
Abstract
Introduction
The burden of cardiovascular disease, including congenital and rheumatic heart disease, is disproportionately higher in low- and middle-income countries (LMICs) compared with areas with advanced healthcare systems. 1 Rheumatic heart disease, a commonly acquired cardiovascular disease in low-resource settings, is responsible for more than one million deaths per year. 2 Similarly, 90% of the one million children born with congenital heart defects each year are in areas with suboptimal healthcare or no access to care. 3 Despite this increased need, access to cardiac surgery remains very limited in LMICs.
The humanitarian efforts of nongovernmental organizations (NGOs) attempt to lessen the burden of cardiovascular disease in LMICs.1,3 Surgical volunteerism programs aim to provide care in the form of short-term cardiac surgery missions. Long-term follow-up of patients after the mission is particularly important for cardiac surgery and the provision of standard access to care. Patients are often discharged with medications essential for the long-term success of their procedure, surgery, or treatment plan; their medications and clinical status may change depending on disease complexity and postoperative complications, prompting the need for routine monitoring.4,5
Clinical databases have been constructed to measure the success of medical trips, with metrics to analyze both outcomes and assess quality of life and freedom from disease. 3 Short- and long-term outcomes data are a known challenge for medical missions in LMICs, with 30-day follow-up rates rarely reported and commonly less than 30% when available.1,6,7 Sykes noted in a 2014 systematic review of short-term medical missions that outcome information beyond one week was reported in only 26% of medical service trip publications, and follow-up percentages ranged between 14% and 84% in those cases. 6
Commonly noted barriers to follow-up care include weak or overwhelmed local infrastructure and logistical issues at the mission sites, including language constraints.7,8 Sykes reported that some medical service organizations may not prioritize standardized evaluation tools, data collection, and analysis because research is thought to provide only limited mission benefits. 6 Other NGO's presume lack of technology, financial costs, misunderstandings about the need for further care, or remote location of a patient's home as barriers for patients’ follow-up care and data collection.8,9 There is currently little evidence to support these various assumptions for lack of follow-up data. Although the primary altruistic mission goal may be to clinically review and operate on as many patients as possible, delivering care without accountable follow-up and understanding of the outcomes through research falls short of the ideal standards of care and presents an ethical dilemma. 6 We therefore chose to examine the demographic, socioeconomic, and surgical factors associated with long-term follow-up rates following short-term cardiac surgery missions in nine LMICs, endeavoring to improve this essential component of patients’ comprehensive heart care.
Patients and Methods
CardioStart International, a nonprofit organization providing cardiac surgery services in LMICs, provided the underlying data for this study using RedCap.10,11 Institutional review board approval was obtained by the University of Minnesota, USA. Each of the nine mission sites agreed to data collection prior to the surgical mission, and separate consent forms for treatment and data collection were obtained from each patient or patient's guardian by the surgeon and database researcher, respectively. A research coordinator was provided by CardioStart International for each mission to record patient information, including demographics, socioeconomic, and surgical data. Follow-up care was scheduled with an appointed local physician at 1 week and 30 days, and in-person follow-up data collection in the form of structured interviews and questionnaires was attempted by the CardioStart International research coordinator on subsequent missions to the same site. Successful follow-up for the study involved completion of in-person interviews and repeat questionnaires by CardioStart International researchers. The time periods for return visits and data collection did, however, vary due to local team availability, fluctuating patient volumes, financial constraints, and patient logistical issues.
A retrospective analysis of the prospectively maintained database was conducted to identify mission sites with at least two visits to the same country and at least 20 patients treated in total (Figure 1). The following nine countries that experienced multiple missions in the same location, allowing the opportunity for subsequent follow-up data collection, were included in analysis: Brazil, Dominican Republic, Ecuador, Ghana, Honduras, Nepal, Peru, Tanzania, and Vietnam. Four patients, for whom there was a lack of minimal data, including age and surgical information were subsequently excluded from the study. A total of 550 pediatric and adult patients who underwent cardiac surgery between 2009 and 2020 were then identified for analysis.
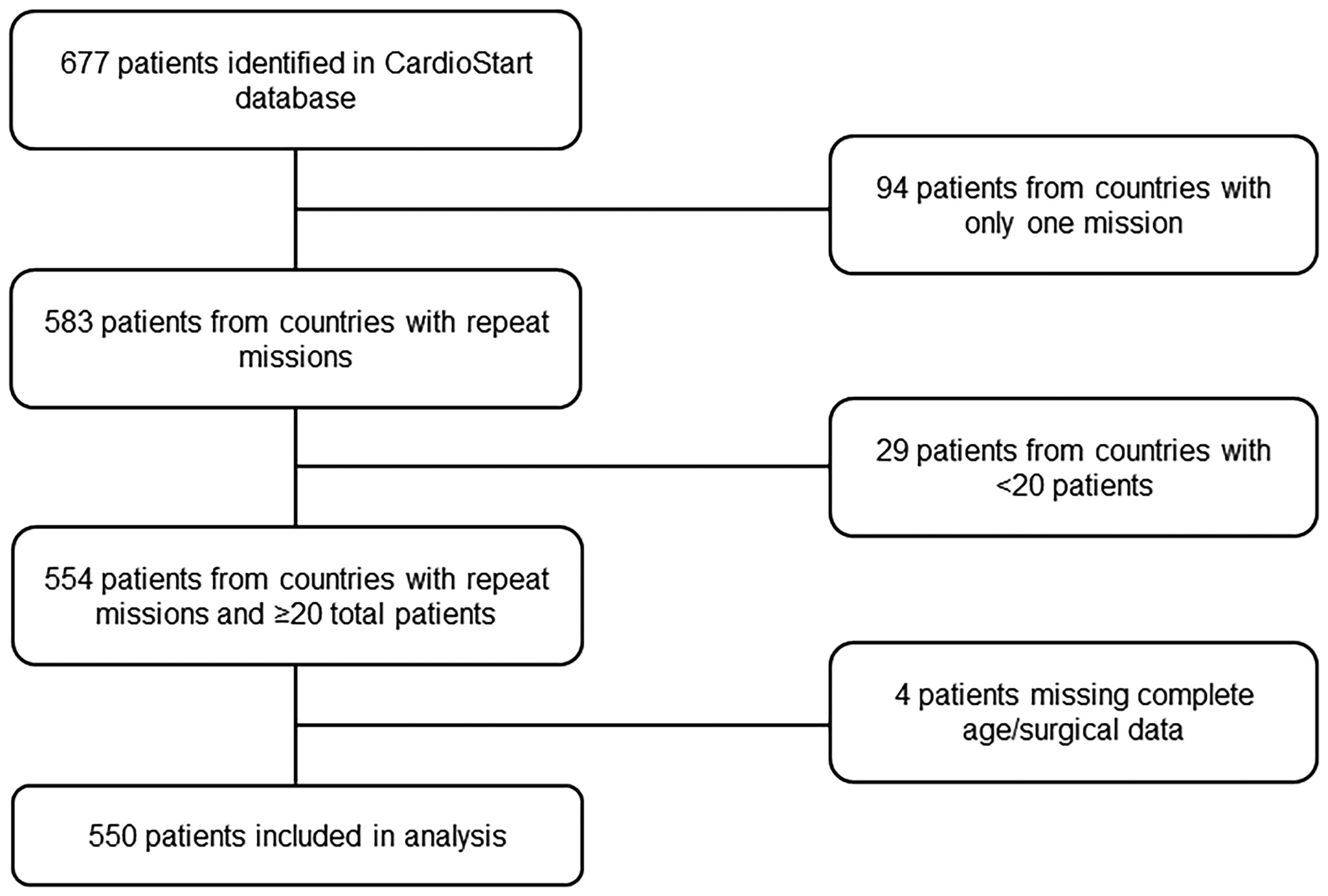
A flowchart of the patient cohort.
Demographic, procedural, and socioeconomic factors were analyzed and compared with the availability of follow-up information. Age, sex, and country of residence were examined as demographic factors. Surgical factors included the type of surgical intervention performed. The 11 socioeconomic status (SES) surrogate metrics included home access to a computer, electricity, hot water, an inside toilet, internet, phone (cell phone or landline), nondirt flooring, refrigerator, running water, shower, and television. The SES metrics were collected from each patient using the dataset questionnaires and represent individual reflections of poverty level.
All patient demographic characteristics are described as median and interquartile ranges (IQRs) or counts and percentages, as appropriate. Categorical variables were compared using either the χ2 test of independence or the Fisher exact test. P values <0.05 were considered statistically significant. The standardized residuals (r) of the χ2 test were calculated to compare the nature of dependence, with an absolute value >2 considered significant. All data were analyzed with the use of R version 4.2.1 (R Foundation for Statistical Computing).
Results
The study population included 550 adult and pediatric cardiac surgery patients from countries with at least 20 total patients and multiple missions per site (Figure 1). The median age at the time of surgery was 18 years (IQR 4-43). Patient demographic factors are summarized in Table 1. The total population follow-up percentage was 14.7% (n = 81), with a mean time to follow-up of 1.46 years and range between 20 weeks and 4 years. There were 275 (50%) adult patients over 18 years, 135 (24.5%) patients between 5 and 18 years, and 140 (25.5%) patients less than five years old. Of the 547 patients with gender information, 268 (49.0%) were males. No significant relationship was observed between follow-ups and sex or age categories (P = 0.29 and 0.30, respectively). In Brazil, Dominican Republic, Ecuador, Ghana, Honduras, Nepal, Peru, Tanzania, and Vietnam, a number of patients with successful follow-up were 0, 24 (30.4%), 1 (4.0%), 4 (7.5%), 3 (10.0%), 0, 14 (10.3%), 0, and 35 (43.2%), respectively. The mission location, categorized by country, was significantly associated with the follow-up rates (P < 0.0001). Patients from the Dominican Republic and Vietnam had significantly positive standardized residuals, r = 3.6 and r = 6.7, respectively, while Brazil and Tanzania showed negative correlations, r = −3 for both.
Follow-Up Percentages by Patient Demographic Factors. a
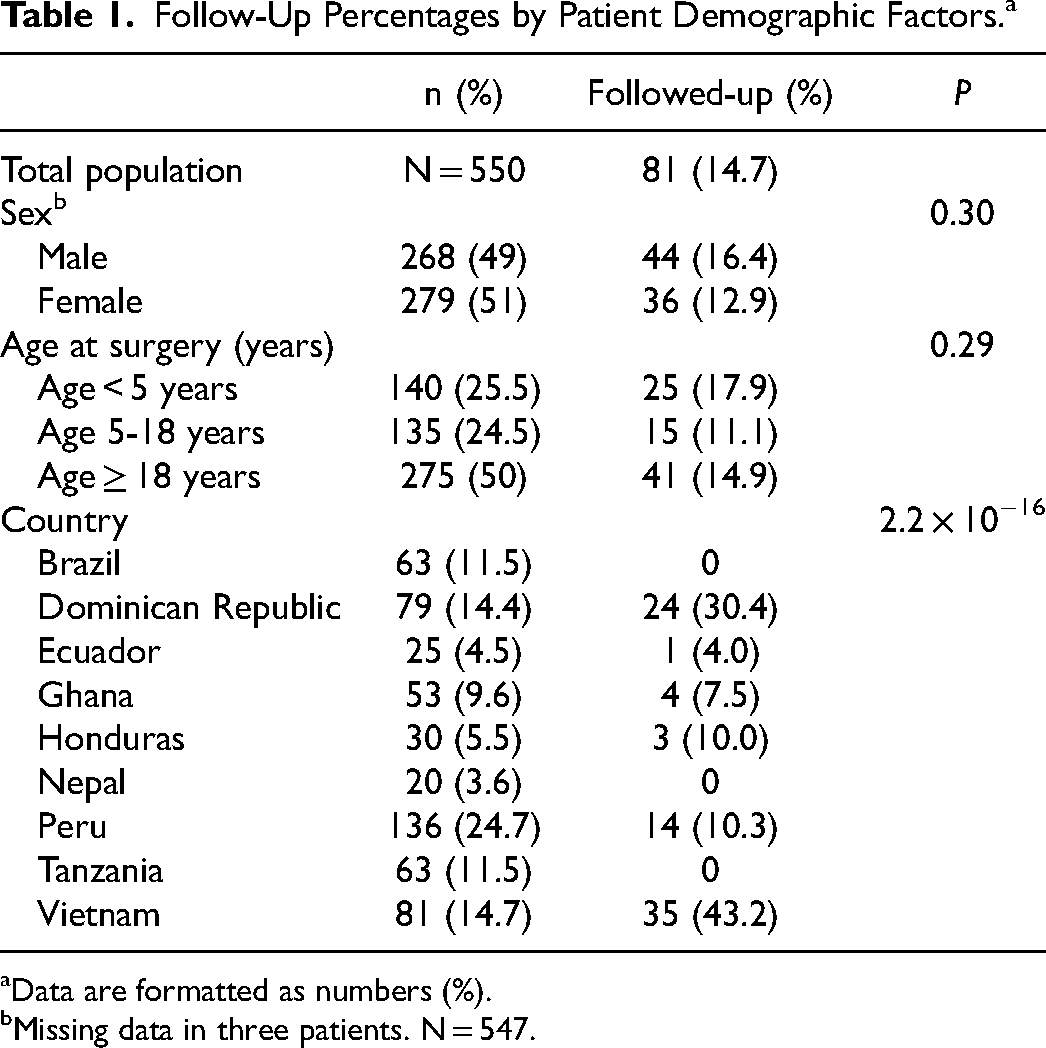
Data are formatted as numbers (%).
Missing data in three patients. N = 547.
Surgical information, including the type of intervention, was complete for 335 patients. The documented surgical interventions are depicted in Figure 2. The type of intervention was significantly associated with follow-up data (P = 0.009). For this analysis, the miscellaneous “other procedures or combinations” category was excluded due to its diverse, unspecified contents. The adult cardiac cases, including coronary artery bypass grafts (CABGs) and valvular interventions, revealed no trends correlating the type of procedure and follow-up likelihood. Congenital procedures demonstrated a trend of increased follow-ups among higher Risk Adjustment for Congenital Heart Surgery (RACHS-1) categories. The patients who underwent a ventricular septal defect (VSD) procedure, a RACHS-1 score of 2, had a significantly increased follow-up rate of 32.5%. Patients who underwent isolated atrial septal defect (ASD) closures or patent ductus arteriosus (PDA) ligations beyond 30 days old, both being lower risk RACHS-1 score of 1, had decreased follow-up percentages (7.3% and 3.6%, respectively). Further analysis of the VSD population demonstrated that 12 of the 13 follow-up cases (92.3%) were from Vietnam, the country with the highest follow-up rate in the study, indicating that mission location may have influenced the VSD follow-up percentage.
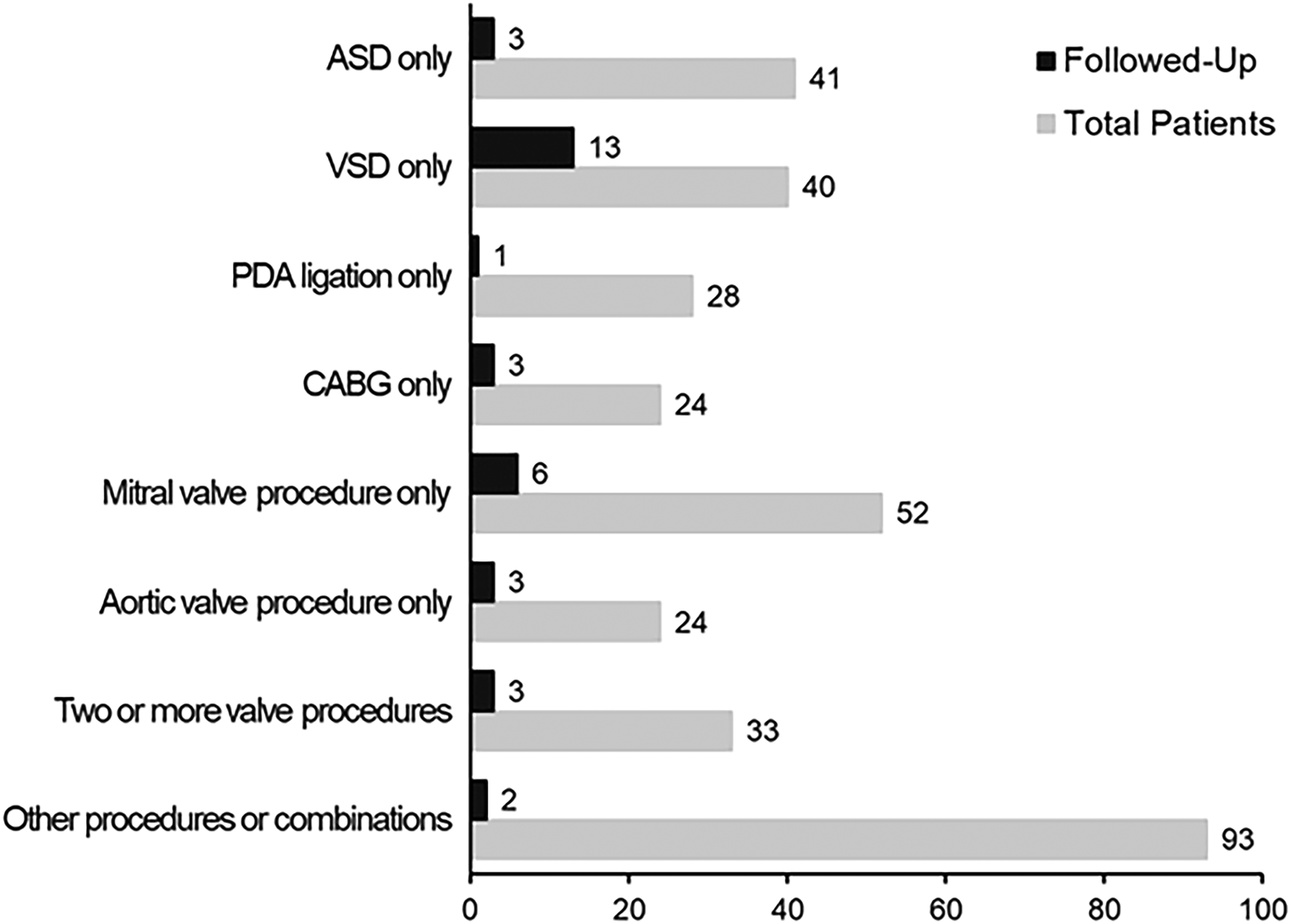
Follow-ups by cardiac surgical intervention. A subset of 335 patients exhibited a follow-up percentage of 10.1% with significant association to surgical intervention (P = 0.009). The other category was excluded from analysis. ASD, atrial septal defect; CABG, coronary artery bypass graft; PDA, patent ductus arteriosus; VSD, ventricular septal defect.
The 11 SES surrogate factors were examined to determine if poverty levels were relevant to patients’ ability to attend follow-up appointments; these factors are detailed in Table 2. The total number of patients with access to electricity, hot water, a refrigerator, running water, and a shower in the home were 412 (74.9%), 54 (9.8%), 257 (46.7%), 340 (61.8%), and 225 (40.9%), respectively. A subset of 441 patients with complete inside/outside toilet data revealed that 269 (61.0%) patients had access to a toilet inside the home. Another subset of 344 patients with complete information on the type of flooring inside the dwelling demonstrated that 282 (82.0%) had wood or concrete flooring compared with dirt flooring. This indicates that electricity, an inside toilet, nondirt flooring, and running water were more common than not in homes in LMICs. Of these cohorts, the follow-up percentages ranged from 11.0% to 14.3%, but there were no significant associations between home features and follow-ups (P > 0.05).
Follow-Up Percentages by Socioeconomic Factors. a
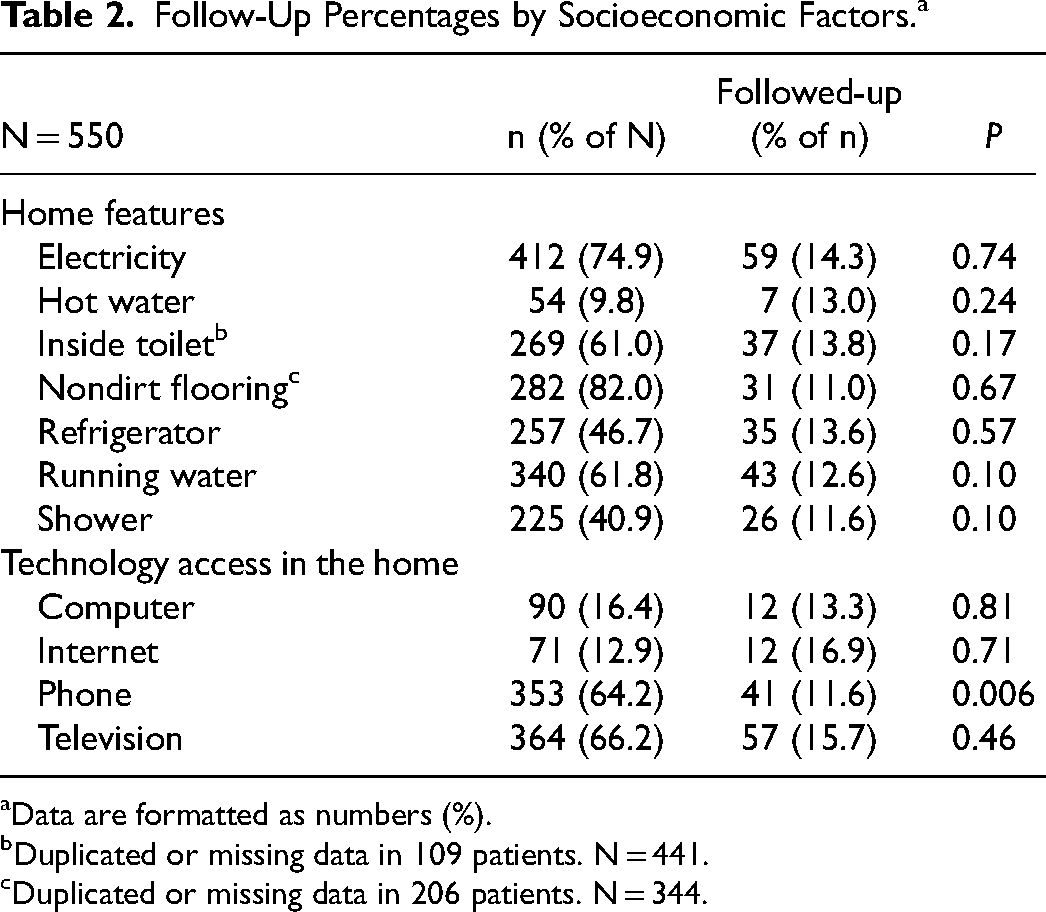
Data are formatted as numbers (%).
Duplicated or missing data in 109 patients. N = 441.
Duplicated or missing data in 206 patients. N = 344.
Access to a phone (n = 353, 64.2%) and television (n = 364, 66.2%) in the home showed greater prevalence than access to a computer (n = 90, 16.4%) or the internet (n = 71, 12.9%) (Table 2). The follow-up rates for patients with access to a computer, internet, or television were 13.3%, 16.9%, and 15.7%, respectively. These technological factors were not significantly associated with completion of follow-up (P > 0.05). Conversely, patients who had access to a landline or cellphone in the home had a significantly decreased follow-up rate of 11.6% (P = 0.006).
Discussion
Despite the millions of cases of congenital and acquired heart disease reported, access to cardiac care remains severely limited in LMICs.1–3 Finding and evaluating patients is an upfront challenge, and in some locations, primary screening is rudimentary. Patient's perception of their disease and access to primary and tertiary care facilities remain uncertain and complex. Short-term cardiac surgery missions led by CardioStart International teams strive to lessen the cardiovascular disease burden in LMIC communities through the following three goals: increase access to lifesaving interventional and surgical procedures; assist general education of the local team on new cardiological management and perioperative techniques; and provide essential equipment to help the programs reach eventual self-sustainability.
A database is crucial to measuring the success of these goals, with a focus on outcomes and quality of care data. Consistent with current literature reporting 30-day follow-up rates of less than 30%,1,6,7 our study found an overall rate of 14.7% across nine countries hosting repeat, short-term cardiac surgery missions. The time to follow-up extended between 20 weeks and 4 years, which may explain the lower rates, as longer-term follow-ups sought in our study can present greater challenges to patient contact and return. The patients’ socioeconomic factors were predominantly insignificant in explaining the lack of follow-up information, with the exception of phone access. Alternatively, demographic and surgical factors, including the country where the mission occurred and type of intervention, showed significant correlations.
The location of the mission was the most significant factor associated with follow-ups. The differences between countries could reflect nonuniform data collection procedures or unique, site-specific barriers to obtaining follow-ups, such as distance to facilities, difficulty of travel, and local program support. For example, missions to Brazil resulted in a 0% follow-up rate, but some patients in Northern Brazil reported traveling up to 1,000 km to attend the preoperative screenings, arriving sometimes without a relative due to family work obligations. Other studies have also reported long distance travel is a substantial burden and increasing levels of remoteness led to greater loss to follow-up1,8 and poorer overall outcomes. 12 The Dominican Republic had the second highest follow-up rate, which may be influenced by a strong local partnership. To illustrate: a local healthcare professional, permanently employed at the Dominican Republic mission site, actively worked to bring patients back to the clinic. Upon acceptance to a CardioStart International mission, the local partner collected extensive contact information, including addresses and phone numbers, for the patient, as well as their neighbors and close relatives. The importance of updating their contact information and following up after cardiac surgery was extensively explained to patients. The local partner then began reaching out to patients to organize their return to the hospital as soon as future mission dates were set, allowing coordinated follow-ups with physicians and database collectors during subsequent missions. Thus, implementing site-specific guidelines and nurturing local healthcare team involvement at each mission site may improve the effectiveness in obtaining comprehensive, long-term follow-up information. We anticipate a potential barrier to widespread implementation of local follow-up partners may be inconsistent with job security at some mission locations.
The requirements for follow-up after cardiac surgery vary depending on the type of intervention. Procedures, including valvular interventions and CABGs, rely heavily on routine follow-ups for medication adjustments, cardiac function monitoring, and potential repeat surgeries. Previous literature has stressed the importance of long-term follow-up after cardiothoracic surgery in high-income countries, particularly after CABG procedures. Noyez et al demonstrated that a structured one-year follow-up could obtain high response rates and provide crucial information on mortality to assess a program's quality control. 13 Another study by de Ward et al noted a lack of primary care follow-up at 30 days after a CABG procedure was associated with a 5-fold increased risk of poor cardiac function at one year, which may be attributed to suboptimal monitoring of complications, rehabilitation progress, or optimization of medications. 14 We did not find an increased trend in follow-up data among CABG and valve procedures, which must be considered a critical area for improvement. There was, however, a trend toward higher follow-up rates in congenital cardiac procedures with a higher RACHS-1 score. Patients undergoing congenital ASD closures and PDA ligations demonstrated lower follow-up percentages when compared with higher risk VSD procedures. Differences among procedure types may reflect unclear expectations for follow-up care and monitoring after corrective cardiac surgery. We strongly support the recommendation that children with complex congenital heart disease are ensured lifelong follow-up to address both the operative revision as a child grows older and the long-term, specialized care needed during adult life. Additionally, organizations should expect and strive for each patient to attend at least one follow-up appointment with the visiting NGO after undergoing a major cardiac intervention.
Beyond organizational and procedural factors, our study investigated the individual patient factors influencing follow-ups. Previous literature has reported lack of technology and financial costs as major restrictions to patients’ ability to be contacted and followed,8,9 yet to the best of our knowledge, no report has statistically analyzed the correlation between specific SES factors and lack of follow-up. Our study found the majority of SES surrogate factors did not significantly correlate with follow-up attendance, with the exception of phone access. Access to a telephone showed an unexpectedly negative association with follow-ups for undetermined reasons. This challenges the current understanding that lack of technology and phone subscriptions are barriers to follow-up. 8 However, the analysis does not account for the stability of phone subscriptions or the role of technology in follow-up methods. Temporary or transient phone access may hinder patients’ ability to be contacted for future follow-up. For example, some patient interviews revealed that phones may be provided by the current employer and were then confiscated if their position were terminated, which may obscure the correlations between phone access and follow-up. Further study into the stability of technology access could provide useful insight for active, technology-based follow-up protocols.
Through discussions with patients and local team members, we found other regularly apparent barriers to follow-ups that were not quantified in the questionnaires and analysis. In addition to the long distances traveled and employment-dependent phone access, literacy, finances, and local perceptions may also influence the likelihood of a patient to follow-up. Literacy rates varied between mission sites, and written guidelines in the local language may not be sufficiently clear or reassuring, unless they are written at an appropriate reading level and shared with the attending family member. There may be additional unexpressed reluctance to return for evaluation in case a negative clinical finding is exposed. Misconceptions and past family experiences lead some patients to avoid hospitals, as they believe hospitals are where one goes to die. In certain locations, patients and relatives are also required to pay for a portion of the care they receive in the hospital (disposables, medications, etc), even though international mission groups, including CardioStart International, provide all equipment and specialist care freely. In these circumstances, patients and their families may specifically avoid being contacted by the hospital for fear that they will be required to pay a bill. Unquantified factors, including literacy, hospital perceptions, and financial expectations, should be examined and addressed in future studies to holistically improve organizational follow-up rates at each mission site.
Finally, the short-term nature of global surgical missions, ranging from one to two weeks in duration, presents inherent challenges to long-term patient follow-up. There exists a narrow time frame for patients to return for follow-up and a limit for how many follow-up patients can be seen on subsequent missions, in addition to the new surgical patients. Time limitations may be overcome by focusing on multiple return missions to the same site within a year, rather than spreading the missions over numerous countries. Consistent visits throughout the year to the same site may promote stronger local connections, who can contact patients for follow-up appointments. In future missions, follow-up data collection may also be transitioned under the responsibilities of local healthcare teams, which promotes increasing local involvement in patient care and outcomes research. Local teams may benefit from this partnership and accurate collection of cardiological and surgical activities, as it may lead to better source funding for their program, educational growth, transfer of skills, and eventual progression toward self-sustainability.
Conclusions
Short-term international cardiac surgery missions strive to bring cardiac care to the millions of patients in need in LMICs. Patient follow-up after these missions is crucial, not only to the provision to care but also to analyzing outcomes and ensuring quality. Our study identified mission location, type of intervention, and phone access as factors associated with follow-up compliance. To combat inconsistent follow-ups, improvements to the follow-up guidelines should reflect a multilevel approach, targeting both patient and organizational factors. CardioStart International is now partnered with the World Database for Pediatric and Congenital Heart Surgery and is placing greater emphasis on the formal incorporation of local healthcare partners in follow-up appointments and data collection. Education is also provided to patients before discharge and local teams during mission planning to better emphasize the importance of staying in contact and the expectation of follow-up at determined intervals. By confronting the challenge of low follow-up attendance and uncovering the information currently concealed by lack of follow-up data, humanitarian organizations and local teams may better achieve their goals of quality cardiac care, program sustainability, and community growth.
Limitations
Our retrospective analysis of a prospectively maintained database has inevitable flaws. Patient selection bias, cultural differences between mission sites, and missing information could not be avoided. We were unable to account for mortality, which may be the underlying reason for a subset of the lack of follow-up information. Small sample sizes also may not adequately represent the countries’ patient populations. To draw stronger conclusions, complete data should continue to be collected from the ongoing missions and integrated into the analysis to increase power.
Footnotes
Abbreviations
Acknowledgments
The authors would like to thank the volunteers who have dedicated their time, donations, and efforts in support of CardioStart International.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.