
Abstract
Background
We aimed to analyze mid-term outcomes of the fenestrated Fontan procedure, focusing on the fenestration size.
Methods
We retrospectively reviewed the outcomes of the fenestrated Fontan procedure. Among 165 patients who underwent the Fontan procedure from 2011 to 2021, fenestration was created in 27 patients with the highest risks, including those with hypoplastic left heart syndrome, hypoplastic pulmonary arteries, heterotaxy syndrome with high pulmonary vascular resistance, and pulmonary arterial pressure >15 mm Hg. The patients underwent the procedure at a median age of three years (body weight, 11.4 kg; body surface area, 0.54 m2). Fenestration sizes were 3.5 to 5 mm.
Results
Spontaneous fenestration closure occurred within one year postoperatively in nine patients. Among them, three experienced Fontan failure, necessitating refenestration. Although fenestration size did not differ, the size corrected by body surface area at the time of surgery was smaller in patients with fenestration closure (6.4 mm/m2 vs 8.3 mm/m2, P < .05). Patients with a fenestration <7 mm/m2 were more likely to have fenestration closure within one year postoperatively, and those with a fenestration >9 mm/m2 were more likely to have severe desaturation and require home oxygen therapy following discharge.
Conclusions
Spontaneous fenestration closure affected the frequency of Fontan complications. A very small fenestration size corrected by body surface area was a significant risk factor for spontaneous closure. Conversely, a very large fenestration size corrected by body surface area resulted in severe desaturation. The optimal fenestration size to prevent early spontaneous closure and severe desaturation is approximately 8 mm/m2.
Keywords
Introduction
Postoperative mortality following the Fontan procedure remains high in patients with risk factors such as high pulmonary artery pressure, high pulmonary vascular resistance, and a complex anatomy, including heterotaxy syndrome with pulmonary venous obstruction and hypoplastic left heart syndrome (HLHS), predominantly due to elevated systemic venous pressure and decreased cardiac output.1–4 Fenestration of the Fontan circuit, first described in 1989, decreases postoperative morbidity and mortality rates in high-risk patients. 1 Such fenestration improves short-term outcomes by decreasing pleural drainage and hospital length of stay and reducing pulmonary pressure.5–7 However, introduction of the extracardiac conduit Fontan procedure is associated with the technical challenge of maintaining fenestration patency. 8 Reports suggest that 30% to 90% fenestrations close spontaneously, and 30% of these close within three months.9–12 Early spontaneous fenestration closure is problematic, particularly in high-risk Fontan patients 13 ; however, limited data are available on the factors influencing spontaneous fenestration closure.
The benefits of the fenestrated Fontan procedure come at the expense of lower systemic oxygenation in the early and late stages. Some reports suggest that patients with overly large fenestrations experience severe desaturation and require percutaneous intervention to reduce the fenestration size.14–17 Another unresolved question is how a large fenestration size influences desaturation in each patient. Therefore, this study analyzed mid-term outcomes following the fenestrated Fontan procedure with a focus on the association between fenestration size and risks of spontaneous fenestration closure or severe desaturation.
Patients and Methods
Ethical Statement
This research was approved by the Institutional Review Board (approval no.: 1524; approved on March 11, 2022). The requirement for written informed consent was waived because of the retrospective study design.
Patient Population and Data Collection
Between January 2011 and December 2021, 165 patients underwent the Fontan procedure at our institution. We retrospectively reviewed the clinical records of 27 consecutive high-risk patients who underwent the fenestrated Fontan procedure. In particular, we examined echocardiogram results, preoperative and postoperative cardiac catheterization findings, operative findings, and surgical outcomes.
Criteria for Fenestrated Fontan Procedure
We routinely create fenestration for patients who are undergoing high-risk Fontan procedures. High-risk patients included those with HLHS after the Norwood procedure associated with a severely hypoplastic pulmonary artery, those with heterotaxy syndrome with high pulmonary vascular resistance following correction of total anomalous pulmonary venous connection and/or worse than moderate atrioventricular valve regurgitation, those with pulmonary arterial pressure >15 mm Hg, and those with functional single-lung Fontan procedures. Moreover, we performed the fenestrated Fontan procedure for patients without fenestration who needed Fontan revision because of Fontan complications. A severely hypoplastic pulmonary artery was defined as a pulmonary artery with a pulmonary artery index <150 mm/m2 that was severely unbalanced such that the diameter of the smaller side was <50% of the diameter of the opposite side. Pulmonary vascular resistance was considered high when it was >3.0 Wood units·m2.
Surgical Technique
The surgical techniques for the Fontan procedure have been described elsewhere. 18 Extracardiac total cavopulmonary connection (EC-TCPC) was typically performed under conditions of cardiopulmonary bypass with aortic cross-clamping, cardioplegic electromechanical arrest, and mild systemic cooling. The inferior end of the graft was anastomosed to the inferior vena cava. A fenestration incision was made on the Fontan graft and the right atrial lateral wall; thus, a fenestration was created through direct side-by-side anastomosis without a bridging graft. Following the anastomosis completion, we clamped the graft superior to the fenestration site, declamped the aorta, and performed anastomosis of the superior end of the graft in the on-pump beating state. A transverse incision was made on the inferior aspect of the central branch pulmonary artery, and a Fontan graft was anastomosed to it. A polytetrafluoroethylene (PTFE) tube was used as the Fontan graft. The graft sizes used were 16, 18, or 20 mm, according to body size. The fenestration sizes were 3.5, 4, and 5 mm. The fenestration size was at the physician's discretion, considering body size and preoperative hemodynamic values; however, no objective criteria were followed. Fenestration of the Fontan graft was created with an aortic punch with the same size as the desired fenestration. We confirmed the size by measuring the punch hole on the Fontan graft before anastomosis with the lateral atrial wall. To prevent fenestration closure, we stitched the cut edge of the atrium onto the sequestered surface of the Fontan graft at least one-half a centimeter away from the edge of the punch hole, onto the flat surface of the Fontan graft.
Anticoagulation Regimen
Our anticoagulation regimen for patients undergoing the fenestrated Fontan procedure has been described previously. 19 The patients were continuously administered aspirin (initial dose: 5 mg/kg/d) and received combined administration of warfarin immediately after the procedure; that is, before hospital discharge. The prothrombin time-international normalized ratio (PT-INR) was controlled to 1.5 to 2.0. Warfarin administration was discontinued one year postoperatively.
Follow-Up
Follow-up included clinical examination, transthoracic echocardiography, and cardiac catheterization. Cardiac catheterization was performed to evaluate the hemodynamic situation of patients one year after the Fontan procedure and every five years thereafter. Catheter-based device closure of the fenestration was not performed. The indication of coiling for aortopulmonary collaterals (APCs) was enhancement of the pulmonary veins with contrast medium during aortography and a mean pulmonary artery pressure >15 mm Hg.
Endpoints
The primary endpoints were death, reoperation/Fontan failure (defined as Fontan takedown/revision/conversion), Fontan complications (protein-losing enteropathy, plastic bronchitis, arrhythmia, bleeding complications, thromboembolic complications, venovenous collaterals [VVCs]), and APCs. Aortopulmonary collateral data were gathered as nominal, dichotomous variables (coil embolization or not) without quantifying the magnitude. The secondary endpoint was fenestration closure within one year postoperatively. Echocardiography was used to assess whether the fenestration was open. The tertiary endpoint was severe desaturation at discharge after surgery and one-year postoperative cardiac catheterization. Severe desaturation was defined as the necessity of home oxygen therapy because of percutaneous oxygen saturation <85% in room air at discharge after the Fontan procedure and at cardiac catheterization one year postoperatively.
First, we compared patients with fenestration closure and those with fenestration patency at one year postoperatively to determine if any long-term outcomes were influenced by the fenestration patency. Subsequently, we compared patients with fenestration closure within one year postoperatively and patients with a persistently patent fenestration for one year postoperatively to determine preoperative factors associated with fenestration closure within one year.
Statistical Analysis
Statistical analysis was performed using PASW Statistics for Windows (version 18.0; SPSS Inc). Frequencies are presented as absolute numbers (percentages). Continuous data are presented as means ± standard deviations or medians (ranges), as appropriate. Mean values were compared using Student t test. Perioperative data were compared using χ2 test. Fisher exact test was used for categorical data. Pearson correlation analysis was used to assess the relationships between the Fontan graft size and body surface area (BSA), between the fenestration size and BSA, and between the fenestration size and Fontan graft size. The rates of freedom from death, reoperation/Fontan failure, Fontan complications, and APCs since the one-year postoperative cardiac catheterization were analyzed using Kaplan-Meier analysis. P < .05 was considered statistically significant.
Results
Patient demographic characteristics and intraoperative outcomes are shown in Table 1. Figure 1 shows the correlations of BSA with the Fontan graft size and fenestration size. Fontan tube size was correlated with BSA (r = 0.47 [95% confidence interval [CI], 0.30-0.62], P < .01), fenestration size was correlated with BSA (r = 0.34 [95% CI, 0.16-0.51], P < .01), and fenestration size was correlated with Fontan tube size (r = 0.18 [95% CI, 0.11-0.25], P = .03). No operative mortalities or deaths were observed during the hospital stay; however, two patients died during the follow-up period, one owing to HLHS and acute myocardial infarction at 1.9 years postoperatively, and the other owing to heterotaxy syndrome with total anomalous pulmonary venous connection and pulmonary venous obstruction at six months postoperatively. Reoperation was required for two patients who underwent Fontan revision and pulmonary venous obstruction release for heterotaxy syndrome with total anomalous pulmonary venous connection and one patient who underwent aortic valve replacement for HLHS with neo-aortic valve regurgitation. No cases of Fontan conversion or takedown occurred. Fontan complications, which included embolic stroke (n = 2), lung bleeding (n = 2), arrhythmia (n = 2), plastic bronchitis (n = 1), protein-losing enteropathy (n = 1), and VVCs (n = 1), occurred at a median of 21 months postoperatively (range, 4-90 months). Figure 2 shows the fenestration patency rate over time. Nine patients (33%) had fenestration closure within one year postoperatively. There was no difference in the rate of fenestration closure between each fenestration size. Percutaneous refenestrations were performed in three patients (Figure 3). One patient with HLHS and a severely hypoplastic pulmonary artery had fenestration closure and liver dysfunction at seven months postoperatively. One patient undergoing a single lung Fontan procedure had fenestration closure and plastic bronchitis at nine months postoperatively. One patient with tricuspid valve atresia and a severely hypoplastic pulmonary artery had fenestration closure and protein-losing enteropathy. Symptoms improved significantly in all three patients after percutaneous refenestration. At one year postoperatively, 21 patients showed fenestration patency, and six showed fenestration closure.
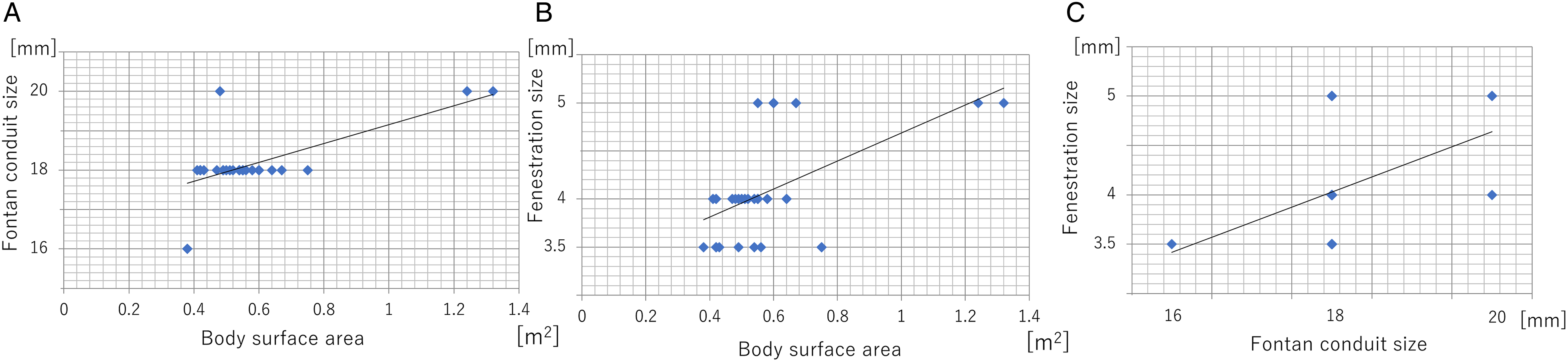
Correlations among body surface area, Fontan graft size, and fenestration size. (A) Between body surface area and Fontan graft size. (B) Between body surface area and fenestration size. (C) Between Fontan graft size and fenestration size.
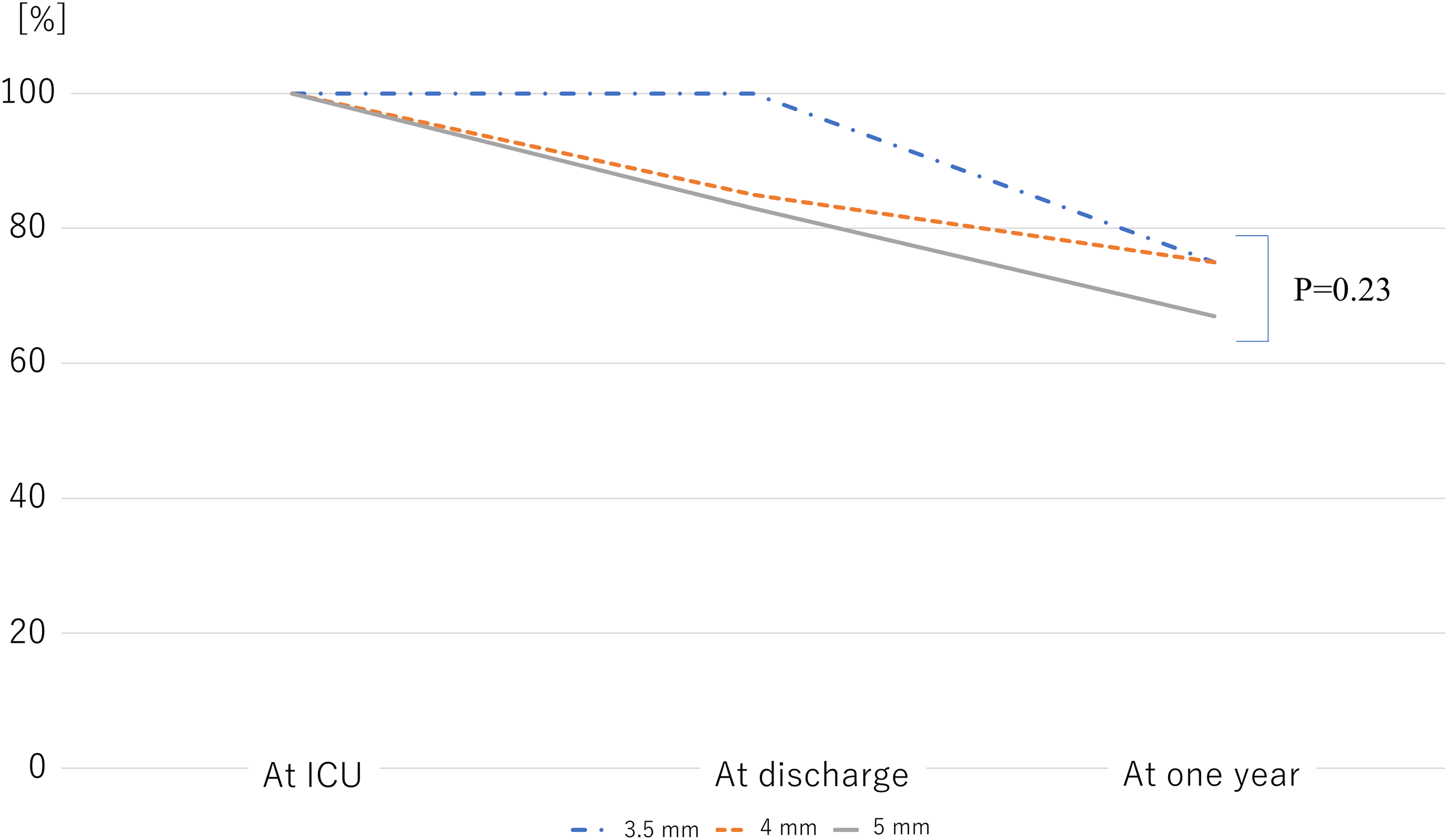
Fenestration patency rate over the postoperative time course. ICU, intensive care unit.

Postoperative time course until one year. EC-TCPC, extracardiac total cavopulmonary connection.
Demographic Characteristics and Intraoperative Outcomes.
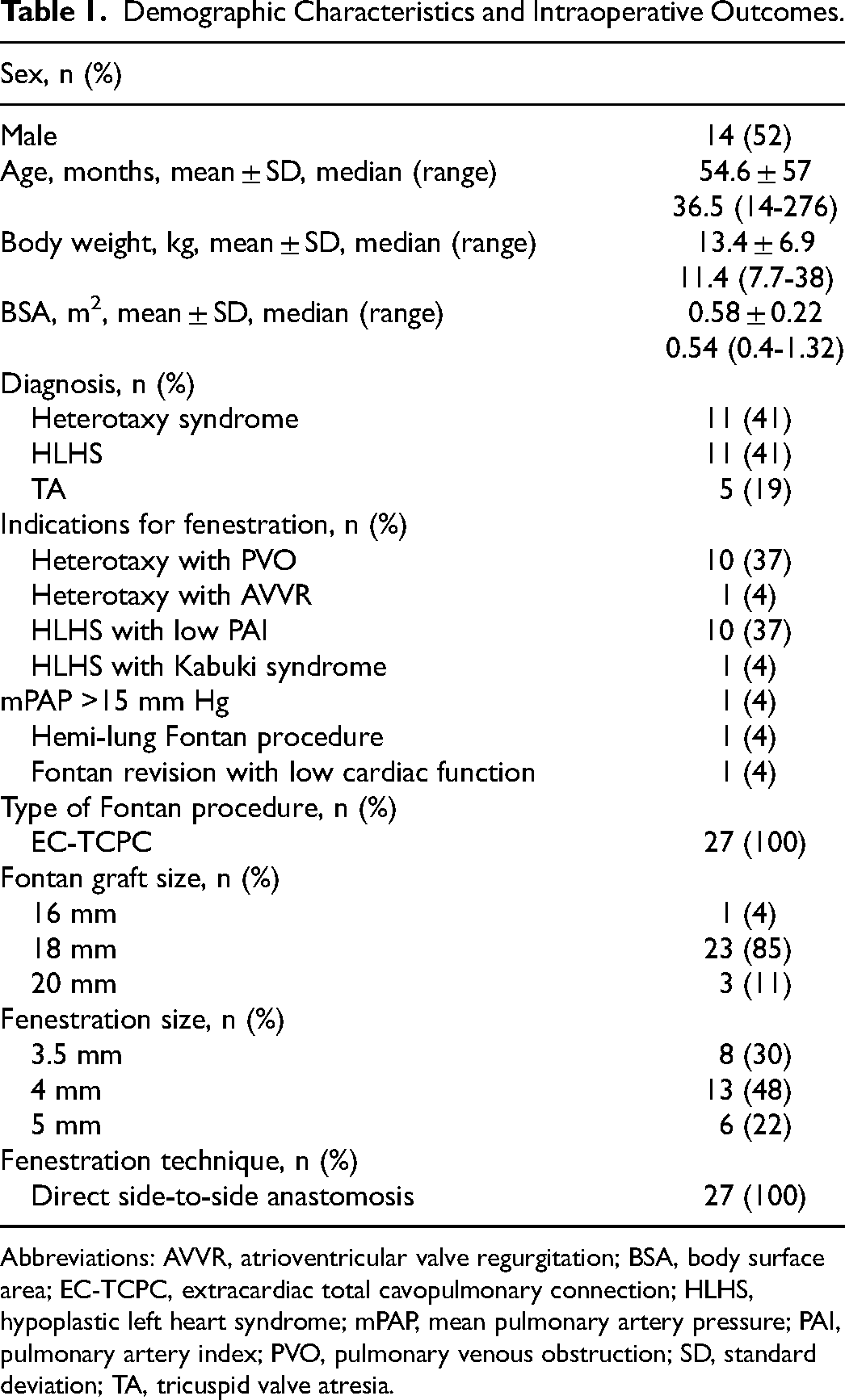
Abbreviations: AVVR, atrioventricular valve regurgitation; BSA, body surface area; EC-TCPC, extracardiac total cavopulmonary connection; HLHS, hypoplastic left heart syndrome; mPAP, mean pulmonary artery pressure; PAI, pulmonary artery index; PVO, pulmonary venous obstruction; SD, standard deviation; TA, tricuspid valve atresia.
Does the Patency of the Fenestration Improve Outcomes?
We compared 21 patients with a patent fenestration and six with fenestration closure at one year postoperatively. The median follow-up period after the one-year postoperative catheterization was 5 (0.9-11.0) years. One patient exhibited spontaneous fenestration closure at seven years (eight years postoperatively), with no Fontan complications. Catheter-based device closure of the fenestration was not performed for any patient. For patients with a patent fenestration, the rates of freedom from death were 100% and 78% at one and five years, respectively, and the rate of freedom from reoperation/Fontan failure was 100% at both 1 and 10 years. For patients with fenestration closure, the rate of freedom from death was 95% at both 1 and 10 years, while the rates of freedom from reoperation/Fontan failure were 100% and 75% at 1 and 10 years, respectively. The rates of freedom from death, reoperation/Fontan failure, or Fontan complications since one-year postoperative cardiac catheterization did not significantly differ between the groups (Figure 4A-C). However, the rate of freedom from coil embolization of APCs was significantly different between the two groups (P = .03) (Figure 4D). Additionally, for patients with fenestration patency, arterial oxygen saturation (SaO2; 85% vs 95%, P < .01) and the mean pulmonary artery pressure (12 mm Hg vs 14 mm Hg, P = .04) were significantly lower at the five-year postoperative cardiac catheterization (Table 2).
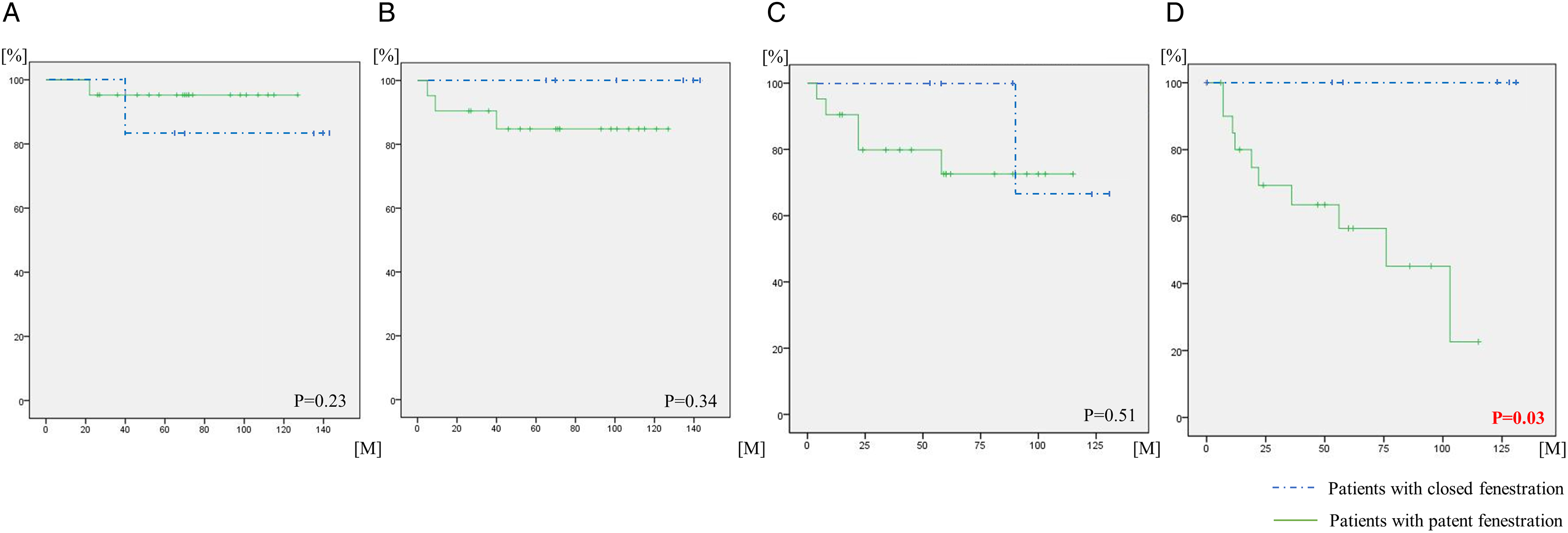
Rates of freedom from (A) death, (B) reoperation/Fontan failure (Fontan revision/conversion/takedown), (C) Fontan complications, and (D) coil embolization of APCs, analyzed using the Kaplan-Meier method. The dotted line represents patients with fenestrations that had already closed at one year postoperatively, while the solid line represents patients with patent fenestrations at one year postoperatively. The Kaplan-Meier curves start from the one-year postoperative cardiac catheterization time point. APCs, aortopulmonary collaterals.
Patency of the Fenestration and Outcomes.
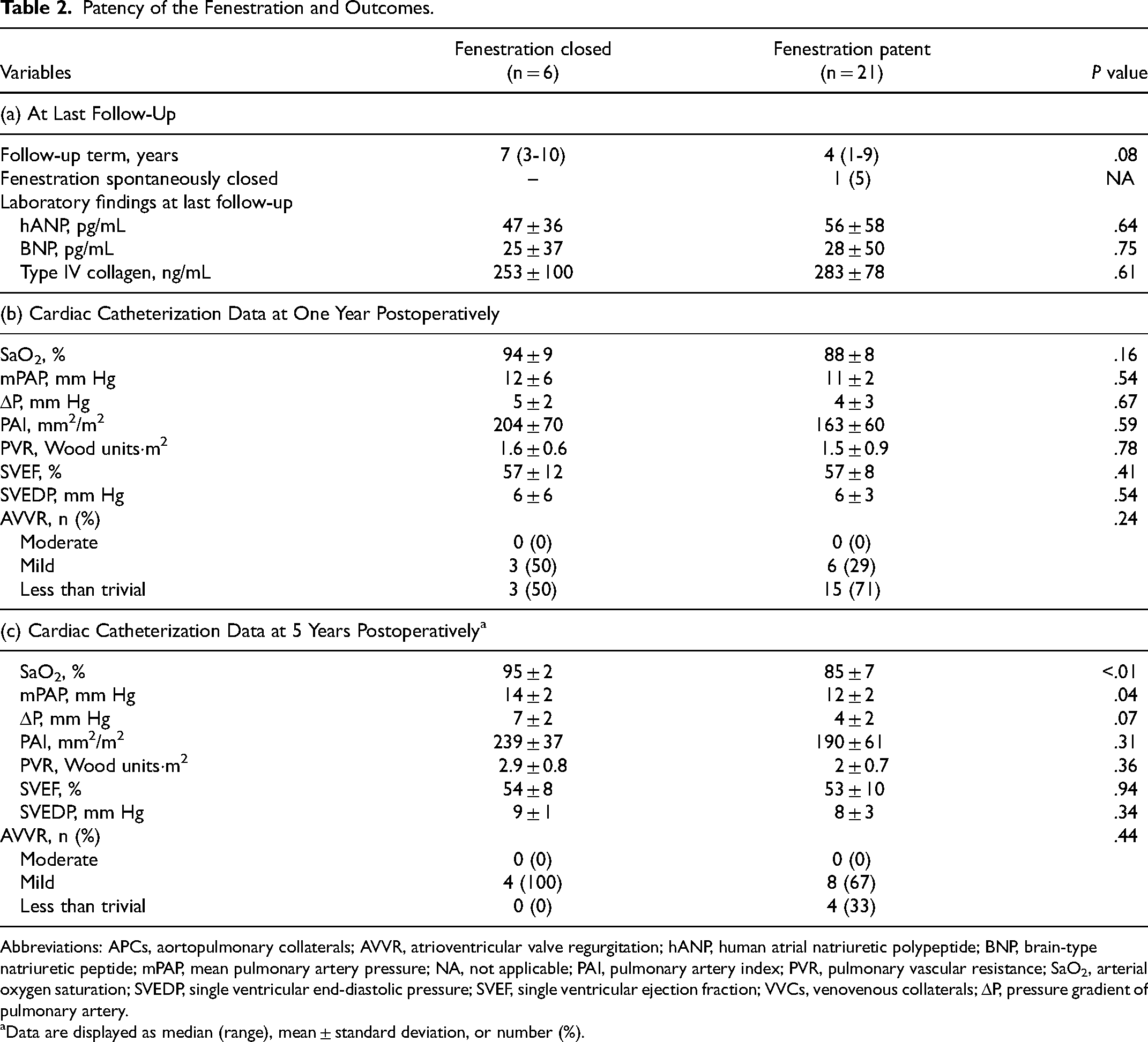
Abbreviations: APCs, aortopulmonary collaterals; AVVR, atrioventricular valve regurgitation; hANP, human atrial natriuretic polypeptide; BNP, brain-type natriuretic peptide; mPAP, mean pulmonary artery pressure; NA, not applicable; PAI, pulmonary artery index; PVR, pulmonary vascular resistance; SaO2, arterial oxygen saturation; SVEDP, single ventricular end-diastolic pressure; SVEF, single ventricular ejection fraction; VVCs, venovenous collaterals; ΔP, pressure gradient of pulmonary artery.
Data are displayed as median (range), mean ± standard deviation, or number (%).
Are There Any Factors Associated With Fenestration Closure?
We compared 18 patients with fenestration patency with 9 patients with fenestration closure at one year postoperatively. In patients with fenestration closure, the mean pulmonary vascular resistance was significantly lower (0.5 ± 1.2 Wood units·m2 vs 3.2 ± 1.1 Wood units·m2, P = .02) at the preoperative cardiac catheterization (Table 3). In terms of warfarin control, the mean PT-INRs in patients with fenestration closure and fenestration patency were 1.14 ± 0.11 at the time of the Fontan procedure and 1.19 ± 0.14 at one year postoperatively, respectively (P = .51).
Factors Associated With Patency of the Fenestration.a
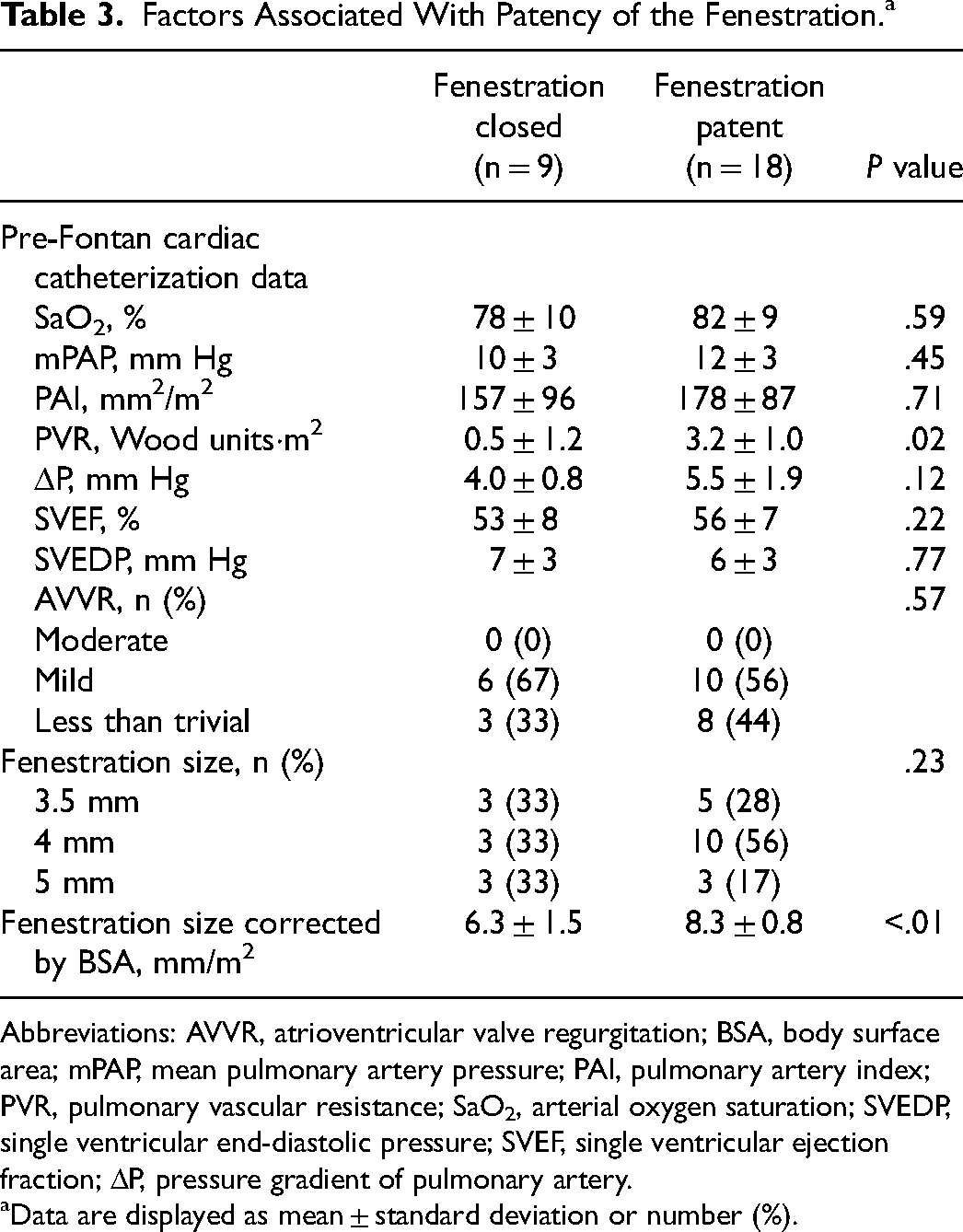
Abbreviations: AVVR, atrioventricular valve regurgitation; BSA, body surface area; mPAP, mean pulmonary artery pressure; PAI, pulmonary artery index; PVR, pulmonary vascular resistance; SaO2, arterial oxygen saturation; SVEDP, single ventricular end-diastolic pressure; SVEF, single ventricular ejection fraction; ΔP, pressure gradient of pulmonary artery.
Data are displayed as mean ± standard deviation or number (%).
Additionally, no differences were found in the fenestration size; however, the fenestration size corrected by BSA at the time of the Fontan procedure was associated with the rate of fenestration closure (Table 2).
Association Between Fenestration Size Corrected by BSA and Fenestration Closure/Severe Desaturation
Figure 5 shows the association between the fenestration size corrected by BSA during surgery and the rates of fenestration closure within one year postoperatively and severe desaturation at discharge after the Fontan procedure and at the one-year postoperative cardiac catheterization. When patients with a fenestration <7 mm/m2 (under seven group) were compared with those with a fenestration >7 mm/m2 (over seven group), the number of patients with fenestration closure was significantly higher in the under seven group (eight patients [100%] vs one patient [5%]; P < .01). In contrast, when patients were compared according to fenestration sizes of >9 mm/m2 (over nine group) and <9 mm/m2 (under nine group), the number of patients with severe desaturation was significantly higher in the over nine group (four patients [100%] vs one patient [4%]; P < .01).
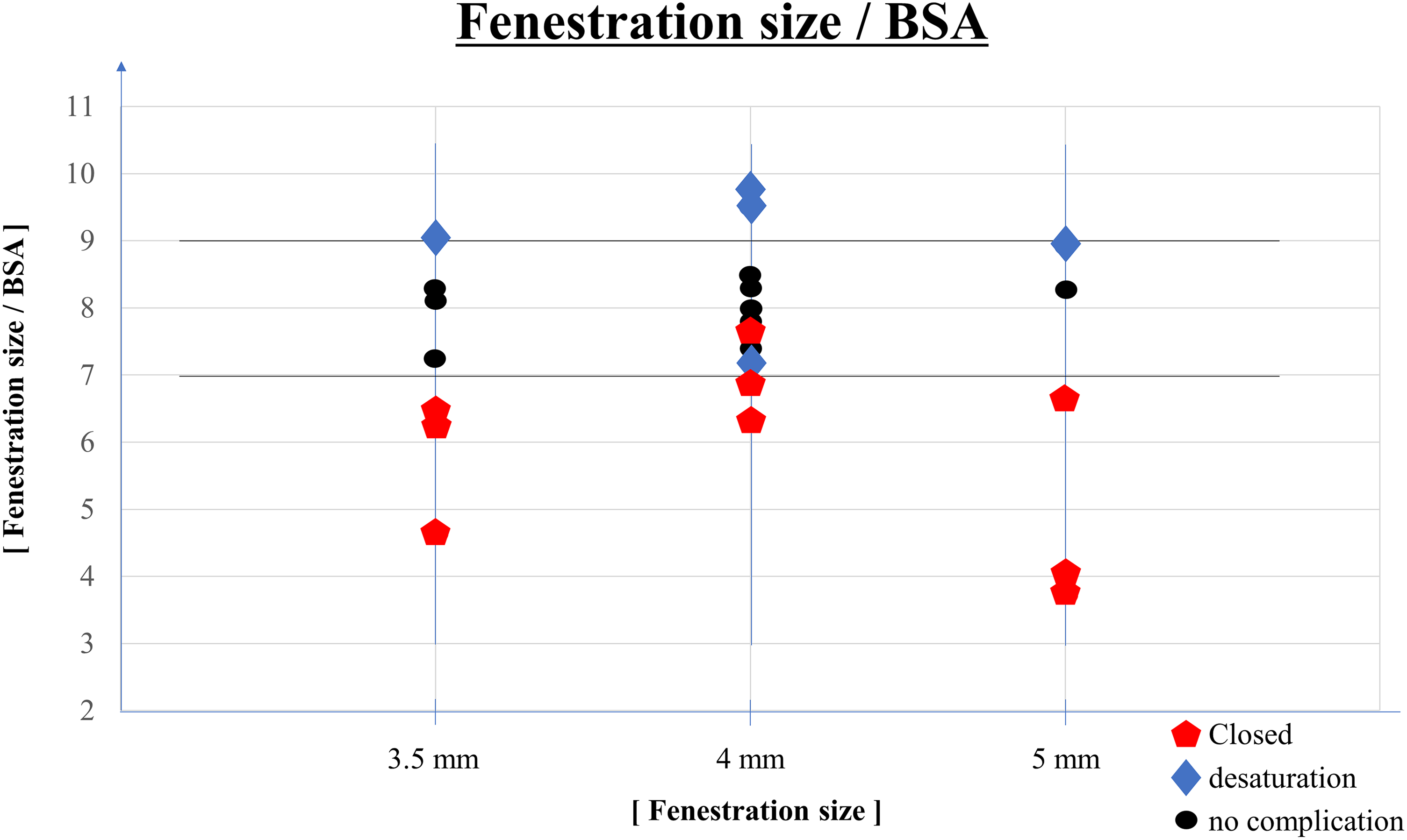
Associations of the fenestration size corrected by BSA at the time of the Fontan procedure with the rate of spontaneous fenestration closure within one year postoperatively and the rate of home oxygen therapy because of severe desaturation at discharge after the Fontan procedure and at the one-year postoperative cardiac catheterization. BSA, body surface area.
Comment
Fenestration Indication and Size Decision
Evidence regarding the use of fenestrations in the Fontan circuit is conflicting. Therefore, we have migrated to the selective use of fenestration with a very narrow range of indications reserved only for very high-risk patients. In recent studies, fenestrations for EC-TCPC were approximately 3 to 8 mm; however, these studies did not suggest criteria for fenestration size selection. 5 Fiore et al reported selection of fenestration size according to body weight (<15 kg, 5 mm; >15 kg, 6 mm; some patients with 4 mm); nonetheless, the rationale for using body weight as a means to select fenestration size was not provided. 12 In our institution, the first choice of fenestration size is 4 mm; however, we change it to 3.5 to 5 mm depending on body size and preoperative hemodynamic values. This is because the fenestration size and BSA are correlated. Because Fontan graft size was also decided depending on body size, the fenestration size and Fontan graft size were correlated.
Long-Term Fenestration Management
After catheter-based device fenestration closure, in addition to a predictable increase in arterial saturation, patients reportedly experienced improved exercise tolerance and better somatic growth and required fewer cardiac medications. 20 A patent fenestration and persistent cyanosis have been suggested to impair functional status and the potential for systemic embolization. Alternatively, other studies have indicated that, in patients undergoing catheter-based device closure of a fenestration, late fenestration closure results in increased arterial saturation but decreased cardiac output. However, the increase in SaO2 is insufficient to overcome the decrease in cardiac output; therefore, a decrease in systemic oxygen delivery is observed. 21 Studies also suggest that a patent fenestration is of long-term benefit to patients undergoing the Fontan procedure.22,23 Therefore, the necessity of fenestration closure remains controversial, and we do not perform catheter-based device closure of a fenestration unless it is absolutely necessary because our indications for fenestration are limited to patients with the highest risk. However, our results showed that long-term fenestration patency leads to desaturation and risk of APCs. More importantly, one patient died of myocardial infarction and two patients had a stroke during the follow-up period. Therefore, we may need to reconsider our long-term strategy regarding catheter-based device closure of a fenestration.
Incidence and Factors Influencing Fenestration Closure
Reports from different institutions indicated that 30% to 90% of fenestrations close spontaneously while approximately 30% close within three months.9–12 These institutions adopted fenestrations of 3 to 5 mm and a surgical technique with direct side-to-side anastomosis similar to that used in our institution. In our report, the rate of spontaneous fenestration closure was 33%, which is similar to that in these previous reports.
Among patients who undergo initial fenestration at the time of the Fontan procedure, those who experienced spontaneous fenestration closure before discharge had a significantly higher risk of hospital mortality, total mortality, Fontan failure, and complications, including extracorporeal membrane oxygenation use. 13 We also found many Fontan complications in patients with fenestration closure, and three patients underwent percutaneous refenestration within one year.
There are few reports on factors influencing the spontaneous closure of a fenestration. Gorla et al reported that patients with higher preoperative pulmonary vascular resistance and a history of postoperative systemic venous thromboembolism had a higher likelihood of persistent fenestration. 24 In our study, preoperative catheterization showed that patients with a higher preoperative pulmonary vascular resistance had a lower rate of spontaneous closure of the fenestration, similar to that in previous reports. In the study by Kotani et al, comparing three groups (catheter-based closure, spontaneous closure, and patency), the presence of an open fenestration was associated with the lowest survival and highest occurrence of Fontan complications. In contrast, the group with spontaneous fenestration closure had the best outcomes in terms of both mortality and morbidity. These results suggest that persistent fenestration is a marker of physiologic intolerance, even in cases with high pulmonary vascular resistance. 21
Regarding the blood coagulation test, the PT-INR was 1.2 ± 0.1, 1.4 ± 0.1, and 1.4 ± 0.1 at 1, 5, and 10 years after the Fontan procedure, respectively. This target certainly appears insufficient for patients with a fenestrated Fontan circuit, but no associations were found with the rate of fenestration closure. We previously reported that the PT-INR is difficult to control in patients who are administered warfarin, particularly during the early phase after TCPC. 19 In younger patients, the PT-INR varies easily, even with the same warfarin dose; therefore, patients need to undergo frequent blood tests for PT-INR assessment. However, this makes lifelong warfarin control challenging. 19
In terms of the surgical technique used for fenestration, many institutions have adopted direct side-to-side anastomosis, and the rates of spontaneous closure with this procedure are 30% to 60%. 5 Some reports suggest the possibility of a difference in the rate of spontaneous fenestration closure using surgical techniques.13,22,25 Ruiz et al reported that fenestration techniques using the interposition of a PTFE tube between the Fontan graft and the right atrial wall or a direct side-to-side anastomosis could crowd the anastomotic area with atrial muscle, and procedures that use a pericardial skirt might be associated with thrombus formation. 25 Kotani et al performed a similar technique with direct side-to-side anastomosis between the Fontan graft and the common atrial wall, which had a slightly higher spontaneous closure rate than did fenestration using a bridging PTFE tube, possibly because of right atrial trabeculation. 21 The proportion of spontaneous early fenestration closure was significantly higher in the EC-TCPC Fontan group than that in the lateral tunnel Fontan group (14% vs 4%; P < .01). 13 However, the optimal fenestration creation technique for the EC-TCPC Fontan procedure has not been reported. In our institution we perform only direct side-to-side anastomosis. To prevent fenestration closure, we suture at least half a centimeter of the cut edge of the atrium onto the sequestered surface of the Fontan graft, away from the edge of the punch hole, onto the flat surface of the Fontan graft. This is because a tunnel effect to the fenestration is obtained if too much of the atrium is picked up or if the atrium is bulky (which is not uncommon in a single ventricle) when performing direct side-to-side anastomosis because the atrial tissues impinge on the punch hole and result in an unreliable hole size.
In our study, although the rate of fenestration closure was not associated with fenestration size, the size corrected by BSA at the Fontan procedure was significantly smaller in these patients than that in patients with fenestration patency (6.4 mm/m2 vs 8.3 mm/m2, P < .05). However, patients with a fenestration <7 mm/m2 had fenestration closure.
Incidence and Factors Influencing Severe Desaturation in Patients Undergoing a Fenestrated Fontan Procedure
The fenestrated Fontan procedure poses a risk of desaturation in both the short and long terms. Regarding desaturation in the early phase, some reports suggest that patients with overly large fenestrations experience severe desaturation and need percutaneous intervention to reduce the fenestration size.14–17 These reports suggest that fenestration size and desaturation are associated. However, the unresolved question is how large a fenestration should be to influence desaturation in each patient. In our results, patients with a fenestration size corrected by BSA >9 mm/m2 had severe desaturation, necessitating home oxygen therapy. Regarding desaturation in the long term, some reports suggest that a significantly lower SaO2 persisted in patients undergoing a fenestrated Fontan procedure because fenestration was consequently transformed into VVCs. These caused significantly high pulmonary vascular resistance (hypoxia-induced vasoconstriction), leading to the growth of APCs. 20 In our study, the rate of APC growth was higher in patients with fenestration patency.
Limitations
This study had some limitations. First, it was a retrospective review of patients who underwent the fenestrated Fontan procedure in a single center. Second, the small sample size limited our ability to perform statistical adjustments. In this study, all patients underwent EC-TCPC, and the fenestration was limited to 3.5, 4, or 5 mm. Therefore, our results should be applied only to patients with a BSA of approximately 0.54 m2, an age of approximately three years, and who undergo EC-TCPC. Most studies on EC-TCPC, the most widely adopted variation of the Fontan procedure, included patients who were approximately three years of age, which is the same age as our study's patients, with fenestration sizes similar to ours (approximately 4 mm).4,13,24,26–30 Therefore, we believe that the results of this study may apply to many institutions. Third, the follow-up period for patients with fenestration closure might have been longer than that for patients with fenestration patency (P = .08); the results for the long-term outcomes influenced by fenestration patency might have been different if the follow-up periods for open and closed fenestrations were more similar. However, this limitation does not influence the key finding of this study; that is, the factors associated with fenestration closure within one year postoperatively.
Conclusion
Early fenestration closure may affect the frequency of postoperative adverse events, and too small a fenestration size corrected by BSA at the time of the Fontan procedure may present a risk of early closure. Conversely, too large a size corrected by BSA at the time of surgery may result in low SaO2. Therefore, to determine the optimal fenestration size it is crucial to consider BSA. According to this study, the optimal fenestration size is approximately 8 mm/m2 to prevent early spontaneous closure and severe desaturation.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.