectasis while awaiting definitive management. Dynamic bronchoscopy confirmed near-complete collapse of the left mainstem bronchus due to extrinsic pulsatile compression, with minimal improvement despite high positive airway pressures. A ventilation–perfusion scintigraphy demonstrated delayed washout and reduced perfusion of the left lung, confirming the EIT findings.

Electrical impedance tomography results depicting differences in ventilatory patterns in different positions and continuous positive airway pressure (CPAP) levels. The infant had decreased ventilation to the left lung during supine positioning, and despite CPAP increase, there were minimal changes in ventilation. Improvement of left lung ventilation is evidenced at lower CPAP pressures and left lateral decubitus positioning.
Medical closure of the PDA with ibuprofen was attempted without success. The PDA anatomy was deemed unsuitable for transcatheter closure due to a short ampulla and wide ductal morphology, which precluded secure device anchoring. Given the combination of persistent airway obstruction and a large PDA, the infant underwent left thoracotomy with ligation and division of the ductus arteriosus. A left thoracotomy was performed, and the latissimus dorsi was spared. The 3rd interspace was identified and entered. The left subclavian and aortic arch were clearly identified. The proximal descending aorta was mobilized. The course of the left recurrent laryngeal nerve was identified around the PDA. The PDA was then circumferentially mobilized. This vessel was extraordinarily short, and so the pericardium was entered, and the pulmonary artery size was mobilized. Two sutures were used to ligate the PDA. The PDA was then divided, and an additional 2 sutures were placed on the aortic end of the duct.
Postoperatively, her respiratory status improved rapidly, allowing extubation and weaning to room air. She tolerated full oral feeds, demonstrated appropriate weight gain, and was discharged on a diuretic, which was subsequently discontinued during outpatient follow-up. Genetic evaluation, including chromosomal microarray, did not reveal an underlying diagnosis. At follow-up, the patient remained asymptomatic with normal growth and no evidence of increased work of breathing.
Discussion
This case illustrates a rare etiology of neonatal respiratory distress in a term infant: extrinsic airway compression caused by a large, window-type PDA. Although PDAs are among the most common congenital heart defects, 8 the majority are small and close spontaneously in full-term infants without any respiratory compromise. 9 However, external compression of trachea or main bronchi by a persistently large PDA can cause significant respiratory symptoms (eg, wheezing, stridor, or cyanosis) with air trapping, hyperinflation, and atelectasis seen on chest imaging. 3 This case highlights the need for a high index of suspicion and a systematic, multimodality imaging strategy when evaluating uncommon causes of neonatal respiratory distress related to airway compromise. In addition, the use of EIT at the bedside helped guide the respiratory management while awaiting additional diagnostics and therapeutic interventions. Definitive management with surgical ligation and division of the PDA is a reasonable and effective treatment option in appropriately selected cases.2,3,10
In rare instances, large PDAs may distort mediastinal anatomy and cause extrinsic airway compression, particularly when associated with atypical ductal morphology or abnormal great-vessel anatomy. 8 Window-type (Krichenko type B) PDAs are characterized by a short, wide duct lacking the constricted ampulla required for device anchoring. 11 These lesions are frequently resistant to medical therapy and often require surgical correction. In this patient, the combination of a window-type PDA, bovine aortic arch, and rightward deviation of the descending aorta resulted in pulsatile compression of the left mainstem bronchus, producing dynamic airway collapse. Relief of the respiratory symptoms were achieved after “shrinkage” of the PDA with a surgical ligation and division, and removal of the left-to-right shunt and volume overload, highlighting the contribution of the large ductal diameter and shunt flow on the compression mechanism.3,12
Vascular causes of airway compression may mimic pneumonia or atelectasis on chest radiography, contributing to diagnostic delay.3,4 In our case, the discordance between persistent respiratory symptoms and radiographic findings prompted a comprehensive, multimodal evaluation. Echocardiography, cross-sectional imaging, bronchoscopy, ventilation–perfusion scintigraphy, and bedside EIT together delineated both the anatomic abnormality and its functional respiratory consequences. Notably, EIT provided noninvasive, real-time assessment of ventilation asymmetry and positional effects, complementing static imaging and informing respiratory management.6,7 To our knowledge, this is the first case report to utilize EIT to guide bed-side management and optimize the clinical state prior to definitive closure of the PDA.
Conclusion
This case emphasizes the importance of maintaining a high index of suspicion for cardiovascular causes of airway compromise in neonates with persistent or unexplained respiratory distress. The close anatomic relationship between the ductus arteriosus and the left mainstem bronchus makes this a recognized, although uncommon, complication in infants with a large PDA. Electric impedance tomography can guide initial management and titration of respiratory support. Surgical ligation and division remain the definitive treatment for these cases in patients with severe symptoms. Early recognition through targeted, multimodal imaging can guide immediate management, facilitate timely intervention and lead to excellent clinical outcomes, underscoring the reversibility of this condition when promptly addressed.
Footnotes
Abbreviations
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Pediatric Scientist Development Program (grant number 5T32HD098061) and the Brown Family NICU Research Award.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.