
Abstract
Background
Congenital heart disease (CHD) is the most common major congenital anomaly. Ninety percent of children with CHD are born in low- and middle-income countries (LMICs), where over 90% of patients lack access to necessary treatments. Reports on barriers to accessing CHD care are limited. Accordingly, it is difficult to design evidence-based interventions to increase access to congenital cardiac surgical care in LMICs.
Objective
We performed a qualitative systematic review to understand barriers to accessing congenital cardiac surgical care in LMICs.
Methods
We conducted a search of Ovid MEDLINE and CINAHL databases to identify relevant articles from January 2000 to May 2021. We then used a thematic analysis to summarize qualitative data into a framework of preoperative, perioperative, and postoperative barriers.
Results
Our search yielded 1,585 articles, of which 67 satisfied the inclusion criteria. Notable preoperative barriers included delayed diagnosis, insufficient caregiver education, financial constraints, difficulty reaching treatment centers, sociocultural stigma of CHD, sex-based discrimination of patients with CHD, and Indigeneity. Perioperative barriers included lack of hospital resources and workforce, need for prolonged hospitalization, and strained physician–patient relationships. Many patients faced barriers postoperatively and into adulthood due to a shortage of critical care resources, inadequate caregiver counseling and patient education, lack of follow-up, and debt from hospital bills and missed work.
Conclusion
Reducing neonatal and childhood mortality begins with recognizing barriers to accessing health care. Our systematic review identifies and classifies challenges in accessing CHD in LMICs and suggests solutions to major barriers.
Introduction
Congenital heart disease (CHD) poses a significant disease burden worldwide. CHD is the most common major congenital anomaly, present in approximately 1 in 100 live births, and accounting for one-third of all birth defects. 1 Each year, an estimated one million children are born with CHD. 1 Approximately 49% of patients with CHD will require surgery at some point in their lives. Further, when left untreated, most children with CHD will not live past their fifth birthday. 2
Due to advancements in pediatric cardiac diagnostic investigations and surgical care in the last 20 years, 90% to 95% of CHD patients who receive timely surgical intervention survive with good quality of life well into their adult years. 1 As a result, in many high-income countries (HICs), there are now more patients with adult CHD (ACHD) than children with CHD. Unfortunately, while these statistics hold true in HICs, the reality is very different in low- and middle-income countries (LMICs), where pediatric cardiac care is lacking and access to adequate surgical intervention remains a challenge. 2 This is especially concerning given that 90% of CHD births occur in lower-resource settings. 2 Indeed, the alarming worldwide disparity in congenital cardiac care results in nearly 200,000 preventable deaths each year. 2
In 2016, the United Nations introduced the Sustainable Development Goals (SDGs) to tackle major global development challenges, two of which were addressing high neonatal and under-five mortality. 2 Given that CHD contributes substantially to childhood morbidity and mortality, understanding inequities in congenital cardiac care is an important part of addressing and achieving the SDGs. Previous studies have determined possible causes for inequities in access to cardiac care in specific regions, but comparative reports are limited. Our study, therefore, aims to collate existing studies to provide a more holistic understanding of barriers to accessing congenital cardiac surgery in LMICs.
Through a qualitative systematic review, we identified preoperative, perioperative, and postoperative barriers that patients with CHD face in accessing surgical care in LMICs. In identifying and classifying challenges in accessing CHD in these settings, we hope to suggest potential solutions to major barriers that could be implemented in diverse contexts.
Material and Methods
The search was conducted according to the Preferred Reporting Items of Systematic Reviews and Meta-analyses (PRISMA) guidelines and encompassed Medline and CINAHL databases. It included E-pubs ahead of print, as well as in-process and in-data reviews. The search also included commentaries, editorials, review articles, journal articles, news articles, status reports, and studies with varying designs.
Search Criteria
With the assistance of a medical librarian, we implemented a search strategy that included strings of keywords, MeSH terms, and filters. In order to obtain barriers pertinent to present-day health care settings, the search criteria included results published from January 2000 to May 2021. We implemented the “LMIC Filters 2020” search hedge from Cochrane to include countries in the World Bank list of countries classified as low-income, lower-middle-income, and upper-middle-income. To search for articles regarding health care barriers in these areas, keywords such as “access,” “barriers,” “inequality,” and “equity,” as well as a combination of variations of these keywords were included in the search. MeSH terms regarding health care access such as “health policy,” “global health,” and “resource allocation” were used. The search strategy also included terms related to cardiac diseases such as “congenital heart defect,” “heart anomaly,” “tetralogy,” “ventricular septal defect,” and “atrial septal defect.”
Inclusion and Exclusion Criteria
Location: Articles with countries within the scope of the “Cochrane LMIC Filters 2020” were included. High-income countries were excluded.
Population: Articles involving patients with a form of congenital heart anomaly were included. Noncongenital conditions such as rheumatic heart disease or secondary cardiac complications due to other causes were not included.
Content: We included articles with discussion of barriers to accessing surgical services or inequities in surgical care for the population of interest. Search results which only mentioned barriers without further discussion of these subjects were excluded. Articles exclusively discussing medical management or patient outcomes unrelated to surgical treatments of CHDs were excluded. We excluded results which proposed strategies to improve health care access without identifying and discussing the barrier itself.
Language: We included results published in English or translated into English.
Data Extraction
The title and abstract were first screened independently by two reviewers (SC and KH). Discrepancies in decisions were resolved after discussion between the reviewers. This was followed by full-text screening, data extraction, and analysis. Risk of bias assessment was completed according to the PRISMA guidelines by two independent reviews (SC and KH).
We developed a novel and iterative framework for qualitative data extraction. Factors that prevented and delayed patients in accessing surgical care were classified as “preoperative,” “perioperative,” and “postoperative” barriers. Preoperative barriers were classified as factors preventing patients from obtaining a surgical consultation or arriving at a diagnosis, as well as affecting their ability to consent to or undergo surgery. Perioperative barriers included any challenges that interfered with surgical planning, execution, or safety. Finally, postoperative barriers encompassed all difficulties affecting the care and quality of life during recovery, follow-up, or successful transition to adult cardiac care.
Results
The search yielded 1,585 articles, of which 56 were duplicates and removed (Figure 1); 1,422 articles were excluded during title and abstract screening. A total of 107 articles underwent full-text screening. Of these, 67 satisfied all inclusion criteria and data were extracted.
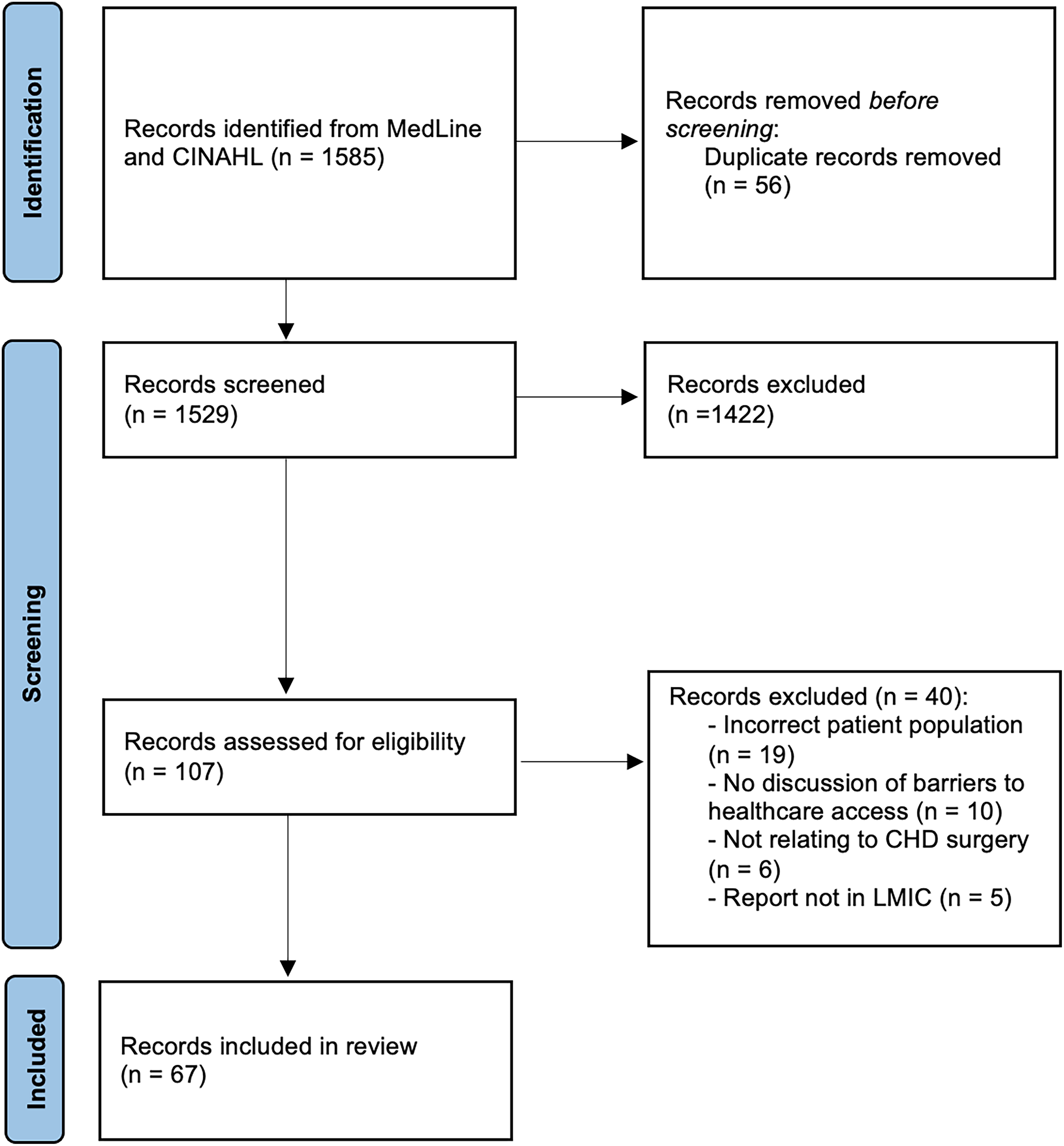
Preferred Reporting Items of Systematic Reviews and Meta-analyses (PRISMA) flow diagram of search results and reports excluded. Refer to Supplementary Table S1 for full list of included articles.
The 67 results spanned countries worldwide. Using the United Nations geoscheme classification system, 17 articles were from Southern Asia, 11 from Africa, 11 from Latin America and the Caribbean, 7 from South-eastern Asia, 4 from Western Asia, and 4 from Eastern Asia (Figure 2).
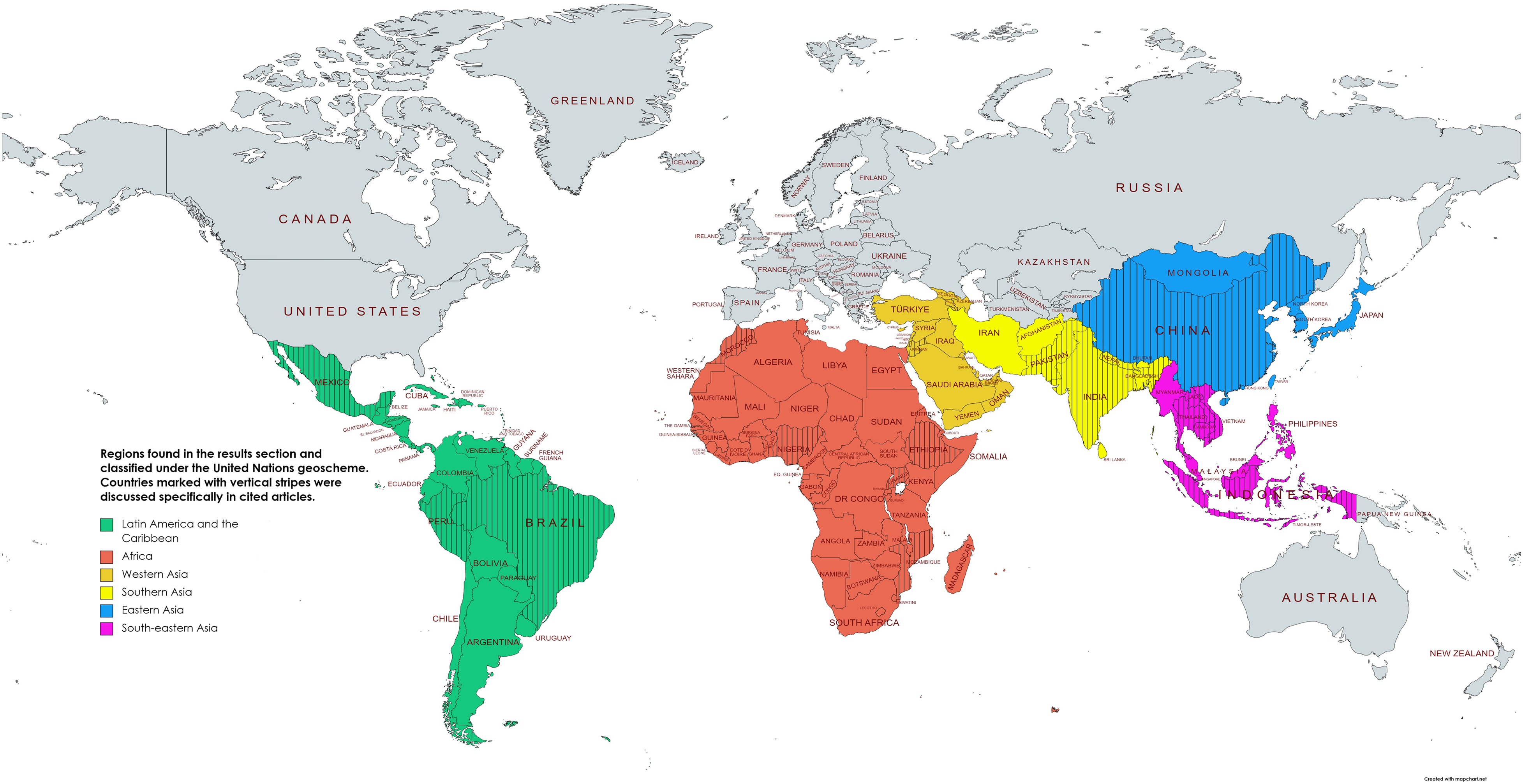
Regions and countries of records included in the study. Regions are classified using the United Nations geoscheme. Figure created using mapchart.net. Color image is available in the online version of the article.
Preoperative, Perioperative, and Postoperative Barriers
Preoperative barriers are summarized in Table 1. Barriers of note included themes of delayed diagnoses of CHD and sociocultural beliefs surrounding CHD. Some delayed diagnoses of CHD were identified to be due to increased rates of home deliveries without qualified personnel or equipment and lack of specialized workforce capable of identifying signs of CHD.3,4,6,10 From a social perspective, girls faced sex-based discrimination due to caregivers having concern with matrimonial prospects of their child with postoperative scars.3,4,9–11 As studies from India indicated, this can result in a lower percentage of girls undergoing CHD surgery as compared to boys.5,9 Under the theme of institutional-level barriers to access, maldistribution of resources by governing bodies was a major barrier to health care access for patients with CHD.
Themes, Subthemes, and Specific Examples of Preoperative Barriers in Accessing Congenital Heart Disease (CHD) Surgery.
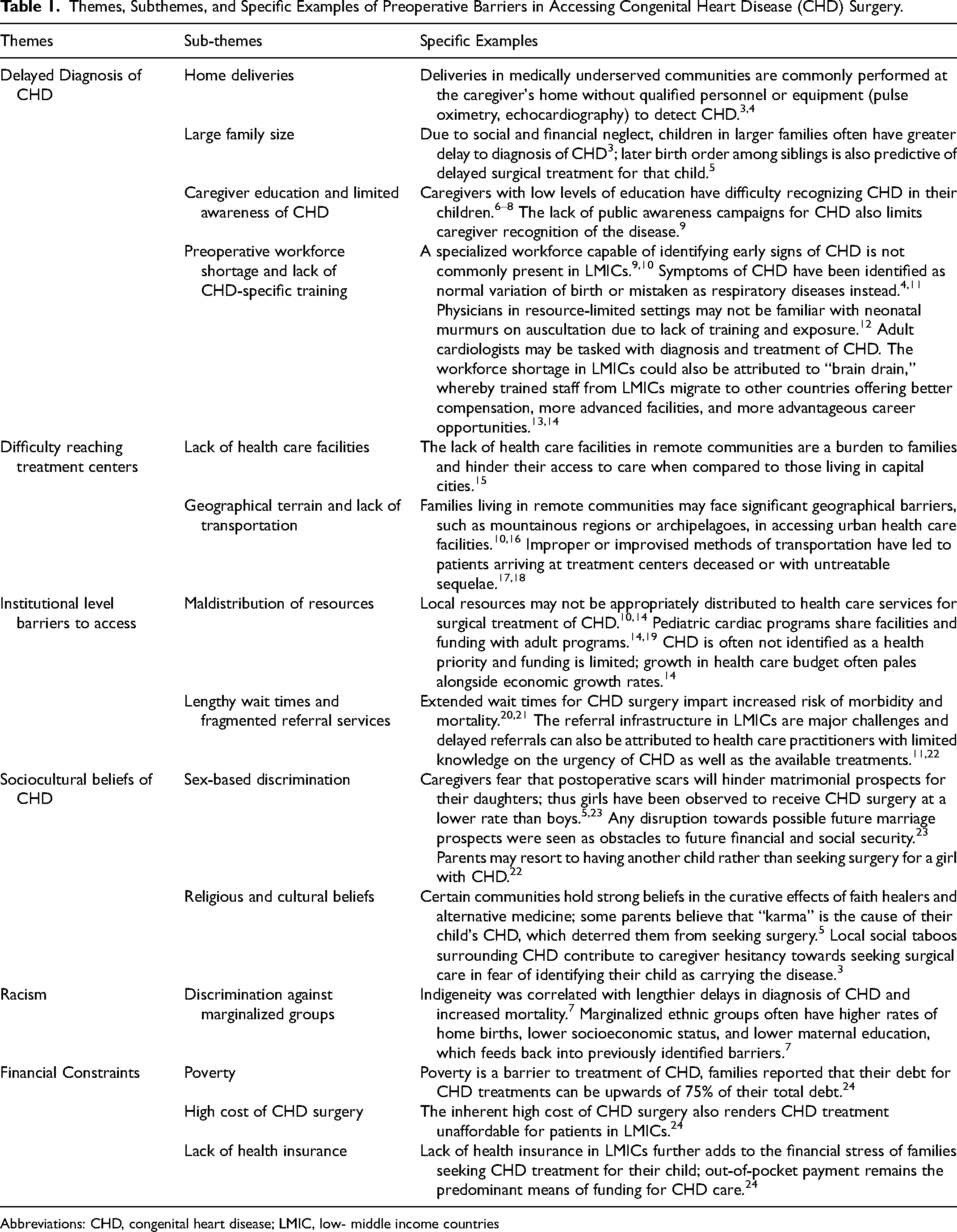
Abbreviations: CHD, congenital heart disease; LMIC, low- middle income countries
Perioperative barriers are outlined in Table 2. We found that a shortage of perfusionists, anesthesiologists or other trained anesthesia providers, and cardiac surgeons is frequently a barrier to patients accessing CHD surgical care. 25 Certain communities also may not have consistent supplies of electricity, water, or oxygen, which are necessary for surgery.26,27
Themes, Subthemes, and Specific Examples of Perioperative Barriers in Accessing CHD Surgery.
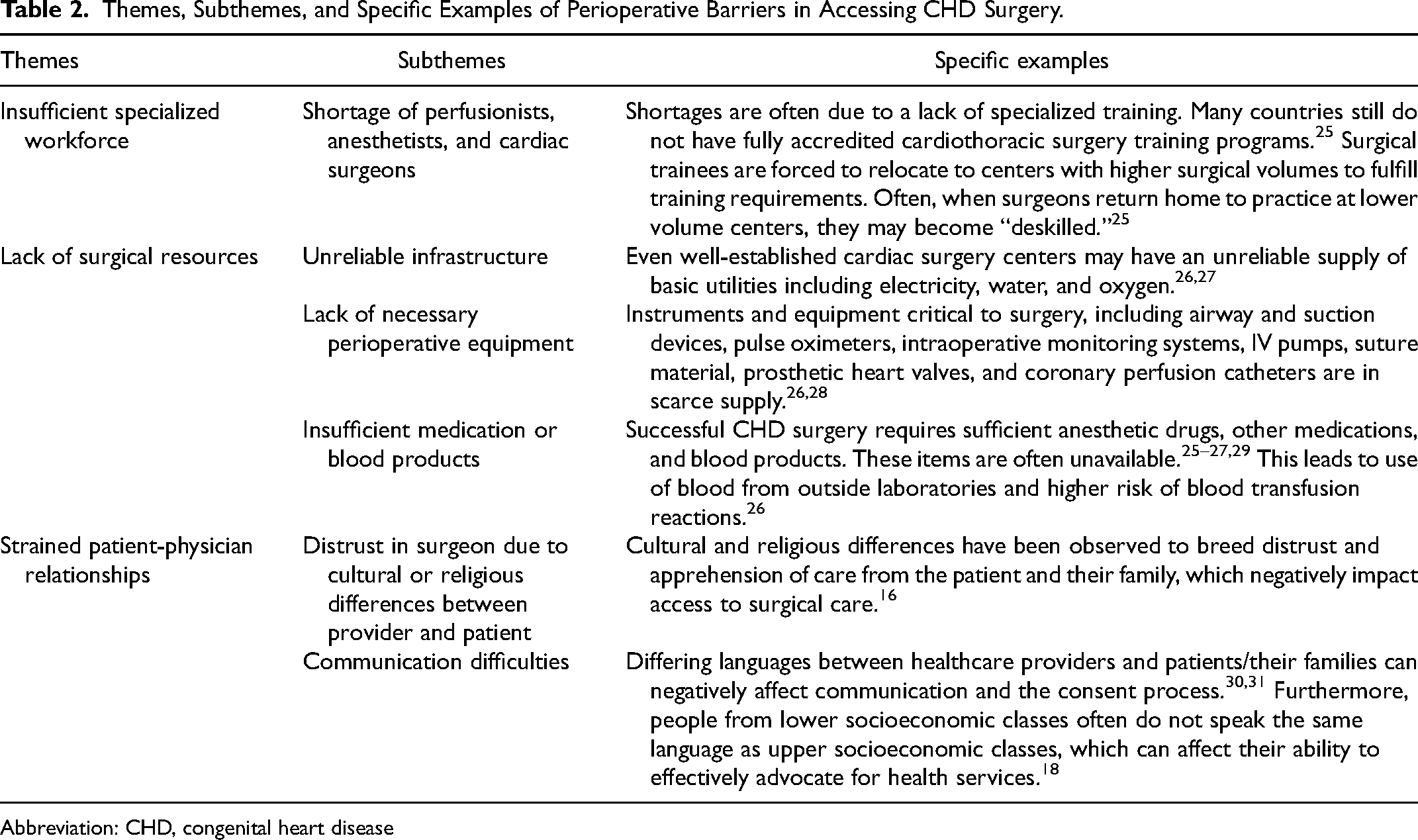
Abbreviation: CHD, congenital heart disease
Table 3 describes the postoperative barriers. Patients and families find it difficult to navigate postoperative care due to lack of appropriate caregiver counseling, in addition to social stigma from having undergone surgery. 23 Patients and families also often suffer negative economic consequences due to lengthy hospitalizations post-surgery.6,16 Hospitalization results in missed work for parents and families, as well as potentially lengthy absences from school.6,16,23 This burden summates with the accrued debt from costs due to the surgery, hospitalization, and any necessary relocation.6,16,23,36 Disjointed postoperative follow-up has negative consequences for children who may grow up and require life-long care for CHD. 35 Patients with ACHD often do not have specialized care to manage their unique long-term postoperative complications, such as arrhythmias and heart failure. Further, a lack of CHD registries preclude the ability to follow and study ACHD in the long term.9,35 Lastly, given the large number of children who survive into adulthood with CHD despite not having undergone surgery, there is a significant need to address the health care needs of ACHD, including with surgical intervention. 37
Themes, Subthemes, and Specific Examples of Postoperative Barriers in Accessing CHD Surgery.
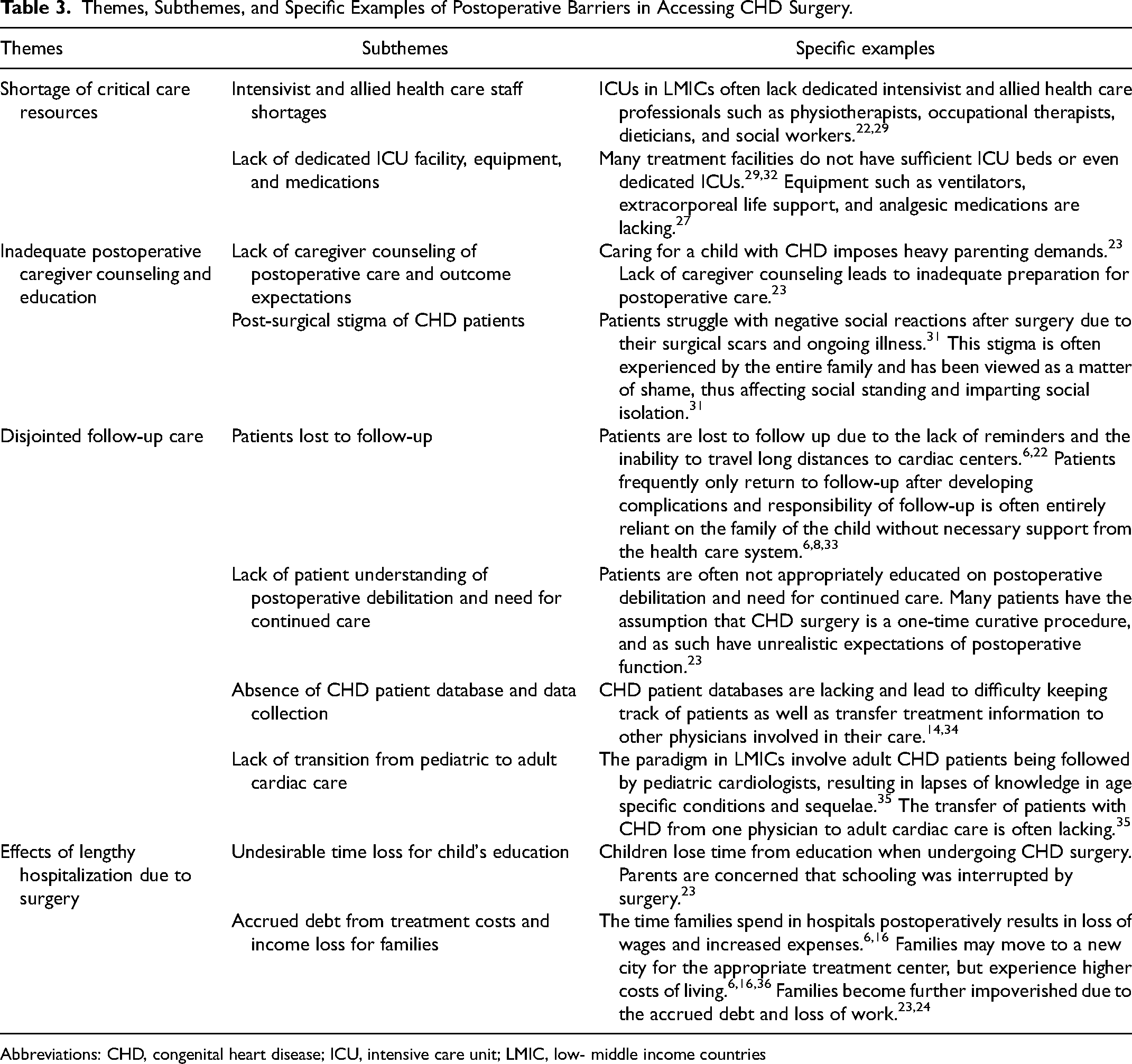
Abbreviations: CHD, congenital heart disease; ICU, intensive care unit; LMIC, low- middle income countries
Discussion
The global burden of CHD remains pressing, yet congenital heart surgery is not accessible for the majority of children and adults living with CHD globally. We identified 67 articles describing congenital heart surgery in LMICs, identifying common themes in terms of pre-, peri-, and postoperative barriers. The articles included ranged in publication from 2002 to 2021. When grouped into five-year categories, 12 were from 2002 to 2009, 43 were from 2010 to 2019, and 12 were from 2020 to 2021. Included articles described barriers to accessing care pertinent to the time periods around publication. Although formal statistical analysis could not be performed due to the heterogeneity of data and endpoints, informal qualitative review did not reveal associations between the time period and types of barriers described.
Notable preoperative barriers included delayed diagnosis, insufficient caregiver education, financial constraints, difficulty reaching treatment centers, sociocultural stigma of CHD, sex-based discrimination of patients with CHD, and Indigeneity (Table 1). Perioperative barriers included lack of hospital resources and workforce, need for prolonged hospitalization, and strained physician–patient relationships (Table 2). Many patients faced barriers postoperatively and into adulthood due to a shortage of critical care resources, inadequate caregiver counseling and patient education, lack of follow-up, and debt from hospital bills and missed work (Table 3). The multitude of barriers across the care continuum illustrates the complexity of congenital heart surgery and the need for health systems approaches to improve care for CHD.
Improving Early Detection
A high percentage of deliveries in LMICs occur at home or in under-equipped health centers. As such, detection and diagnosis of CHD are challenging without access to specialized physicians and necessary equipment, such as pulse oximetry.4,6,23 Delayed diagnoses of CHD lead to increased disease severity and translate to worsened prognosis and higher rates of complications during surgery. 11 Approximately one-half of patients with CHD with delayed diagnoses present with congestive heart failure at the onset of diagnosis. 11 Many studies from HICs have shown that pulse oximetry is an excellent method to screen for CHD in newborns. Indeed, pulse oximetry combined with physical examination remains a sensitive screening tool and a low-cost strategy to reduce delayed diagnoses of CHD in LMICs. To this end, Saxena et al found that the addition of pulse oximetry to clinical examination greatly improved sensitivity for detection of CHDs to between 75.5% and 84.6%. 38 Pulse oximetry is a particularly critical diagnostic tool for ductal-dependent CHDs, since most patients do not survive the newborn period unless they are promptly diagnosed and treated.6,38 However, the in context where pulse oximetry is unavailable, our review identified that engaging community health workers, nurses, medical officers, and midwives to recognize heart murmurs can enhance early screening for CHD.3,4,6,11,12,27,33,39,40 Zhao et al concluded that cardiac auscultation has a high sensitivity for identifying CHD and, in some situations, is as important as pulse oximetry in detecting CHD. 12 Therefore, a relatively simple intervention would be to ensure that health care providers who frequently see infants are trained in auscultation to offer postnatal screening for CHD in their community, especially when equipment such as pulse oximetry is not available. 12 Zhao et al acknowledged that it is challenging for generalist physicians, and even pediatricians, to determine the significance of murmurs by the location, timing, and characteristics of the murmur, especially in high-volume delivery centers. 12 However, Zhao et al's study suggests that detecting grade 2/6 or higher intensity murmurs successfully identifies major CHD with a sensitivity of 89.6%. 12
Resource Allocation
Although CHD represents 58% of the disability-adjusted life years (DALYs) due to congenital anomalies in LMICs, CHD care receives far less funding than diseases such as malaria, HIV/AIDS, and tuberculosis.13,41 Increasing funding for CHD surgical care is, therefore, critical to reducing DALYs in LMICs. Several countries have proposed strategies to mitigate costs for CHD surgery. In India, some hospitals have implemented subsidies for health care services for patients by utilizing funding from corporate social responsibility programs. 6 In Vietnam, all children under six years old undergoing most cardiac surgeries or catheter interventions in government hospitals fall under government insurance. 42 In rural China, Zhang et al proposed a cost-sharing protocol for CHD, whereby 50% of costs are covered by the current universal health insurance, 30% by the government, and 10% deduction of in-hospital bill covered by hospital medical relief foundations. 43 A shift in perspective to recognize that health care investments are also economic investments may also prove advantageous. 44 Indeed, Calderon-Colmenero et al found a 4% increase in a country's GDP for every 10% increase in life expectancy. 44 Unfortunately, many LMICs experience ongoing economic and political instability which leads to health care resource allocation assuming a lower priority. Understanding that access to CHD surgery may greatly avert DALYs lost may prove to be a helpful method for governing bodies with objective data as to where resources should be allocated. 44
It is important to note that even within the World Bank classification of “LMIC,” there exists a range of resource availabilities between countries. In the fiscal year 2020, the World Bank classified countries into various income groups utilizing Gross National Income (GNI) per capita. The various delineations are as follows: low-income country <$1025 GNI per capita; lower-middle income = $1026-$3995 GNI per capita; and upper middle-income = $3996-$12,375 GNI per capita. 45 This classification scheme highlights the large range of resource availability between groups—even between lower-middle and upper-middle income countries. Therefore, grouping countries together as LMICs makes it difficult to identify specific barriers relevant to each country's health care and economic context. Similarly, even regions within a country have different economic barriers. Thus, effective resource allocation strategies should be country or region-specific, and targeted toward their unique contexts. This can be accomplished through needs assessment studies prior to designing strategies to address health care barriers.
Deconstructing Sex-Based Discrimination
Despite increased attention to gender equality and empowering women, we found that sex-based discrimination was a notable barrier to accessing CHD care. 23 Discrimination toward women and girls reduces their access to basic needs as well as health care utilization. 23 Families may refuse CHD surgeries for girls because of the potential detriment that post-surgical scars have to their matrimonial prospects.5,23 Since marriage is viewed as a major source of social status mobilization and financial stability, families may opt to have another child rather than seek care for their daughter. 22 Some have suggested that education and literacy are important to deconstruct such stigma. 23 Promoting literacy and education for girls may be part of the solution.23,46 For example, the Indian state of Gujarat has implemented free education for girls and women, and it has subsequently provided them with greater vertical social mobility and into positions of power in the workplace. 46 This allows women to bring about the change in gender bias and this has been reflected in decreases in the gender gap for seeking medical care. 46 While these may be the ultimate and long-term solutions, immediate solutions involving subsidizing surgery costs for girls, monetary incentives, plastic surgery to improve postoperative scaring, or offering employment and education opportunities for female patients who underwent CHD surgery have been suggested. 5
Adult CHD
As the care for CHD improves, more children with CHD survive into adulthood. In HICs, more than 95% of children born with a CHD reach adulthood, resulting in the prevalence of ACHD surpassing pediatric CHD. 47 As CHD care remains insufficient across LMICs and premature mortality high, ACHD needs are poorly described and ACHD care is particularly lacking. It is estimated that there are approximately 150 ACHD centers in the United States, 17 in Canada, and 365 in Europe, whereas LMICs have only a fraction of those: most countries have either no ACHD center or one center catering to more than 40 million people.48,49 As a result, only a minority of adults with CHD in LMICs have received surgery or interventional cardiology despite their needs. Those who do receive care are often at risk of poorer outcomes compared compared with patients in HICs due to the complexity of ACHD presentations and a general lack of specialized training in ACHD. Indeed, in HICs, outcomes are worse for non-ACHD-trained surgeons compared with ACHD-trained surgeons. 50 Moreover, the transition of patients with CHD from childhood into adulthood often results in lost-to-follow-up despite the need for lifelong care. This is particularly problematic in LMICs, where electronic medical records and follow-up care are more limited and distances and barriers to tertiary care are larger.
Importance of Research for Solutions to Health Care Barriers
Clinical research and dissemination of information are critical to understanding CHD as well as informing policymakers of the required health care resources. The lack of research on CHD in LMICs hinders policymakers and health advocates to address barriers to health care access. 32 The burden of CHD is thought to be significantly higher than what is currently known, but the lack of data reduces urgency in the distribution of necessary resources and programs that could aid in CHD treatment and survivability. 32 Health professionals in LMICs may be unaware of the advances in treatment of CHD and as a result may counsel patients against interventions. 51 Research is paramount in order to ensure that pediatric hospitals can generate solutions to local problems, train local clinical experts, improve cost effectiveness of CHD treatment, and develop locally-sourced technology.52,53 The World Society for Pediatric and Congenital Heart Surgery encourages basic and clinical research in CHD across the world to form worldwide databases and increase collaboration between health care workers of different nations. This in turn can aid in knowledge transfer of solutions for health care accessibility issues. 54
Study Limitations
Limitations of our study include the small sample size of articles (n = 67), which is likely due to our relatively strict exclusion criteria. While the articles reviewed provide a good synopsis of the barriers to accessing congenital heart surgery in LMICs, we may not have captured all barriers. A scoping review that includes more databases and non-English language journals may result in a larger sample size. Another limitation of our review is that we limited the search to articles in English, which may have excluded perspectives published in non-English journals. This introduces an anglophone bias in our study and potentially misses studies in other languages frequently spoken in LMICs. Additionally, our study only captures views that have been reported; experiences of individuals from remote or otherwise marginalized communities may be underrepresented. While classifying barriers into preoperative, perioperative, and postoperative barriers, we noted that barriers rarely fall into one distinct category. Indeed, many barriers interact. For example, difficulty reaching treatment centers is classified as its own major theme but is interconnected with the socioeconomic status of families and number of treatment centers in a region. Lastly, our study also lacks first-hand perspectives from LMIC authors. This involvement may have provided context-specific knowledge and culturally sensitive insight.
Conclusion
Understanding the barriers that CHD patients face in accessing cardiac surgical care is a step toward decreasing neonatal and childhood mortality. Only after identifying the challenges that patients and families face in accessing care can we propose targeted solutions. Our thematic analyses grouped barriers into three categories. Preoperative barriers consisted of delayed diagnosis of CHD, difficulty reaching treatment centers, institutional-level barriers in health care, sociocultural beliefs surrounding CHD, racism, and financial constraints. Perioperative barriers consisted of insufficient specialized workforce, lack of surgical resources, and strained patient–physician relationships. Even after surgery, patients struggle with barriers such as shortage of critical care resources, inadequate caregiver counseling and education, disjointed follow-up care, and effects of lengthy hospitalization due to surgery. We propose several cross-cutting solutions to the aforementioned barriers, including task sharing, improved resource allocation, and deconstructing sex-based discrimination.
Supplemental Material
sj-docx-1-pch-10.1177_21501351231204328 - Supplemental material for Barriers to Accessing Congenital Heart Surgery in Low- and Middle-Income Countries: A Systematic Review
Supplemental material, sj-docx-1-pch-10.1177_21501351231204328 for Barriers to Accessing Congenital Heart Surgery in Low- and Middle-Income Countries: A Systematic Review by Samuel P.S. Cheng, Kayoung Heo, Emilie Joos, Dominique Vervoort and Shahrzad Joharifard in World Journal for Pediatric and Congenital Heart Surgery
Footnotes
Abbreviations
Acknowledgments
DV is supported by the Canadian Institutes of Health Research (CIHR) Vanier Canada Graduate Scholarship.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DV is a Board Member of the Global Alliance for Rheumatic and Congenital Hearts (Global ARCH).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.